You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Memonic Exam 2Document18 pagesMemonic Exam 2Justine Grace TolentinoNo ratings yet
- Fluid Electrolyte WorksheetDocument8 pagesFluid Electrolyte WorksheetJonna EstabilloNo ratings yet
- IV Compatibility ChartDocument6 pagesIV Compatibility ChartMae Quenie Abadingo Tiro75% (4)
- FurosemideDocument4 pagesFurosemideapi-3797941100% (1)
- An Assignment On Routinely Use Drugs in Our Clinic: Submitted To: Submitted byDocument48 pagesAn Assignment On Routinely Use Drugs in Our Clinic: Submitted To: Submitted byIbad Ur Rahman100% (1)
- Drug Study - FurosemideDocument3 pagesDrug Study - FurosemideIzza DeloriaNo ratings yet
- Notes Assessing The Male Genitalia and RectumDocument11 pagesNotes Assessing The Male Genitalia and RectumElvira GumiNo ratings yet
- Drug Study Delivery RoomDocument7 pagesDrug Study Delivery RoomkhleeoNo ratings yet
- Drug Study - FurosemideDocument2 pagesDrug Study - FurosemideKian HerreraNo ratings yet
- 50 Drugs: Every Emergency Physician Should KnowDocument52 pages50 Drugs: Every Emergency Physician Should KnowMohamed Abu ElgheetNo ratings yet
- Pharmacology Practice Test IDocument27 pagesPharmacology Practice Test Isidharta_chatterjeeNo ratings yet
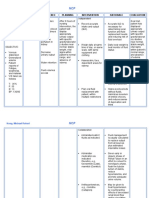
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Inference Planning Intervention Rationale EvaluationMr. whiteNo ratings yet
- Nursing Compilation of Questions June2019Document154 pagesNursing Compilation of Questions June2019Wani Zahoor0% (1)
- A World of RegionsDocument3 pagesA World of RegionsElvira GumiNo ratings yet
- MeaslesWhatYouShouldKnow ADADocument1 pageMeaslesWhatYouShouldKnow ADAElvira GumiNo ratings yet
- Nursing Cultural DiversityDocument3 pagesNursing Cultural DiversityElvira GumiNo ratings yet
- Pharmacology Modules 1 - 2Document10 pagesPharmacology Modules 1 - 2Elvira GumiNo ratings yet
- 5876 - 874429 - Theories Applied in CHNDocument6 pages5876 - 874429 - Theories Applied in CHNElvira GumiNo ratings yet
- Furosemide Lasix 20mg TabletsDocument23 pagesFurosemide Lasix 20mg TabletsMerro KellyNo ratings yet
- Drug TabulationDocument13 pagesDrug TabulationKristian Dave DivaNo ratings yet
- Pharmacology SlidesDocument114 pagesPharmacology Slidesbrandon15000100% (9)
- Drug StudyDocument9 pagesDrug Studyjanelee2824No ratings yet
- DrugsDocument17 pagesDrugsRenzkie GeronimoNo ratings yet
- Case Study 1 PediaDocument7 pagesCase Study 1 PediaXeyanNo ratings yet
- Pharma Downloads Pharma Downloads: 1-Clinodin 2-Guanbenz 3-GuanfacineDocument5 pagesPharma Downloads Pharma Downloads: 1-Clinodin 2-Guanbenz 3-GuanfacineSrihari DivyaNo ratings yet
- IV Compatibility Chart (PDF Library)Document19 pagesIV Compatibility Chart (PDF Library)Lynda PerryNo ratings yet
- Maylynn Renal Lasix MonographDocument1 pageMaylynn Renal Lasix MonographAORN2008No ratings yet
- Renal Failure PresentationDocument110 pagesRenal Failure PresentationMusa yohana100% (1)
- Januvia, Amlodipine, FurosemideDocument4 pagesJanuvia, Amlodipine, Furosemideyummy_17100% (1)
- Pharmacy News Capsule: Update On Drug AllergyDocument6 pagesPharmacy News Capsule: Update On Drug AllergyMajd ShakerNo ratings yet
- Acute Renal FailureDocument12 pagesAcute Renal FailureElsa SimangunsongNo ratings yet
- Renal Drugs - Dr. UretaDocument4 pagesRenal Drugs - Dr. UretaAlbert CorderoNo ratings yet
- Disorders of Renal Function and EdemasDocument102 pagesDisorders of Renal Function and EdemasViorelVelenciucNo ratings yet
- Case StudyDocument17 pagesCase StudyEarl Viray JulaoNo ratings yet
- Pharmacology Handout Dr. Ann SpolarichDocument16 pagesPharmacology Handout Dr. Ann SpolarichMina Lotfallah ShenoudaNo ratings yet
- Emergency Drugs Used in O.S. Common Drug Interactions in O.S. Practice Oral SurgeryDocument52 pagesEmergency Drugs Used in O.S. Common Drug Interactions in O.S. Practice Oral SurgeryFourthMolar.comNo ratings yet