You might also like
- The Ultimate Frozen Shoulder Therapy Guide, 2005Document49 pagesThe Ultimate Frozen Shoulder Therapy Guide, 2005Phany Ezail Ududec100% (5)
- Pulmo Management Week 1Document160 pagesPulmo Management Week 1Dharlyn MungcalNo ratings yet
- Shoulder Movement Analysis: The Overhand Volleyball ServeDocument14 pagesShoulder Movement Analysis: The Overhand Volleyball Serveapi-340991045No ratings yet
- Dave Tate's Free Squat ManualDocument38 pagesDave Tate's Free Squat ManualZack Farsheed DavoodiNo ratings yet
- Anatomy of Respiratory SystemDocument75 pagesAnatomy of Respiratory SystemAnonymous aqeaNUn80% (5)
- Upper Respiratory Tract AnatomyDocument61 pagesUpper Respiratory Tract Anatomyيحيى اسماعيل الجميليNo ratings yet
- Orthopedics Clinical Rotation Notes 2013 (Modified) PDFDocument109 pagesOrthopedics Clinical Rotation Notes 2013 (Modified) PDFSheema Sh100% (1)
- Anatomy of Respiratory SystemDocument57 pagesAnatomy of Respiratory SystemRyan Larsen100% (1)
- Skeletal SystemDocument125 pagesSkeletal SystemJem Pantig100% (4)
- Anatomy of Respiratory System: Dr. Dwi Rita Anggraini, MkesDocument64 pagesAnatomy of Respiratory System: Dr. Dwi Rita Anggraini, MkesFira TasyaNo ratings yet
- Histology of The Respiratory SystemDocument62 pagesHistology of The Respiratory Systemmichelle100% (1)
- Respiratory SystemDocument6 pagesRespiratory SystemQK CLARONo ratings yet
- Anatomy and Physiology of Female Reproductive SystemDocument12 pagesAnatomy and Physiology of Female Reproductive SystemSyed Isamil100% (1)
- Respiratory System: Anatomy & PhysiologyDocument111 pagesRespiratory System: Anatomy & PhysiologyJape GarridoNo ratings yet
- Phase 1 Exercise ProgramDocument2 pagesPhase 1 Exercise Programkatysmith1687No ratings yet
- ENT - An Introduction and Practical Guide, Second Edition-CRC Press (2017)Document176 pagesENT - An Introduction and Practical Guide, Second Edition-CRC Press (2017)Marton B.No ratings yet
- Physiology of SkinDocument29 pagesPhysiology of SkinIlham KurniawanNo ratings yet
- Respiratory SystemDocument12 pagesRespiratory SystemTricia CabiliNo ratings yet
- Pre-Finals Topic 1 AnaphyDocument5 pagesPre-Finals Topic 1 AnaphyGlenice Joy SenocNo ratings yet
- Respiratory SystemDocument77 pagesRespiratory SystemYour Materials100% (1)
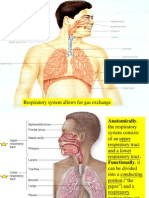
- Respiratory System Allows For Gas ExchangeDocument327 pagesRespiratory System Allows For Gas ExchangeMichael Lester100% (1)
- The Human Respiratory SystemDocument15 pagesThe Human Respiratory SystemNandita Halder100% (1)
- Respiratory System Anatomy, Assessment & Diagnostic TestsDocument24 pagesRespiratory System Anatomy, Assessment & Diagnostic TestsPrince Rener Velasco PeraNo ratings yet
- Dysphagia After Total LaryngectomyDocument6 pagesDysphagia After Total LaryngectomyEduardo Lima de Melo Jr.No ratings yet
- RESPIRATORY SYSTEM AnjuDocument38 pagesRESPIRATORY SYSTEM Anjuanju rachel jose100% (1)
- Respiratory System ReviewerDocument7 pagesRespiratory System ReviewerVictoria Ellex TiomicoNo ratings yet
- 1.anatomy of Respiratory SystemDocument73 pages1.anatomy of Respiratory Systemokoti.omutanyi22No ratings yet
- Anatomy of Respiratory SystemDocument9 pagesAnatomy of Respiratory SystemLatifah Husna Zulkafli100% (1)
- The Respiratory System: Raymund Christopher R. Dela Peña, RN, RM, MAN Clinical Faculty UNP-College of NursingDocument95 pagesThe Respiratory System: Raymund Christopher R. Dela Peña, RN, RM, MAN Clinical Faculty UNP-College of NursingrnrmmanphdNo ratings yet
- Anatomi Sistem ParuDocument64 pagesAnatomi Sistem ParuMochammad Fariz AmsalNo ratings yet
- Anaphy ReviewerDocument10 pagesAnaphy ReviewerTsukishima RinNo ratings yet
- Respiratory SystemDocument82 pagesRespiratory Systemsubhojitnayek100% (2)
- Anatomy of AirwayDocument50 pagesAnatomy of AirwayHari Om ChaurasiyaNo ratings yet
- A &P Overview Respiratory SystemDocument16 pagesA &P Overview Respiratory SystemOpeyemi OmolabakeNo ratings yet
- Respiratory SystemDocument27 pagesRespiratory Systemyoga karsendaNo ratings yet
- Respiratory SystemDocument4 pagesRespiratory SystemAlloiza CaguiclaNo ratings yet
- The Respiratory SystemDocument6 pagesThe Respiratory SystemIftikharNo ratings yet
- Respiratory System: Instructor: Mizpah A. Bañes, RN, ManDocument117 pagesRespiratory System: Instructor: Mizpah A. Bañes, RN, ManNorma TacabaNo ratings yet
- Respiratory System-2cgf2Document42 pagesRespiratory System-2cgf2Nzenwa Jedidiah KimizuNo ratings yet
- Anatomy and PhysiologyDocument7 pagesAnatomy and PhysiologyKelly Camero ÜNo ratings yet
- Anatomi Sistem PernapasanDocument64 pagesAnatomi Sistem PernapasanLili ManaoNo ratings yet
- Anatomy of The Respiratory SystemDocument8 pagesAnatomy of The Respiratory Systemsuharti2365No ratings yet
- The Respiratory Syste M: DR Arif Chowdhury Opu, MbbsDocument21 pagesThe Respiratory Syste M: DR Arif Chowdhury Opu, MbbsMuntasirNo ratings yet
- Humb1000 Compendium NotesDocument9 pagesHumb1000 Compendium NotesZeba ZiaNo ratings yet
- Respiratory SystemDocument55 pagesRespiratory SystemSitotaye DinkuNo ratings yet
- Respiratory SystemDocument5 pagesRespiratory SystemJay QuilnetNo ratings yet
- Respiratory System AnatomyDocument49 pagesRespiratory System AnatomyHiraya WNo ratings yet
- The Respiratory System: Anatomy, Biomedic 1Document39 pagesThe Respiratory System: Anatomy, Biomedic 1Grace Febryanti TodingNo ratings yet
- Respiratory System-1Document33 pagesRespiratory System-1Sadiq khanNo ratings yet
- Respiration System PP TDocument57 pagesRespiration System PP Troyanirudh99No ratings yet
- Therespiratorysystem 130524022043 Phpapp01 TestDocument21 pagesTherespiratorysystem 130524022043 Phpapp01 TestMergel GeconcilloNo ratings yet
- Respiratory System PDFDocument16 pagesRespiratory System PDFMary Ann SacramentoNo ratings yet
- Respiratory SystemDocument5 pagesRespiratory SystemPreeti ChouhanNo ratings yet
- Respiratory SystemDocument54 pagesRespiratory SystemEndin Nokik StujannaNo ratings yet
- Human Respiratory System - Britannica Online EncyclopediaDocument31 pagesHuman Respiratory System - Britannica Online EncyclopediaAlina AluculeseiNo ratings yet
- Respiratory SystemDocument61 pagesRespiratory SystemDenise Nicole PinedaNo ratings yet
- Respiratory SystemDocument27 pagesRespiratory SystemKatherineMysterieuxNo ratings yet
- Respiratory System: Joanna Cabuhay 293 Calingacion ST - Poblacion SibulanDocument6 pagesRespiratory System: Joanna Cabuhay 293 Calingacion ST - Poblacion SibulanJoanna :DNo ratings yet
- 01 Respiratory SystemDocument43 pages01 Respiratory Systemhafaisolo37No ratings yet
- The Respiratory SystemDocument28 pagesThe Respiratory SystemJuma SammyNo ratings yet
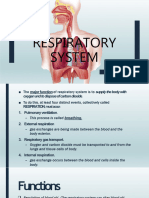
- Functions of The Respiratory System: BloodDocument12 pagesFunctions of The Respiratory System: BloodSesrine BuendiaNo ratings yet
- Anatomy and Physiology of The Respiratory SystemDocument9 pagesAnatomy and Physiology of The Respiratory SystemMitchy SunNo ratings yet
- San Beda Respiratory System 9-15Document68 pagesSan Beda Respiratory System 9-15conyxzNo ratings yet
- The Respirator Y System: Mungcal, Dharlynette RTRPDocument158 pagesThe Respirator Y System: Mungcal, Dharlynette RTRPDharlyn MungcalNo ratings yet
- The Respiratory SystemDocument28 pagesThe Respiratory SystemJuma SammyNo ratings yet
- Functions of The Respiratory SystemDocument10 pagesFunctions of The Respiratory SystemKrisha AvorqueNo ratings yet
- Week 3 Respiratory SystemDocument10 pagesWeek 3 Respiratory SystemangeliaNo ratings yet
- Anatomy 2nd-U-3 Respiratory SystemDocument113 pagesAnatomy 2nd-U-3 Respiratory Systemsinte beyuNo ratings yet
- LEC - Week 9 (Respiratory)Document42 pagesLEC - Week 9 (Respiratory)Al SerenosoNo ratings yet
- Breathe In, Breathe Out: Learning About Your LungsFrom EverandBreathe In, Breathe Out: Learning About Your LungsRating: 3.5 out of 5 stars3.5/5 (3)
- 3 Inflammation and OsteoporosisDocument28 pages3 Inflammation and OsteoporosisIlham KurniawanNo ratings yet
- HipertiroidDocument48 pagesHipertiroidIlham KurniawanNo ratings yet
- Tuberkulosis Anak: Dr. Dewi Angreany M.Ked (Ped), Sp.ADocument52 pagesTuberkulosis Anak: Dr. Dewi Angreany M.Ked (Ped), Sp.AIlham KurniawanNo ratings yet
- Iii Year Mbbs Question Bank Ophthalmology & Ent (Short Answers)Document54 pagesIii Year Mbbs Question Bank Ophthalmology & Ent (Short Answers)051 DhinakarNo ratings yet
- ACB Dan FIBCDocument21 pagesACB Dan FIBCharjunaNo ratings yet
- Element Element ElementDocument34 pagesElement Element ElementenmassNo ratings yet
- Cavernous Sinus ThrombosisDocument6 pagesCavernous Sinus ThrombosismcwnotesNo ratings yet
- How To Work Wonders With A Piece of Wood: The Elitefts Definitive Guide To Board PressingDocument12 pagesHow To Work Wonders With A Piece of Wood: The Elitefts Definitive Guide To Board PressingDaniel RasiaNo ratings yet
- 3.LUNGS Medo NotesDocument17 pages3.LUNGS Medo NotesChandrababu ANo ratings yet
- Beauty Center: Jl. Rungkut Asri Timur 18 No.22 (RUKO), Open Every Day 9am - 7PmDocument8 pagesBeauty Center: Jl. Rungkut Asri Timur 18 No.22 (RUKO), Open Every Day 9am - 7Pmnurainy triasNo ratings yet
- Maxillarysinus 170705134531 PDFDocument93 pagesMaxillarysinus 170705134531 PDFmelaniaNo ratings yet
- PA (Revised)Document16 pagesPA (Revised)Daryl Jake FornollesNo ratings yet
- Head Neck and Regional LymphaticsDocument34 pagesHead Neck and Regional LymphaticsDr Husam AlzghoulNo ratings yet
- Mrs Potato Head 25780Document2 pagesMrs Potato Head 25780Ligia DragomirNo ratings yet
- Dev of Hard & Soft PalateDocument94 pagesDev of Hard & Soft PalatepriyaNo ratings yet
- MED 1101 - Descriptive Anatomy I - 2015Document8 pagesMED 1101 - Descriptive Anatomy I - 2015Sanjay VeerasammyNo ratings yet
- Urinary System-Anatomy and PhysiologyDocument20 pagesUrinary System-Anatomy and PhysiologyFlo Neri BerondoNo ratings yet
- Special Senses: Physiology / 2009-10 Dr. Ahmad .S. AlarabiDocument29 pagesSpecial Senses: Physiology / 2009-10 Dr. Ahmad .S. AlarabiJerome EkohNo ratings yet
- The Heart of The ProblemDocument6 pagesThe Heart of The ProblemKeaton0% (1)
- Anatomy of Orofacial Structures 7th Edition Brand Test BankDocument10 pagesAnatomy of Orofacial Structures 7th Edition Brand Test Bankalmaydyd100% (41)
- The Endocrine System Work SheetDocument3 pagesThe Endocrine System Work SheetLucia SpaninksNo ratings yet
- Physical Assessment of The IntegumentDocument75 pagesPhysical Assessment of The IntegumentDiane BaunsitNo ratings yet
- Utility of Neurodiagnostic Studies in The Diagnosis of Autoimmune Encephalitis in PDFDocument26 pagesUtility of Neurodiagnostic Studies in The Diagnosis of Autoimmune Encephalitis in PDFMaverick 18No ratings yet
- Isolated Medial Collateral Ligament Injuries in The KneeDocument6 pagesIsolated Medial Collateral Ligament Injuries in The KneekenthepaNo ratings yet