You might also like
- Self Discovery MaterialsDocument62 pagesSelf Discovery Materialsarojutony100% (8)
- Job Safety Analysis (Hydro Jetting)Document4 pagesJob Safety Analysis (Hydro Jetting)rashid zaman57% (7)
- Dry Needling For Female Chronic Pelvic Pain A.3Document9 pagesDry Needling For Female Chronic Pelvic Pain A.3amnatul khairiNo ratings yet
- Body Back Buddy ManualDocument11 pagesBody Back Buddy ManuallyleNo ratings yet
- The Original Backnobber II Tool: User GuideDocument37 pagesThe Original Backnobber II Tool: User GuideAl BnNo ratings yet
- The End of Poverty - Jaffrey SachsDocument32 pagesThe End of Poverty - Jaffrey SachsPulkit GargNo ratings yet
- Applied Kinesiology Collected Papers 2001-2006Document124 pagesApplied Kinesiology Collected Papers 2001-2006Huib Salomons80% (10)
- M W M K C W S e P P S: R C TDocument10 pagesM W M K C W S e P P S: R C TDaniel GuevaraNo ratings yet
- A Structured Physiotherapy Treatment Model Can Provide Rapid Relief To Patients Who Qualify For Lumbar Disc Surgery: A Prospective Cohort StudyDocument8 pagesA Structured Physiotherapy Treatment Model Can Provide Rapid Relief To Patients Who Qualify For Lumbar Disc Surgery: A Prospective Cohort StudyQuiroprácticaParaTodosNo ratings yet
- Jmu 26 194Document6 pagesJmu 26 194Arkar SoeNo ratings yet
- 0Document11 pages0kang soon cheolNo ratings yet
- 7405 15461 1 SMDocument9 pages7405 15461 1 SMMuhammad AbdullahNo ratings yet
- Effectiveness of Myofascial Release and Muscle Energy Technique On Pectoralis Minor Length in Subjects With Shoulder Impingement Syndrome A Comparative StudyDocument10 pagesEffectiveness of Myofascial Release and Muscle Energy Technique On Pectoralis Minor Length in Subjects With Shoulder Impingement Syndrome A Comparative StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pillastrini 2016Document41 pagesPillastrini 2016alonsoNo ratings yet
- 291-297 Jopct1Document7 pages291-297 Jopct1efi hudriahNo ratings yet
- Bowen Back Pain WSN-93-2018-81-94Document14 pagesBowen Back Pain WSN-93-2018-81-94Saleha TariqNo ratings yet
- Conventional Therapy Versus Positional Release Technique in The Treatment of Chronic Low Back DysfunctionDocument7 pagesConventional Therapy Versus Positional Release Technique in The Treatment of Chronic Low Back DysfunctionEmad Eldin Mohamed AbdelatiefNo ratings yet
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and ResearchMuhamad BenyaminNo ratings yet
- ArchRheumatol 33 418Document6 pagesArchRheumatol 33 418qwerty hrNo ratings yet
- This Item Is The Archived Peer-Reviewed Author-Version ofDocument12 pagesThis Item Is The Archived Peer-Reviewed Author-Version ofK scuddsNo ratings yet
- Castrogiovanni 2016Document14 pagesCastrogiovanni 2016carlos corteNo ratings yet
- 1 s2.0 S0003999319303892 MainDocument8 pages1 s2.0 S0003999319303892 MainRizkyrafiqoh afdinNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyhfhfhNo ratings yet
- To_Compare_the_Effects_of_Maitland_MobilizationDocument4 pagesTo_Compare_the_Effects_of_Maitland_MobilizationravichandragoudaNo ratings yet
- Physiotherapy: P. Ratan Khuman Lourembam Surbala Priyanka Patel Dhara ChavdaDocument4 pagesPhysiotherapy: P. Ratan Khuman Lourembam Surbala Priyanka Patel Dhara ChavdaSahithya MNo ratings yet
- UntitledDocument7 pagesUntitledElizabeth VivancoNo ratings yet
- Treating Lumbar SpondylosisDocument10 pagesTreating Lumbar SpondylosisDiyya Awaliah Nurhakiimah IbrahimNo ratings yet
- International Journal of Osteopathic Medicine: Jacob Marten Switters, Stefan Podar, Luke Perraton, Zuzana MachotkaDocument8 pagesInternational Journal of Osteopathic Medicine: Jacob Marten Switters, Stefan Podar, Luke Perraton, Zuzana MachotkaElizabeth VivancoNo ratings yet
- To Analyse The Short Term Effect of Upper Trapezius Inhibition Taping in Patients With Mechanical Neck PainDocument8 pagesTo Analyse The Short Term Effect of Upper Trapezius Inhibition Taping in Patients With Mechanical Neck PainDr. Krishna N. SharmaNo ratings yet
- Effect of Lumbar Stabilization and Dynamic LumbarDocument9 pagesEffect of Lumbar Stabilization and Dynamic LumbarwladjaNo ratings yet
- Effects of Six-Week Exercise Training Protocol On Pain Relief in Patients With Lumbar Disc HerniationDocument7 pagesEffects of Six-Week Exercise Training Protocol On Pain Relief in Patients With Lumbar Disc HerniationAlexandra NistorNo ratings yet
- HKPJ 39 025Document9 pagesHKPJ 39 025IlhamDikaNo ratings yet
- Background:: TH ST THDocument6 pagesBackground:: TH ST THRahayu WindariNo ratings yet
- 3 8 24 398Document6 pages3 8 24 398brain jackNo ratings yet
- Pi Is 000399931300453 XDocument7 pagesPi Is 000399931300453 XFarhaanKhanHaleemNo ratings yet
- Patients' Experience of Health Three Years After Structured Physiotherapy or Surgery For Lumbar Disc HerniationDocument8 pagesPatients' Experience of Health Three Years After Structured Physiotherapy or Surgery For Lumbar Disc HerniationsamNo ratings yet
- F0602044753 PDFDocument7 pagesF0602044753 PDFArif Adi FatuhrokhmanNo ratings yet
- Effect of NMES Vs Isometric Exercise in OA of Knee-With-Cover-Page-V2 Removed RemovedDocument5 pagesEffect of NMES Vs Isometric Exercise in OA of Knee-With-Cover-Page-V2 Removed RemovedZahra SativaniNo ratings yet
- A Review of Current Treatment Options For CoccygodyniaDocument8 pagesA Review of Current Treatment Options For CoccygodyniaClara ViMiNo ratings yet
- 24 - JPTS 2012 156Document4 pages24 - JPTS 2012 156Βιβιλάκη ΓεωργίαNo ratings yet
- Lumbar StabilizationDocument16 pagesLumbar StabilizationSahithya MNo ratings yet
- Comsenço e Alogoritmo Reabilitacao Ombrto Klintberg2014Document6 pagesComsenço e Alogoritmo Reabilitacao Ombrto Klintberg2014Sandro PerilloNo ratings yet
- Tens1Document8 pagesTens1marcelogascon.oNo ratings yet
- Efficacy of Retrowalking in Patients With Chronic Knee Osteoarthritis: A Single Group Experimental Pilot StudyDocument9 pagesEfficacy of Retrowalking in Patients With Chronic Knee Osteoarthritis: A Single Group Experimental Pilot StudyDr. Krishna N. SharmaNo ratings yet
- Artikel Mahasiswa AkhirDocument5 pagesArtikel Mahasiswa AkhirAfdan Tegar NugrohoNo ratings yet
- Short-And Long-Term Effects of Exercise On Neck Muscle Function in Cervical Radiculopathy: A Randomized Clinical TrialDocument9 pagesShort-And Long-Term Effects of Exercise On Neck Muscle Function in Cervical Radiculopathy: A Randomized Clinical Trialvidisanjaya21No ratings yet
- 08IJPHY696Document8 pages08IJPHY696charleskimNo ratings yet
- 8600Document8 pages8600elchinovichileno420No ratings yet
- Chronic Back PainDocument6 pagesChronic Back PaininnyNo ratings yet
- International Journal of Health Sciences and ResearchDocument8 pagesInternational Journal of Health Sciences and Researchrizk86No ratings yet
- Penatalaksanaan Fisioterapi Pada Kasus: Osteoarthritis Knee Sinistra Dengan Modalitas Infra Red (Ir) Dan Terapi LatihanDocument9 pagesPenatalaksanaan Fisioterapi Pada Kasus: Osteoarthritis Knee Sinistra Dengan Modalitas Infra Red (Ir) Dan Terapi LatihanDerti BenuNo ratings yet
- Tufekci Et Al. The Effectiveness of Manipulation in Combination With Exercise For Patients With CoccydDocument6 pagesTufekci Et Al. The Effectiveness of Manipulation in Combination With Exercise For Patients With CoccydMilton Ricardo de Medeiros FernandesNo ratings yet
- Burger Et Al 2016 Effect of Corticosteroid Injections Versus Physiotherapy On Pain Shoulder Range of Motion andDocument9 pagesBurger Et Al 2016 Effect of Corticosteroid Injections Versus Physiotherapy On Pain Shoulder Range of Motion andchandni saxenaNo ratings yet
- ptrs009 03 03 PDFDocument6 pagesptrs009 03 03 PDFGusti Ayu KrisnayantiNo ratings yet
- Effect of Lumbar Stabilization Exercise On Disc Herniation Index, Sacral Angle, and Functional Improvement in Patients With Lumbar Disc HerniationDocument5 pagesEffect of Lumbar Stabilization Exercise On Disc Herniation Index, Sacral Angle, and Functional Improvement in Patients With Lumbar Disc HerniationMuhammad Ridha Al JinaniNo ratings yet
- Penatalaksanaan Fisioterapi Pada KondisiDocument8 pagesPenatalaksanaan Fisioterapi Pada KondisiMuhamad BenyaminNo ratings yet
- 2017 PNF and Manual Therapy Treatment Results of Cervical OADocument7 pages2017 PNF and Manual Therapy Treatment Results of Cervical OApainfree888100% (1)
- Article 9Document8 pagesArticle 9umair muqriNo ratings yet
- Riginal Research: LucasDocument11 pagesRiginal Research: Lucas'fanny Quenhita'No ratings yet
- 8Document1 page8Daniel GuevaraNo ratings yet
- 10 1016@j Physio 2019 11 002Document27 pages10 1016@j Physio 2019 11 002Milton Ricardo de Medeiros FernandesNo ratings yet
- Effect of Positional Release Technique in Subjects With Subacute TrapezitisDocument9 pagesEffect of Positional Release Technique in Subjects With Subacute TrapezitisijphyNo ratings yet
- Effectiveness of Intradialytic Stretching Exercise On Pain Due To Muscle Cramps Among Patients Undergoing HaemodialysisDocument7 pagesEffectiveness of Intradialytic Stretching Exercise On Pain Due To Muscle Cramps Among Patients Undergoing HaemodialysisAhmad IsmailNo ratings yet
- I C M M, M O, H P A M T P - F H P: A R C TDocument9 pagesI C M M, M O, H P A M T P - F H P: A R C TAngie D. AndradesNo ratings yet
- Sports Hernia and Athletic Pubalgia: Diagnosis and TreatmentFrom EverandSports Hernia and Athletic Pubalgia: Diagnosis and TreatmentDavid R. DiduchNo ratings yet
- Principles of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodFrom EverandPrinciples of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodShigehiko KatadaNo ratings yet
- Use of The Thera Cane: What Is A Trigger Point?Document6 pagesUse of The Thera Cane: What Is A Trigger Point?Al BnNo ratings yet
- ACCUNIQBC300 UserManual 161124 Rev1.1Document68 pagesACCUNIQBC300 UserManual 161124 Rev1.1Al BnNo ratings yet
- Theracane®: (For Deep Pressure Massage)Document16 pagesTheracane®: (For Deep Pressure Massage)Al BnNo ratings yet
- For Deep Pressure Massage: Theracane Owner'S ManualDocument15 pagesFor Deep Pressure Massage: Theracane Owner'S ManualAl BnNo ratings yet
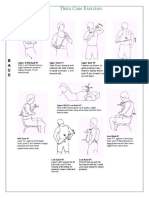
- Thera Cane Exercises - tcm75-469554Document3 pagesThera Cane Exercises - tcm75-469554Al BnNo ratings yet
- Deep Muscle Self Care GuideDocument40 pagesDeep Muscle Self Care GuideWilliam NguyenNo ratings yet
- 21Q1 1.1 Buddy Manual PreviewDocument12 pages21Q1 1.1 Buddy Manual PreviewAl BnNo ratings yet
- Exercises Print PDFDocument3 pagesExercises Print PDFZayZay317No ratings yet
- BMW Rescue Manual ENG Up by Dunaj2Document36 pagesBMW Rescue Manual ENG Up by Dunaj2Al BnNo ratings yet
- Thera Cane Exercises - tcm75-469554Document3 pagesThera Cane Exercises - tcm75-469554Al BnNo ratings yet
- Palmassager Handheld Massager Catalog RedactedDocument1 pagePalmassager Handheld Massager Catalog RedactedAl BnNo ratings yet
- Exercises Print PDFDocument3 pagesExercises Print PDFZayZay317No ratings yet
- Electrical System OverviewDocument275 pagesElectrical System OverviewAl BnNo ratings yet
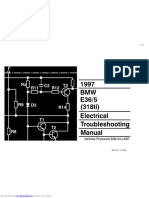
- 1998 BMW E36 318is/c, 323i/c, 328i/c, M3/c Electrical Troubleshooting ManualDocument386 pages1998 BMW E36 318is/c, 323i/c, 328i/c, M3/c Electrical Troubleshooting ManualAl BnNo ratings yet
- BMW Rescue Manual ENG Up by Dunaj2Document36 pagesBMW Rescue Manual ENG Up by Dunaj2Al BnNo ratings yet
- Best Drum Practice Pad Warmup Spacing PDFDocument3 pagesBest Drum Practice Pad Warmup Spacing PDFLuz Dary BotelloNo ratings yet
- Final MHA Thesis, Getachew L.Document62 pagesFinal MHA Thesis, Getachew L.Ochom Yar RiamNo ratings yet
- Wrist Stretching and Posture Guide: @kastor - UyDocument14 pagesWrist Stretching and Posture Guide: @kastor - UyIzzaldinNo ratings yet
- Internship Report of Global Insurance Ltd. by M A Muhaimin Alveen Batch-XIIDocument16 pagesInternship Report of Global Insurance Ltd. by M A Muhaimin Alveen Batch-XIIKIRAN BHATTARAINo ratings yet
- Sja Self-Learning Kit No.4: Fourth Quarter Title of The ModuleDocument15 pagesSja Self-Learning Kit No.4: Fourth Quarter Title of The ModuleMariel Gregore100% (1)
- Sss Gsis LawDocument57 pagesSss Gsis LawBroy D Brium100% (1)
- Drug Therapy of MalariaDocument41 pagesDrug Therapy of MalariaAbby LiewNo ratings yet
- Frenillo LingualDocument9 pagesFrenillo LingualJosé DavidNo ratings yet
- IISC UG Info Handbook FinalDocument36 pagesIISC UG Info Handbook FinalvijaynaikNo ratings yet
- The Effects of Online Learning On Students' Eyes Health: A Case in West JavaDocument40 pagesThe Effects of Online Learning On Students' Eyes Health: A Case in West JavaRagilby IzzaNo ratings yet
- Ethanol 99-7-100 (Absolute) AnalaRDocument4 pagesEthanol 99-7-100 (Absolute) AnalaRPrabath MadusankaNo ratings yet
- COVID-19 Vaccination Hesitancy, Misinformation and Conspiracy Theories On Social Media: A Content Analysis of Twitter DataDocument30 pagesCOVID-19 Vaccination Hesitancy, Misinformation and Conspiracy Theories On Social Media: A Content Analysis of Twitter DataPutri Raudatul JannahNo ratings yet
- Brittle Bone Disease Causes Fragile BonesDocument30 pagesBrittle Bone Disease Causes Fragile BonesKhim GoyenaNo ratings yet
- Artikel Kebakaran Hutan Dan Lahan - 3344Document21 pagesArtikel Kebakaran Hutan Dan Lahan - 3344Ega Ista NengrumNo ratings yet
- NUTR 150 Case Study on Zane's Nutrition and Risk FactorsDocument4 pagesNUTR 150 Case Study on Zane's Nutrition and Risk FactorsAndrea CusumanoNo ratings yet
- VRBDADocument2 pagesVRBDAEga DeviNo ratings yet
- Акушерство Фукс англ 2019Document875 pagesАкушерство Фукс англ 2019ȜLaa AsHrafNo ratings yet
- Sterilization Consent Form: LDSS-3134Document1 pageSterilization Consent Form: LDSS-3134Jack TedescoNo ratings yet
- Rheumatic Heart DiseaseDocument3 pagesRheumatic Heart DiseasearyshamyleeNo ratings yet
- Project ManagementDocument54 pagesProject ManagementJustin PauNo ratings yet
- Total Quality Management Plays Important Role in The Production ProcessDocument61 pagesTotal Quality Management Plays Important Role in The Production ProcessAmrita Bhat100% (1)
- Economics ProjectDocument21 pagesEconomics ProjectANSHIKA CHAUHANNo ratings yet
- Customs and Taboos of Bidayuh CommunityDocument16 pagesCustoms and Taboos of Bidayuh Communitykhairul ikhwanNo ratings yet
- 2020 Dental-CertificateDocument2 pages2020 Dental-CertificateReygine RamosNo ratings yet
- Medical Terminology: Thе Best Illustrated Guide for Health Care Students and Professionals to Learn and Improve Medical SkillsDocument200 pagesMedical Terminology: Thе Best Illustrated Guide for Health Care Students and Professionals to Learn and Improve Medical SkillsChristieBrownNo ratings yet
- Group 5 Leadership and TeamworkDocument4 pagesGroup 5 Leadership and TeamworkRanets MamondoleNo ratings yet
- Mem671 Case Study March 2023Document11 pagesMem671 Case Study March 2023AIMAN ASYRAAF BIN ROSLANNo ratings yet