You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Mark Klimek Notes 2Document42 pagesMark Klimek Notes 2Emerson Ocampo Alindogan93% (42)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Detroit Receiving Hospital Emergency Medicine Handbook 5th EdnDocument341 pagesDetroit Receiving Hospital Emergency Medicine Handbook 5th EdnElham Alsamahi100% (1)
- Advanced ICD Troubleshooting Part 2 PACE 2006 PDFDocument27 pagesAdvanced ICD Troubleshooting Part 2 PACE 2006 PDFSrajner PéterNo ratings yet
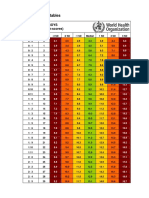
- Who Boys Rda + InterpretDocument34 pagesWho Boys Rda + InterpretrinaNo ratings yet
- A Case of Susac SyndromeDocument5 pagesA Case of Susac SyndromeBeny Pratama SidabutarNo ratings yet
- (Jurnal Inggris) Beny Pratama Sidabutar - 1061050117 - Penutupan Uteri Lapisan Tunggal Vs Lapisan Ganda Pada Operasi Bedah SesarDocument5 pages(Jurnal Inggris) Beny Pratama Sidabutar - 1061050117 - Penutupan Uteri Lapisan Tunggal Vs Lapisan Ganda Pada Operasi Bedah SesarBeny Pratama SidabutarNo ratings yet
- (Jurnal Inggris) Beny Pratama Sidabutar - 1061050117 - Penutupan Uteri Lapisan Tunggal Vs Lapisan Ganda Pada Operasi Bedah SesarDocument5 pages(Jurnal Inggris) Beny Pratama Sidabutar - 1061050117 - Penutupan Uteri Lapisan Tunggal Vs Lapisan Ganda Pada Operasi Bedah SesarBeny Pratama SidabutarNo ratings yet
- Kuliah Emergency Radiologi 2009Document32 pagesKuliah Emergency Radiologi 2009Beny Pratama SidabutarNo ratings yet
- A Rare Cause of Hearing Loss: Susac SyndromeDocument3 pagesA Rare Cause of Hearing Loss: Susac SyndromeBeny Pratama SidabutarNo ratings yet
- Topical and Systemic Therapies For Oral and Perioral Herpes SimplDocument6 pagesTopical and Systemic Therapies For Oral and Perioral Herpes Simplهناء همة العلياNo ratings yet
- StrokeDocument16 pagesStrokeDokdok DocNo ratings yet
- How To Control Atopic Dermatitis (2013)Document5 pagesHow To Control Atopic Dermatitis (2013)Beny Pratama SidabutarNo ratings yet
- Atopic Dermatitis Natural History, Diagnosis, and Treatment (2014) PDFDocument8 pagesAtopic Dermatitis Natural History, Diagnosis, and Treatment (2014) PDFBeny Pratama SidabutarNo ratings yet
- Stroke GordonDocument34 pagesStroke GordonBeny Pratama SidabutarNo ratings yet
- Ferne PDFDocument16 pagesFerne PDFBeny Pratama SidabutarNo ratings yet
- DD Tifoid (Morport 1)Document4 pagesDD Tifoid (Morport 1)Beny Pratama SidabutarNo ratings yet
- Chronic CareDocument37 pagesChronic CareBeny Pratama SidabutarNo ratings yet
- Mitochondrial Encephalomyopathy With Lactic Acidosis and Stroke-Like EpisodesDocument9 pagesMitochondrial Encephalomyopathy With Lactic Acidosis and Stroke-Like EpisodesBeny Pratama SidabutarNo ratings yet
- CancerDocument8 pagesCancerRhenofkunairNo ratings yet
- Pemeriksaan Radiologi Utk BMDDocument14 pagesPemeriksaan Radiologi Utk BMDBeny Pratama SidabutarNo ratings yet
- Bod CerebrovasculardiseasestrokeDocument67 pagesBod CerebrovasculardiseasestrokeErlin IrawatiNo ratings yet
- DD Tifoid (Morport 1)Document4 pagesDD Tifoid (Morport 1)Beny Pratama SidabutarNo ratings yet
- Ferne PDFDocument16 pagesFerne PDFBeny Pratama SidabutarNo ratings yet
- Bahan Referat-Treatment BMDDocument51 pagesBahan Referat-Treatment BMDBeny Pratama SidabutarNo ratings yet
- Clin Genet 2013 p109Document12 pagesClin Genet 2013 p109beny sidabutarNo ratings yet
- Cancer FactsDocument30 pagesCancer FactsArnold ApduaNo ratings yet
- Paul Et Al-2014-The Cochrane LibraryDocument180 pagesPaul Et Al-2014-The Cochrane LibraryBeny Pratama SidabutarNo ratings yet
- JofIMAB - 2015 21 4p895 900Document6 pagesJofIMAB - 2015 21 4p895 900beny sidabutarNo ratings yet
- Clin Exp Ophthalmol 2014 p4Document9 pagesClin Exp Ophthalmol 2014 p4beny sidabutarNo ratings yet
- Melatonin Protects Against Oxidative Stress in Granular Corneal Dystrophy Type 2 Corneal Fibroblasts by Mechanisms That Involve Membrane Melatonin Receptors.Document10 pagesMelatonin Protects Against Oxidative Stress in Granular Corneal Dystrophy Type 2 Corneal Fibroblasts by Mechanisms That Involve Membrane Melatonin Receptors.beny sidabutarNo ratings yet
- Humu 22601aDocument10 pagesHumu 22601aBeny Pratama SidabutarNo ratings yet
- Medicine MCQS JULY 2023 SOLVEDDocument15 pagesMedicine MCQS JULY 2023 SOLVEDLijo JoNo ratings yet
- Hopkins Medicine Review Cardiology SectionDocument54 pagesHopkins Medicine Review Cardiology SectiondrsalilsidhqueNo ratings yet
- Basic Ecg Interpretation Practice Test V 1Document7 pagesBasic Ecg Interpretation Practice Test V 1emmaaziz100% (1)
- BLS-ACLS AHA 2015 Update Hipgabi Jan 2018Document49 pagesBLS-ACLS AHA 2015 Update Hipgabi Jan 2018Anonymous Fws2pztNo ratings yet
- Bradycardia and TachycardiaDocument50 pagesBradycardia and Tachycardialiu_owen17No ratings yet
- Advanced Life Support (Training Manual)Document74 pagesAdvanced Life Support (Training Manual)Matt100% (25)
- Cardiac ArrythmiasDocument63 pagesCardiac ArrythmiasSankara SubramanianNo ratings yet
- Dysrhythmia TestsDocument3 pagesDysrhythmia TestsKimberly WhitesideNo ratings yet
- 10 Peri Arrest ArrhythmiasDocument39 pages10 Peri Arrest ArrhythmiasAnaid FourevaNo ratings yet
- MCQ ArrhythmiaDocument5 pagesMCQ ArrhythmiaDeepak KumarNo ratings yet
- Position Paper: A B C D e F G H CDocument11 pagesPosition Paper: A B C D e F G H CNico IonaşcuNo ratings yet
- Tachycardia AlgorythmDocument1 pageTachycardia AlgorythmUZNAPMNo ratings yet
- Ventricular FibrillationDocument3 pagesVentricular FibrillationsundarirakhmanNo ratings yet
- ACLS ECG Rhythm Strips Pretest Question Answers (Quiz) PDFDocument11 pagesACLS ECG Rhythm Strips Pretest Question Answers (Quiz) PDF김민길100% (1)
- Superimposed ECG PDFDocument93 pagesSuperimposed ECG PDFEdalyn CapiliNo ratings yet
- PHARMACILOGY SUMMryDocument16 pagesPHARMACILOGY SUMMryKathy Real VillsNo ratings yet
- CT 2Document16 pagesCT 2TGB LEGENDNo ratings yet
- Interpretasi EKG - Dr. HerickDocument189 pagesInterpretasi EKG - Dr. HerickDiana IdrisNo ratings yet
- Sample Nursing ExaminationsDocument58 pagesSample Nursing ExaminationsKars AtacadorNo ratings yet
- ECG (EKG) Examples and Quiz: Oxford Medical EducationDocument26 pagesECG (EKG) Examples and Quiz: Oxford Medical EducationMSNo ratings yet
- Defibrillation & DC Shock: Ns. Retno Setyawati, M.Kep., SP - KMBDocument34 pagesDefibrillation & DC Shock: Ns. Retno Setyawati, M.Kep., SP - KMBdanur ciyeeNo ratings yet
- Abstract Book INAACCDocument83 pagesAbstract Book INAACCrodtobingNo ratings yet
- Approach To WCT Seminar by GadisaDocument72 pagesApproach To WCT Seminar by GadisaGadisa DejeneNo ratings yet
- x8 x12 PM Spec SheetDocument22 pagesx8 x12 PM Spec SheetLizzy DuronNo ratings yet
- Instrument - Automated External DefibrillatorDocument2 pagesInstrument - Automated External DefibrillatorJulio ArgañarazNo ratings yet
- Sugiyono, S.Kep., Ners., M.KepDocument48 pagesSugiyono, S.Kep., Ners., M.KepHervin RamadhaniNo ratings yet