You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A Midnight Clear EditDocument8 pagesA Midnight Clear EditMichael0213No ratings yet
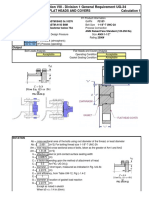
- ASME BPVC 2008a Section VIII - Division 1 General Requirement UG-34Document12 pagesASME BPVC 2008a Section VIII - Division 1 General Requirement UG-34akarczNo ratings yet
- Jadwal Jaga RS HAM Agustus 2023Document1 pageJadwal Jaga RS HAM Agustus 2023Ilham KurniawanNo ratings yet
- 3 Inflammation and OsteoporosisDocument28 pages3 Inflammation and OsteoporosisIlham KurniawanNo ratings yet
- Physiology of SkinDocument29 pagesPhysiology of SkinIlham KurniawanNo ratings yet
- Physiology of Respiratory System: Gusbakti Prof .DR Physiology University MUHAMMADYAH North SumatraDocument134 pagesPhysiology of Respiratory System: Gusbakti Prof .DR Physiology University MUHAMMADYAH North SumatraIlham KurniawanNo ratings yet
- Tuberkulosis Anak: Dr. Dewi Angreany M.Ked (Ped), Sp.ADocument52 pagesTuberkulosis Anak: Dr. Dewi Angreany M.Ked (Ped), Sp.AIlham KurniawanNo ratings yet
- MPRXCX Flexiship 6 - 10kv EngDocument3 pagesMPRXCX Flexiship 6 - 10kv EngFaziNo ratings yet
- EIM Exploratory Course: Quarter 1 - Module 5: Check Condition of Tools and EquipmentDocument17 pagesEIM Exploratory Course: Quarter 1 - Module 5: Check Condition of Tools and EquipmentIng Yng CoNo ratings yet
- Hlep / Vsax: High Performance Cryogenic Reciprocating PumpsDocument4 pagesHlep / Vsax: High Performance Cryogenic Reciprocating Pumpsbarun1977No ratings yet
- Bridging Ageing and Disability - An IntroductionDocument8 pagesBridging Ageing and Disability - An IntroductionGerald NwekeNo ratings yet
- Chemistry Project ReportDocument14 pagesChemistry Project ReportSonam Aggarwal54% (13)
- Standard Front Office Billing InstructionsDocument2 pagesStandard Front Office Billing InstructionsJan Hidalgo LaroyaNo ratings yet
- P S L A R: Canadian Environmental Protection Act, 1999Document68 pagesP S L A R: Canadian Environmental Protection Act, 1999Naeem MajeedNo ratings yet
- Peer TutoringDocument9 pagesPeer Tutoringapi-254418686No ratings yet
- EPLC Stage Gate Reviews Practices GuideDocument5 pagesEPLC Stage Gate Reviews Practices GuideAnonymous XgX8kTNo ratings yet
- Agra Report Final TermDocument87 pagesAgra Report Final TermRafael AdanNo ratings yet
- Top M3 Adler Individual PsychologyDocument6 pagesTop M3 Adler Individual Psychologyteam SAMNo ratings yet
- DS - W73550 - BEAMMASTER 5 IR Smoke and Heat Detector TX RXDocument2 pagesDS - W73550 - BEAMMASTER 5 IR Smoke and Heat Detector TX RXEmir PanjetaNo ratings yet
- Passenger & Freight Elevator Pre-Inspection Checklist 2014 - FinalDocument3 pagesPassenger & Freight Elevator Pre-Inspection Checklist 2014 - FinalMostafa MohmmedNo ratings yet
- Aliofkhazraei M. (Ed.) - Electroplating of NanostructuresDocument287 pagesAliofkhazraei M. (Ed.) - Electroplating of NanostructuresSIMETNo ratings yet
- IGS Technical ProgramDocument15 pagesIGS Technical ProgramSalma AzizahNo ratings yet
- Eee150 Chapter 3 (Electrical Safety) PDFDocument52 pagesEee150 Chapter 3 (Electrical Safety) PDFMUHAMMAD LUKMAN ARSHADNo ratings yet
- Driving Related Stress and Coping Strategies Among Car Drivers and Riders of KarachiDocument19 pagesDriving Related Stress and Coping Strategies Among Car Drivers and Riders of KarachiUzair RiazNo ratings yet
- Operating Procedure Manual: Day-Ahead Market DeskDocument44 pagesOperating Procedure Manual: Day-Ahead Market DeskHadi AntouryNo ratings yet
- Recycled Chopping BoardDocument13 pagesRecycled Chopping BoardDejan RancicNo ratings yet
- 39-Article Text-131-1-10-20191111Document9 pages39-Article Text-131-1-10-20191111berlian gurningNo ratings yet
- Chapter 37Document112 pagesChapter 37Arcanos2312No ratings yet
- LAS Q1 ModalsDocument11 pagesLAS Q1 ModalsAnnaliza Saludaga - PerezNo ratings yet
- MSE GeotextileDocument23 pagesMSE GeotextileshumwenjunNo ratings yet
- Loading Shovel & Backhoe: Australia & New Zealand SpecificationsDocument16 pagesLoading Shovel & Backhoe: Australia & New Zealand Specificationsadnan putraluhsyNo ratings yet
- Chapter 1 - Changing Nature of Human Resource ManagementDocument21 pagesChapter 1 - Changing Nature of Human Resource ManagementFatih BIYIKLINo ratings yet
- Wisnu NugrahaDocument2 pagesWisnu Nugrahanando745No ratings yet
- DIC Connector Info - JSTDocument0 pagesDIC Connector Info - JSTlamping_apNo ratings yet
- Case Study Saket Select CityDocument4 pagesCase Study Saket Select Cityहर्षद भारती रविंद् साठे.No ratings yet