You might also like
- Human Robot InteractionDocument418 pagesHuman Robot InteractionEduardo Andres GerleinNo ratings yet
- Cse V Software Engineering (10is51) SolutionDocument45 pagesCse V Software Engineering (10is51) Solutionbharaths100No ratings yet
- Software Project Management Walker RoyceDocument101 pagesSoftware Project Management Walker Roycehina rani100% (2)
- PQT LG Lk-0525ccDocument229 pagesPQT LG Lk-0525ccGerardo Zamorano100% (2)
- UserManual 703Document733 pagesUserManual 703Gaetano GaetanoNo ratings yet
- Leveson, Applying Systems SafetyDocument17 pagesLeveson, Applying Systems SafetypirotteNo ratings yet
- When Bad Things Happen To Good Leaders Firing Back From Career Disasters PDFDocument7 pagesWhen Bad Things Happen To Good Leaders Firing Back From Career Disasters PDFkNo ratings yet
- System Safety EngineeringDocument4 pagesSystem Safety Engineeringaugur886No ratings yet
- Shell Moerdijk Cast Nancy LevesonDocument78 pagesShell Moerdijk Cast Nancy LevesonСергей МазеинNo ratings yet
- Human Error - in The LoopDocument3 pagesHuman Error - in The Loopsl1828No ratings yet
- Batch Process Playbook - by Automation World - 2013Document101 pagesBatch Process Playbook - by Automation World - 2013Rick VellNo ratings yet
- The ML Test Score: A Rubric For ML Production Readiness and Technical Debt ReductionDocument10 pagesThe ML Test Score: A Rubric For ML Production Readiness and Technical Debt ReductionDinesh BhatiaNo ratings yet
- Whitepaper - State of Platform Engineering ReportDocument18 pagesWhitepaper - State of Platform Engineering ReportElton LewisNo ratings yet
- Monitoring Software Requirements Using Instrumented CodeDocument10 pagesMonitoring Software Requirements Using Instrumented CodeAbdallah GhannamNo ratings yet
- 1software Engineering - Lect#1Document18 pages1software Engineering - Lect#1Shozab SohailNo ratings yet
- 5@introduction To Software EngineeringDocument60 pages5@introduction To Software Engineeringshreya saxenaNo ratings yet
- An Overview of Software EngineeringDocument12 pagesAn Overview of Software EngineeringDomsmasherNo ratings yet
- Introduction To Software Session1Document23 pagesIntroduction To Software Session1G. SiddardhaNo ratings yet
- Chap 1. An Introduction To Software Engineering: © Ian Sommerville 2006 Slide 1Document87 pagesChap 1. An Introduction To Software Engineering: © Ian Sommerville 2006 Slide 1Jerome BañariaNo ratings yet
- Software Engineering ReviewerDocument10 pagesSoftware Engineering ReviewerReign Alysa VillanuevaNo ratings yet
- Introduction To Software Session1Document23 pagesIntroduction To Software Session1mauryaamit2062No ratings yet
- What Is Software EngineeringDocument30 pagesWhat Is Software Engineeringshiv_kaushik9No ratings yet
- Chapter 1 IntroductionDocument64 pagesChapter 1 IntroductionMr. Nitin Jain (SET Assistant Professor)No ratings yet
- UNIT1 Introductionpptx 2024 01 25 08 03 17Document92 pagesUNIT1 Introductionpptx 2024 01 25 08 03 17garvishabajadejaNo ratings yet
- Topics Covered: Lesson 6Document3 pagesTopics Covered: Lesson 6Srawan NathNo ratings yet
- Lecture 1 - SW Testing-Background, IEEE StdsDocument20 pagesLecture 1 - SW Testing-Background, IEEE StdsLOW QZHI YEE UnknownNo ratings yet
- Maintenance Application User Guide - Issue DDocument44 pagesMaintenance Application User Guide - Issue DRonald N Meza CNo ratings yet
- Session 1 - Nature of SWDocument20 pagesSession 1 - Nature of SWGVachaspathi gnaneswarNo ratings yet
- SE UNIT-1,2 Combined VCEDocument36 pagesSE UNIT-1,2 Combined VCEAryan AdlaNo ratings yet
- Software Engineering OverviewDocument62 pagesSoftware Engineering OverviewShariar Parvez TonmoyNo ratings yet
- Unit 1Document61 pagesUnit 1Parth PatelNo ratings yet
- Software Challenges in Achieving Space SafetyDocument15 pagesSoftware Challenges in Achieving Space SafetyAnonymous mE6MEje0No ratings yet
- Introductory LectureDocument30 pagesIntroductory Lecturebhavik jainNo ratings yet
- SE Unit 1Document14 pagesSE Unit 1surajsl308No ratings yet
- Topics Covered: Professionals Software DevelopmentDocument8 pagesTopics Covered: Professionals Software DevelopmentMuhammad SyukronNo ratings yet
- Chapter 1 - Introduction To Software EngineeringDocument31 pagesChapter 1 - Introduction To Software Engineeringhamious.9293No ratings yet
- Unit 1. SEPM LectureDocument191 pagesUnit 1. SEPM LectureSimi JainNo ratings yet
- Unit-1 - New - FinalDocument75 pagesUnit-1 - New - Finalchat GPTNo ratings yet
- Se Unit-1 Material 2021Document32 pagesSe Unit-1 Material 2021iron manNo ratings yet
- Introduction To Software EngineeringDocument30 pagesIntroduction To Software EngineeringRustin FariolenNo ratings yet
- Maintenance Application User Guide - Issue EDocument48 pagesMaintenance Application User Guide - Issue EDarko LekicNo ratings yet
- Software and Software Engineering: Software Engineering: A Practitioner's Approach, 6th EditionDocument19 pagesSoftware and Software Engineering: Software Engineering: A Practitioner's Approach, 6th Editiongopi_meruguNo ratings yet
- هندسة برامجياتDocument78 pagesهندسة برامجياتrayan alkurdiNo ratings yet
- Software Characteristics AreDocument1 pageSoftware Characteristics AreAvinash KumarNo ratings yet
- 1st ClassDocument24 pages1st ClassjayaprasannaNo ratings yet
- Acfrogacm4483xyaze5jn Mpxc4qtcmneugufbxfopgadwjziy3u0unvapdn8qzml8zejrkkg JH Cpbi7adhjgiecvzzegdkkeolj Rgf31 Lgymvxlwswy0lfufxomib0m6ucrt 5brad7j51rDocument26 pagesAcfrogacm4483xyaze5jn Mpxc4qtcmneugufbxfopgadwjziy3u0unvapdn8qzml8zejrkkg JH Cpbi7adhjgiecvzzegdkkeolj Rgf31 Lgymvxlwswy0lfufxomib0m6ucrt 5brad7j51rRana YesmeenNo ratings yet
- Software Reliability: AbstractDocument18 pagesSoftware Reliability: Abstract9890189067No ratings yet
- Cap 10Document21 pagesCap 10tuk hwNo ratings yet
- System Software SafetyDocument15 pagesSystem Software SafetyHosein AlaviNo ratings yet
- Evolve Role of SoftwareDocument19 pagesEvolve Role of Softwareleo_thammuNo ratings yet
- TestingConcepts 1Document41 pagesTestingConcepts 1xyzparog0000No ratings yet
- Introduction To Software EngineeringDocument32 pagesIntroduction To Software Engineeringsameen khanNo ratings yet
- Ch1 IntroductionDocument87 pagesCh1 IntroductioncddchenNo ratings yet
- Lecture 13 - 22 Software Testing - Black Box TestingDocument57 pagesLecture 13 - 22 Software Testing - Black Box Testingi201770 Zeerak ZubairNo ratings yet
- Module 5 Software Redundancy-ShortDocument48 pagesModule 5 Software Redundancy-ShortynjuanNo ratings yet
- SE Lecture Notes Unit 1Document43 pagesSE Lecture Notes Unit 1Lokesh WaradeNo ratings yet
- Figure 1.1 Failure Curve For Hardware Figure 1.2 Failure Curves For SoftwareDocument5 pagesFigure 1.1 Failure Curve For Hardware Figure 1.2 Failure Curves For SoftwareJohn Dustin SaintsNo ratings yet
- Software Engineering Chapter 2Document49 pagesSoftware Engineering Chapter 2nitin guptaNo ratings yet
- Software Engineering: Slide Set 01: Introduction To Software and Software EngineeringDocument67 pagesSoftware Engineering: Slide Set 01: Introduction To Software and Software EngineeringHusnain AhmedNo ratings yet
- Fmea OverviewDocument26 pagesFmea OverviewDavid MartinNo ratings yet
- SE Unit1 20IT3302Document20 pagesSE Unit1 20IT3302santhoshkumpatla76No ratings yet
- 19 Elliott CASTAnalysisOfTheBuncefieldIncidentDocument13 pages19 Elliott CASTAnalysisOfTheBuncefieldIncidentСергей МазеинNo ratings yet
- MIT16 63JS16 LecNotes6Document61 pagesMIT16 63JS16 LecNotes6Сергей МазеинNo ratings yet
- CAST Tutorial 2016Document84 pagesCAST Tutorial 2016Сергей МазеинNo ratings yet
- Thomas - A New Systems Theoretic Approach To SafetyDocument37 pagesThomas - A New Systems Theoretic Approach To SafetyСергей МазеинNo ratings yet
- Systems Theoretic Process Analysis STPA v9 v2 SanDocument71 pagesSystems Theoretic Process Analysis STPA v9 v2 SanСергей МазеинNo ratings yet
- FRAM/STPA: Hazard Analysis Method For FRAM ModelDocument17 pagesFRAM/STPA: Hazard Analysis Method For FRAM ModelСергей МазеинNo ratings yet
- Mallya Archana 2015october MASc STPA ISODocument124 pagesMallya Archana 2015october MASc STPA ISOСергей МазеинNo ratings yet
- Fleming Thesis STECADocument231 pagesFleming Thesis STECAСергей МазеинNo ratings yet
- 2015 STECA TutorialDocument92 pages2015 STECA TutorialСергей МазеинNo ratings yet
- Important Mcq-Switchgear ProtectionsDocument14 pagesImportant Mcq-Switchgear ProtectionsNeil Cal100% (1)
- Lect-2 Lexical ConventionsDocument20 pagesLect-2 Lexical ConventionsSahil SharmaNo ratings yet
- Durlum India PVT Ltd-GOVT - PresentationDocument28 pagesDurlum India PVT Ltd-GOVT - PresentationS S RAWATNo ratings yet
- Chapter 10 - Threads and The Pthread LibraryDocument47 pagesChapter 10 - Threads and The Pthread LibraryAlexNo ratings yet
- EE 213 Fundamentals of Electric CircuitsDocument7 pagesEE 213 Fundamentals of Electric CircuitsIan Christopher CahuloganNo ratings yet
- Math Corrproblems 2019Document4 pagesMath Corrproblems 2019weng paraleNo ratings yet
- AE 231 Thermodynamics Week 3 Week 3: Instructor: Assoc. Prof. Dr. Sinan EyiDocument47 pagesAE 231 Thermodynamics Week 3 Week 3: Instructor: Assoc. Prof. Dr. Sinan EyiOnur ÖZÇELİKNo ratings yet
- Thematic Exploration of Digital, Social Media, and Mobile Marketing PDFDocument34 pagesThematic Exploration of Digital, Social Media, and Mobile Marketing PDFMario Yamid Gil MuñozNo ratings yet
- Unit-1: Dynamics K1 Level Questions Multiple Choice QuestionsDocument21 pagesUnit-1: Dynamics K1 Level Questions Multiple Choice QuestionsBabitha DhanaNo ratings yet
- Whamo User Manual 3.0Document259 pagesWhamo User Manual 3.0bhanu prasadNo ratings yet
- Co., LTD.: WH4004A Character 40x4Document1 pageCo., LTD.: WH4004A Character 40x4Andi FebriantoNo ratings yet
- Chapters: 10 Date: Total Marks: 30 TimeDocument2 pagesChapters: 10 Date: Total Marks: 30 TimeseakanugaNo ratings yet
- Computer Aided Drug DesigningDocument19 pagesComputer Aided Drug DesigningPitchumaniangayarkanni S.No ratings yet
- A Review of Encapsulation of Carotenoids Using Spray Drying and Freeze DryingDocument27 pagesA Review of Encapsulation of Carotenoids Using Spray Drying and Freeze DryingVanja ŠeregeljNo ratings yet
- Orca Datasheet PDFDocument11 pagesOrca Datasheet PDFaze2010No ratings yet
- Becknam-Ref VrednostiDocument44 pagesBecknam-Ref VrednostialisaNo ratings yet
- Lesson 1Document13 pagesLesson 1Kristine Lorraine MateoNo ratings yet
- Moment of Inertia of Cracked SectionDocument26 pagesMoment of Inertia of Cracked SectionChung-silMbunkoueKundaNo ratings yet
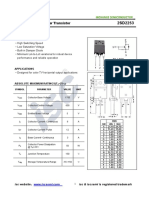
- Isc 2SD2253: Silicon NPN Power TransistorDocument2 pagesIsc 2SD2253: Silicon NPN Power TransistorFrancisco Meza BenavidezNo ratings yet
- Glossory of CompositeDocument125 pagesGlossory of CompositeIshfaq AhmadNo ratings yet
- Applications of Artificial Neural Networks For ECG Signal Detection and ClassificationDocument15 pagesApplications of Artificial Neural Networks For ECG Signal Detection and ClassificationsridharparthipanNo ratings yet
- Operating System Cit333Document124 pagesOperating System Cit333Muhammad HamidNo ratings yet
- Fishing Tools Services Catalog SchlumbergerDocument39 pagesFishing Tools Services Catalog Schlumbergeralvaro_massimoNo ratings yet
- Chapter 1 Research Methods-OverviewDocument24 pagesChapter 1 Research Methods-Overviewkassahun meseleNo ratings yet
- Unit 2 (Finite Transformation)Document28 pagesUnit 2 (Finite Transformation)Meenakshi PriyaNo ratings yet
- Dae Cit-1 RevisedDocument57 pagesDae Cit-1 RevisedSaad AliNo ratings yet
- HP Compaq d530 PDFDocument48 pagesHP Compaq d530 PDFDanny Catalan100% (1)
- Software-Defined Network Function Virtualization A SurveyDocument12 pagesSoftware-Defined Network Function Virtualization A Surveyjainam lathiyaNo ratings yet