You might also like
- Quiz 11 Unit .3 Patricia E. Benner Introduction of Nursing Theory & ModelDocument3 pagesQuiz 11 Unit .3 Patricia E. Benner Introduction of Nursing Theory & ModelZhedriex EspirituNo ratings yet
- Chapter 53 - Assessment and Management of Patients With Allergic DisordersDocument16 pagesChapter 53 - Assessment and Management of Patients With Allergic DisordersTeemara KingNo ratings yet
- Introduction To NutritionDocument37 pagesIntroduction To NutritionburningutotNo ratings yet
- Building Primitive Traps & SnaresDocument101 pagesBuilding Primitive Traps & SnaresJoseph Madr90% (10)
- Laryngitis Nhs ChoicesDocument8 pagesLaryngitis Nhs ChoicesAndrew TandohNo ratings yet
- 3 Frequencydistributionsandgraphs 120820000310 Phpapp02Document32 pages3 Frequencydistributionsandgraphs 120820000310 Phpapp02Javed IqbalNo ratings yet
- Science Grade 9 Learners MaterialDocument27 pagesScience Grade 9 Learners MaterialDeborah OmilesNo ratings yet
- Lesson 04-The DerivativeDocument14 pagesLesson 04-The DerivativeAXELLE NICOLE GOMEZNo ratings yet
- Assessment in Learning 2 Module RIVERADocument159 pagesAssessment in Learning 2 Module RIVERACalamares YtpremsNo ratings yet
- Exam CirculatoryDocument1 pageExam CirculatoryLuisa RamosNo ratings yet
- MR and MS Intrams 2017Document4 pagesMR and MS Intrams 2017Nikko VillanuevaNo ratings yet
- Metabolism: Marcus Cueno, RNDocument15 pagesMetabolism: Marcus Cueno, RNMarcus, RN100% (2)
- Healthcare Ethics - LP 1Document35 pagesHealthcare Ethics - LP 1Daisy RoseteNo ratings yet
- Affordable O2 XDA Zinc phone for saleDocument6 pagesAffordable O2 XDA Zinc phone for saleRanz GarciaNo ratings yet
- Math9 Q2 Mod5Document16 pagesMath9 Q2 Mod5Shawee Gucor Saquilabon100% (1)
- Average and Instantaneous AccelerationDocument35 pagesAverage and Instantaneous AccelerationaraneyaNo ratings yet
- 11.1 Multiple Choice Part I Questions: Chapter 11 The Cardiovascular SystemDocument33 pages11.1 Multiple Choice Part I Questions: Chapter 11 The Cardiovascular SystemmuryumNo ratings yet
- 3rd (X) Lecture (NCM106 ABC IV) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingDocument17 pages3rd (X) Lecture (NCM106 ABC IV) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingKamx Mohammed100% (1)
- 7 - Regulation and Functions of The Thyroid HormonesDocument31 pages7 - Regulation and Functions of The Thyroid HormonesVigneshwaran RavishankarNo ratings yet
- Activity 2B Integumentary System LOPEZ 1.0Document3 pagesActivity 2B Integumentary System LOPEZ 1.0Ma. Joanna Catherine LopezNo ratings yet
- Chem 1ST SemDocument98 pagesChem 1ST SemAubrey Rosales100% (1)
- Chapter 3 - Genetics (Fundamentals of Anatomy and Physiology For Nursing and Healthcare Students)Document87 pagesChapter 3 - Genetics (Fundamentals of Anatomy and Physiology For Nursing and Healthcare Students)Mary Grace MartinNo ratings yet
- Biostatistics, Exam - Nursing, July, 2005Document6 pagesBiostatistics, Exam - Nursing, July, 2005tesfaye gelanNo ratings yet
- Respiratory System QuizDocument7 pagesRespiratory System QuizPhilip YansonNo ratings yet
- Guitar Lessons-April 30,2018Document14 pagesGuitar Lessons-April 30,2018Lednelg YosoresNo ratings yet
- Test Taking Strategies2018Document11 pagesTest Taking Strategies2018Soleil MaxwellNo ratings yet
- AnaphyDocument31 pagesAnaphyBiano, Fortune JayneNo ratings yet
- Foundation of Midwifery Practice (M 100) : Marie Belen C. Tamayor, RN, Man ©Document66 pagesFoundation of Midwifery Practice (M 100) : Marie Belen C. Tamayor, RN, Man ©Mariebelen TamayorNo ratings yet
- Intro To Psychology (Mid Exam)Document2 pagesIntro To Psychology (Mid Exam)Mishal FatimaNo ratings yet
- LET Reviewer Biology Part 1Document4 pagesLET Reviewer Biology Part 1Gemma HernandezNo ratings yet
- MULTIPLE CHOICE. Choose The One Alternative That Best Completes The Statement or Answers The QuestionDocument20 pagesMULTIPLE CHOICE. Choose The One Alternative That Best Completes The Statement or Answers The Questionmiamikiko100% (4)
- Fundamentals of NursingDocument12 pagesFundamentals of NursingTine SabaulanNo ratings yet
- QuartilesDocument8 pagesQuartilessushiljp1984No ratings yet
- LS 2 - Human Respiratory SystemDocument5 pagesLS 2 - Human Respiratory SystemAisha KassandraNo ratings yet
- Grade 9 Science Competencies and LessonsDocument3 pagesGrade 9 Science Competencies and Lessonssai roqueNo ratings yet
- Sustainable Development Lesson 1-FinalsDocument4 pagesSustainable Development Lesson 1-FinalsShiro MisakiNo ratings yet
- Biochemistry Quiz - Enzymes and Vitamins - Answer KeyDocument8 pagesBiochemistry Quiz - Enzymes and Vitamins - Answer KeyKennethNo ratings yet
- MarsiiDocument35 pagesMarsiiMariel Magtalas100% (1)
- I. Multiple Choice. Encircle The Letter of Best Answer. (1pt)Document6 pagesI. Multiple Choice. Encircle The Letter of Best Answer. (1pt)Dianne PeñaNo ratings yet
- The Family With A ToddlerDocument36 pagesThe Family With A ToddlerDaryl Adrian RecaidoNo ratings yet
- Quiz BeeDocument34 pagesQuiz BeeMhel DemabogteNo ratings yet
- Individual Aging Vs Population AgingDocument78 pagesIndividual Aging Vs Population AgingAnonymous iG0DCOf0% (2)
- Department of Health - Adolescent and Youth Health Program (AYHP) - 2011-10-27Document8 pagesDepartment of Health - Adolescent and Youth Health Program (AYHP) - 2011-10-27daryl ann dep-asNo ratings yet
- Law of Conservation of EnergyDocument3 pagesLaw of Conservation of EnergyIrwin Ariel D. MielNo ratings yet
- Traditional and Alternative Medicine Act (TAMA)Document10 pagesTraditional and Alternative Medicine Act (TAMA)Micha AndreaNo ratings yet
- ETHICSDocument4 pagesETHICSJeth Vigilla NangcaNo ratings yet
- Exam 1 Multiple Choice Questions on Wellness and FitnessDocument13 pagesExam 1 Multiple Choice Questions on Wellness and FitnessJeselie PabilaNo ratings yet
- TFN-MIDTERMS-AND-SEMIS Bat Exam ReviewerDocument59 pagesTFN-MIDTERMS-AND-SEMIS Bat Exam ReviewerPrince D. JacobNo ratings yet
- EE40 Basic Electrical Engineering (DC Series-Parralel Circuit)Document45 pagesEE40 Basic Electrical Engineering (DC Series-Parralel Circuit)jason sutanaNo ratings yet
- Grade 9 Learner's Module v1.0Document394 pagesGrade 9 Learner's Module v1.0Pattey Manlapaz100% (2)
- Adult Module 3 - Increasing Fruit and Vegetable Intake Handout (English) PDFDocument4 pagesAdult Module 3 - Increasing Fruit and Vegetable Intake Handout (English) PDFKennedy Fadriquelan0% (1)
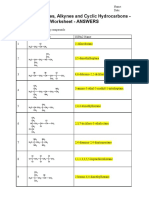
- OC02 - Alkenes, Alkynes and Cyclic Hydrocarbons - WorksheetDocument5 pagesOC02 - Alkenes, Alkynes and Cyclic Hydrocarbons - WorksheetAaravee KNo ratings yet
- Public Health With AnswersDocument8 pagesPublic Health With AnswersJulie Hope CorveraNo ratings yet
- Anaphy-Chapter 1-7 Reviewer (Seeley's 12th Edition)Document15 pagesAnaphy-Chapter 1-7 Reviewer (Seeley's 12th Edition)Bullosos, Siera Jade Anne R.No ratings yet
- Math10 LAS Set 1 Week 1 4Document39 pagesMath10 LAS Set 1 Week 1 4Burner StuffNo ratings yet
- 1 MODULE CHAPTER 12 AnaPhy 2020 2021 PDFDocument27 pages1 MODULE CHAPTER 12 AnaPhy 2020 2021 PDFJosh MagatNo ratings yet
- Fundamental Principle of CountingDocument16 pagesFundamental Principle of CountingEcho AlbertoNo ratings yet
- GametogenesisDocument14 pagesGametogenesisGreenphoenixNo ratings yet
- Lesson 13 - Diabetes, Cancer and Heart DiseaseDocument28 pagesLesson 13 - Diabetes, Cancer and Heart DiseaseAlejandro GuerreroNo ratings yet
- DLP g10 Math 2nd QTR Week 4 FinalDocument10 pagesDLP g10 Math 2nd QTR Week 4 FinalCei-CeiNo ratings yet
- Respiratory System Chapter SummaryDocument7 pagesRespiratory System Chapter Summaryqueen nurseNo ratings yet
- Respiratory System Anatomy & PhysiologyDocument12 pagesRespiratory System Anatomy & PhysiologyDgjj CompuiterNo ratings yet
- Essential Factors for Planning Dental BridgesDocument8 pagesEssential Factors for Planning Dental BridgesShazrin AhmadNo ratings yet
- Biology Paper 1, 2, 3 Trial SPM 2011 MRSMDocument86 pagesBiology Paper 1, 2, 3 Trial SPM 2011 MRSMSashaSparksNo ratings yet
- FIFe EMS System User GuidelinesDocument3 pagesFIFe EMS System User GuidelinesAlexanderSmithNo ratings yet
- Presentation About CellsDocument39 pagesPresentation About Cellsharfiyanto100% (2)
- Phylum Annelida 3Document43 pagesPhylum Annelida 3irsyad100% (1)
- BestialityDocument3 pagesBestialityJustine May S. ColicoNo ratings yet
- Sindrome de DownDocument27 pagesSindrome de DownKhissi BArzaNo ratings yet
- The Pathway To HealthDocument81 pagesThe Pathway To HealthKit Cain100% (2)
- Flashcard Español Ingles 1001 DefinicionesDocument100 pagesFlashcard Español Ingles 1001 DefinicionesRubenMorenoGutierrezNo ratings yet
- Chicken Leg DissectionDocument1 pageChicken Leg DissectionNadrah Harith FadzilahNo ratings yet
- George Orwell - Animal Farm (Summary)Document12 pagesGeorge Orwell - Animal Farm (Summary)nahidkabir2009No ratings yet
- MC AGR-Q4101 Dairy-Farmer-Entrepreneur 1Document24 pagesMC AGR-Q4101 Dairy-Farmer-Entrepreneur 1Kaushik AgrawalNo ratings yet
- ANP1105 Final Exam Review - Respiratory, Lymphatic SystemsDocument4 pagesANP1105 Final Exam Review - Respiratory, Lymphatic SystemsVienna GilmoreNo ratings yet
- Osmoregulation in Earthworms ExplainedDocument28 pagesOsmoregulation in Earthworms ExplainedMa-anJaneDiamosNo ratings yet
- RNTCP - Wikipedia, The Free EncyclopediaDocument5 pagesRNTCP - Wikipedia, The Free EncyclopediaakurilNo ratings yet
- Biophysical Profile (BPP): A 30-Minute Fetal Well-Being TestDocument6 pagesBiophysical Profile (BPP): A 30-Minute Fetal Well-Being TestKikiNo ratings yet
- Modul Pembilna TPA Saintek Kelas XIIDocument103 pagesModul Pembilna TPA Saintek Kelas XIIRisma Damayanti100% (1)
- Titan XC Parent HandbookDocument28 pagesTitan XC Parent HandbookTitanXCNo ratings yet
- Pleura and Pleural Cavities AnatomyDocument105 pagesPleura and Pleural Cavities AnatomyueumanaNo ratings yet
- Allergic RhinitisDocument19 pagesAllergic RhinitisNicole Villaflor FabicoNo ratings yet
- Identifying Labelling and Marketing Advantages of Nutrients in Minced BeefDocument16 pagesIdentifying Labelling and Marketing Advantages of Nutrients in Minced BeefMelisa CalderónNo ratings yet
- Antibiotic treatment guidelines for common infectionsDocument21 pagesAntibiotic treatment guidelines for common infectionsnovaNo ratings yet
- The Complete Daily CowDocument313 pagesThe Complete Daily CowDAVID WYDERNo ratings yet
- (KBA BU HANUM) Senyawa Fenolik AlamDocument134 pages(KBA BU HANUM) Senyawa Fenolik AlamPoppyA.NamiraNo ratings yet
- Daun Gatal PDFDocument7 pagesDaun Gatal PDFIswandi AzisNo ratings yet
- The Tongue: Anatomy, Taste, and Common ConditionsDocument5 pagesThe Tongue: Anatomy, Taste, and Common ConditionsMark TiongsonNo ratings yet
- HK VTC 25-11-2006 Medicinal MushroomsDocument31 pagesHK VTC 25-11-2006 Medicinal MushroomsdeepthikuppuswamyNo ratings yet
- Feline Soft Tissue and General Surgery (VetBooks - Ir)Document721 pagesFeline Soft Tissue and General Surgery (VetBooks - Ir)cosminaNo ratings yet