You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Finish LineDocument3 pagesFinish LineSgNo ratings yet
- Snake Bite: Abhija Babuji. Crri. Department of Pediatrics. SmimsDocument76 pagesSnake Bite: Abhija Babuji. Crri. Department of Pediatrics. SmimsMeliani FranzNo ratings yet
- RS5573 FONA 1000S User Manual 6476381 Ver2 201604 EN CN Reg SADocument36 pagesRS5573 FONA 1000S User Manual 6476381 Ver2 201604 EN CN Reg SAJuan carlos Isaza gNo ratings yet
- Microbiology: Pathogenic Gram-Positive Cocci (Streptococcus)Document26 pagesMicrobiology: Pathogenic Gram-Positive Cocci (Streptococcus)Shuler0071No ratings yet
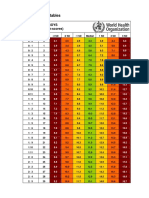
- Who Boys Rda + InterpretDocument34 pagesWho Boys Rda + InterpretrinaNo ratings yet
- (Jurnal Inggris) Beny Pratama Sidabutar - 1061050117 - Penutupan Uteri Lapisan Tunggal Vs Lapisan Ganda Pada Operasi Bedah SesarDocument5 pages(Jurnal Inggris) Beny Pratama Sidabutar - 1061050117 - Penutupan Uteri Lapisan Tunggal Vs Lapisan Ganda Pada Operasi Bedah SesarBeny Pratama SidabutarNo ratings yet
- Kuliah Emergency Radiologi 2009Document32 pagesKuliah Emergency Radiologi 2009Beny Pratama SidabutarNo ratings yet
- Resuscitation: European Resuscitation Council Guidelines 2021: Adult Advanced Life SupportDocument5 pagesResuscitation: European Resuscitation Council Guidelines 2021: Adult Advanced Life SupportBeny Pratama SidabutarNo ratings yet
- (Jurnal Inggris) Beny Pratama Sidabutar - 1061050117 - Penutupan Uteri Lapisan Tunggal Vs Lapisan Ganda Pada Operasi Bedah SesarDocument5 pages(Jurnal Inggris) Beny Pratama Sidabutar - 1061050117 - Penutupan Uteri Lapisan Tunggal Vs Lapisan Ganda Pada Operasi Bedah SesarBeny Pratama SidabutarNo ratings yet
- A Case of Susac SyndromeDocument5 pagesA Case of Susac SyndromeBeny Pratama SidabutarNo ratings yet
- A Rare Cause of Hearing Loss: Susac SyndromeDocument3 pagesA Rare Cause of Hearing Loss: Susac SyndromeBeny Pratama SidabutarNo ratings yet
- Stroke GordonDocument34 pagesStroke GordonBeny Pratama SidabutarNo ratings yet
- Topical and Systemic Therapies For Oral and Perioral Herpes SimplDocument6 pagesTopical and Systemic Therapies For Oral and Perioral Herpes Simplهناء همة العلياNo ratings yet
- How To Control Atopic Dermatitis (2013)Document5 pagesHow To Control Atopic Dermatitis (2013)Beny Pratama SidabutarNo ratings yet
- DD Tifoid (Morport 1)Document4 pagesDD Tifoid (Morport 1)Beny Pratama SidabutarNo ratings yet
- StrokeDocument16 pagesStrokeDokdok DocNo ratings yet
- Atopic Dermatitis Natural History, Diagnosis, and Treatment (2014) PDFDocument8 pagesAtopic Dermatitis Natural History, Diagnosis, and Treatment (2014) PDFBeny Pratama SidabutarNo ratings yet
- Ferne PDFDocument16 pagesFerne PDFBeny Pratama SidabutarNo ratings yet
- Mitochondrial Encephalomyopathy With Lactic Acidosis and Stroke-Like EpisodesDocument9 pagesMitochondrial Encephalomyopathy With Lactic Acidosis and Stroke-Like EpisodesBeny Pratama SidabutarNo ratings yet
- CancerDocument8 pagesCancerRhenofkunairNo ratings yet
- Pemeriksaan Radiologi Utk BMDDocument14 pagesPemeriksaan Radiologi Utk BMDBeny Pratama SidabutarNo ratings yet
- Bod CerebrovasculardiseasestrokeDocument67 pagesBod CerebrovasculardiseasestrokeErlin IrawatiNo ratings yet
- DD Tifoid (Morport 1)Document4 pagesDD Tifoid (Morport 1)Beny Pratama SidabutarNo ratings yet
- Ferne PDFDocument16 pagesFerne PDFBeny Pratama SidabutarNo ratings yet
- Bahan Referat-Treatment BMDDocument51 pagesBahan Referat-Treatment BMDBeny Pratama SidabutarNo ratings yet
- Clin Genet 2013 p109Document12 pagesClin Genet 2013 p109beny sidabutarNo ratings yet
- Cancer FactsDocument30 pagesCancer FactsArnold ApduaNo ratings yet
- Paul Et Al-2014-The Cochrane LibraryDocument180 pagesPaul Et Al-2014-The Cochrane LibraryBeny Pratama SidabutarNo ratings yet
- JofIMAB - 2015 21 4p895 900Document6 pagesJofIMAB - 2015 21 4p895 900beny sidabutarNo ratings yet
- Clin Exp Ophthalmol 2014 p4Document9 pagesClin Exp Ophthalmol 2014 p4beny sidabutarNo ratings yet
- Melatonin Protects Against Oxidative Stress in Granular Corneal Dystrophy Type 2 Corneal Fibroblasts by Mechanisms That Involve Membrane Melatonin Receptors.Document10 pagesMelatonin Protects Against Oxidative Stress in Granular Corneal Dystrophy Type 2 Corneal Fibroblasts by Mechanisms That Involve Membrane Melatonin Receptors.beny sidabutarNo ratings yet
- Humu 22601aDocument10 pagesHumu 22601aBeny Pratama SidabutarNo ratings yet
- RRL Mental IllnessDocument1 pageRRL Mental IllnessGaguka NamanNo ratings yet
- Rubber Band Ligation: of HaemorrhoidsDocument1 pageRubber Band Ligation: of HaemorrhoidsdbedadaNo ratings yet
- Biology Investigatory Project On Caffeine AddectionDocument5 pagesBiology Investigatory Project On Caffeine AddectionShivam SinghNo ratings yet
- Glass Prescription - SutrishnaDocument15 pagesGlass Prescription - SutrishnaSutrishna PramanikNo ratings yet
- C-Reactive Protein: TurbilatexDocument1 pageC-Reactive Protein: TurbilatexAssane Senghor100% (1)
- 9650-0301-01 Rev. MDocument48 pages9650-0301-01 Rev. MCarlos AndresNo ratings yet
- Spinal SurgeryDocument19 pagesSpinal SurgerySalomeSibashviliNo ratings yet
- Teknik Operasi Splenektomi 2Document31 pagesTeknik Operasi Splenektomi 2sphericalfaNo ratings yet
- Hirschsprung's Disease, PDFDocument1 pageHirschsprung's Disease, PDFMr. LNo ratings yet
- Pulsion Work Booklet: Bucarest Hemodynamic Monitoring WorkshopDocument43 pagesPulsion Work Booklet: Bucarest Hemodynamic Monitoring WorkshopghuoiNo ratings yet
- Chamani Essay VAPEDocument2 pagesChamani Essay VAPEChamani MadawalaNo ratings yet
- World No-Tobacco DayDocument2 pagesWorld No-Tobacco DayAkankshaNo ratings yet
- Gastric GavageDocument3 pagesGastric GavageRico Delgado of WorldbexNo ratings yet
- Requires Ongoing Support From Your Service: A Heart AttackDocument2 pagesRequires Ongoing Support From Your Service: A Heart AttackBîrlădeanu VlăduţNo ratings yet
- Which Hard Tissue Augmentation Techniques Are The Most Succesful in Furnishing Bony Support For Implant PlacementDocument25 pagesWhich Hard Tissue Augmentation Techniques Are The Most Succesful in Furnishing Bony Support For Implant PlacementJuan Andres CastilloNo ratings yet
- Effect of Periodontal Therapy On C-Reactive Protein Levels in Gingival Crevicular Fluid of Patients With Gingivitis and Chronic PeriodontitisDocument5 pagesEffect of Periodontal Therapy On C-Reactive Protein Levels in Gingival Crevicular Fluid of Patients With Gingivitis and Chronic PeriodontitisKanagavalli VijayakumarNo ratings yet
- English Task The Summery of Health Illness, Part of The Body, Medical Practicioners, Oncology and X-Ray & CT ScanDocument7 pagesEnglish Task The Summery of Health Illness, Part of The Body, Medical Practicioners, Oncology and X-Ray & CT ScanYudha HupayantiNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailssumandeepNo ratings yet
- Papanicolaou StainDocument1 pagePapanicolaou StainRitam JoarderNo ratings yet
- Abnormal Psychology Movie ReviewDocument3 pagesAbnormal Psychology Movie ReviewAthirah NarawiNo ratings yet
- FibromaDocument3 pagesFibromaAsiyath HNo ratings yet
- DM 2021-0114 Guidelines On The MGMT and Admin of The Initial 600,000 Donated SARS-CoV-2 Vaccine (Vero Cell) Inactivated Coronavac (Sinovac) DosesDocument17 pagesDM 2021-0114 Guidelines On The MGMT and Admin of The Initial 600,000 Donated SARS-CoV-2 Vaccine (Vero Cell) Inactivated Coronavac (Sinovac) DosesRalph Julius MendozaNo ratings yet
- Difference Between Serum and PlasmaDocument2 pagesDifference Between Serum and PlasmaCynthia Adeline SNo ratings yet
- Health Lesson Plan-BandagesDocument8 pagesHealth Lesson Plan-BandagesJaybee MacadangdangNo ratings yet
- 2) Megaloblastic AnemiaDocument17 pages2) Megaloblastic AnemiaAndrea Aprilia100% (1)
- Antenatal Care Services: by DR - Chinedu Ibeh Thursday, 16 APRIL 2015Document81 pagesAntenatal Care Services: by DR - Chinedu Ibeh Thursday, 16 APRIL 2015SehaRizaNo ratings yet