You might also like
- Influenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?From EverandInfluenza vaccination: What does the scientific proof say?: Could it be more harmful than useful to vaccinate indiscriminately elderly people, pregnant women, children and health workers?No ratings yet
- Community-Acquired Pneumonia in Children: Myths and FactsDocument4 pagesCommunity-Acquired Pneumonia in Children: Myths and FactsFranciscoDelgadoNo ratings yet
- Vaccines: Making the Right Choice for Your ChildFrom EverandVaccines: Making the Right Choice for Your ChildRating: 5 out of 5 stars5/5 (2)
- 2010 Fiebre Sin FocoDocument29 pages2010 Fiebre Sin FocoHerminia CastilloNo ratings yet
- Prevention and Treatment of Seasonal Influenza: Clinical PracticeDocument7 pagesPrevention and Treatment of Seasonal Influenza: Clinical PracticeDias PradikaNo ratings yet
- Awareness On Acute Respiratory Infection Among Mothers of Children Under Five YearDocument5 pagesAwareness On Acute Respiratory Infection Among Mothers of Children Under Five YearInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Association Between Nutritional Status and Severity of Pneumonia Among Children Under Five Years Attending Wangaya District HospitalDocument7 pagesAssociation Between Nutritional Status and Severity of Pneumonia Among Children Under Five Years Attending Wangaya District HospitalchairulNo ratings yet
- Human Vaccines & Immunotherapeutics: News: Two Studies On Optimal Timing For Measles VaccinationDocument4 pagesHuman Vaccines & Immunotherapeutics: News: Two Studies On Optimal Timing For Measles VaccinationTri RachmadijantoNo ratings yet
- Evaluation and Management of Febrile Children 2016Document7 pagesEvaluation and Management of Febrile Children 2016Luisa Frj100% (1)
- Articulo 1Document6 pagesArticulo 1Esteban Jose Hernandez ZotoNo ratings yet
- Pediatrics 2012 780 92Document15 pagesPediatrics 2012 780 92ERICKNo ratings yet
- Vaksin VarelaDocument8 pagesVaksin VarelaPutra EkaNo ratings yet
- Fever in The Pediatric Patient PDFDocument24 pagesFever in The Pediatric Patient PDFSABASA1012No ratings yet
- Feverinthepediatricpatient: Robyn Wing,, Maya R. Dor,, Patricia A. McquilkinDocument24 pagesFeverinthepediatricpatient: Robyn Wing,, Maya R. Dor,, Patricia A. McquilkinAzkiaNo ratings yet
- Management of The Febrile Young Infant: Cme R ADocument6 pagesManagement of The Febrile Young Infant: Cme R AsarabisimonaNo ratings yet
- A Comparative-Descriptive Analysis of Clinical Characteristics in 2019-Coronavirus-Infected Children and AdultsDocument28 pagesA Comparative-Descriptive Analysis of Clinical Characteristics in 2019-Coronavirus-Infected Children and AdultsPatrick NunsioNo ratings yet
- Evaluacion Niño Con FiebreDocument24 pagesEvaluacion Niño Con FiebredanielentuxtlaNo ratings yet
- Local Literature: Philippine Disease outbreaks linked to vaccine fearDocument9 pagesLocal Literature: Philippine Disease outbreaks linked to vaccine fearKarl GutierrezNo ratings yet
- Impact of Vaccination On The Epidemiology of Varicella: 1995 - 2009Document9 pagesImpact of Vaccination On The Epidemiology of Varicella: 1995 - 2009Redo Kurniawan Umg IINo ratings yet
- Feverinthepediatricpatient: Robyn Wing,, Maya R. Dor,, Patricia A. McquilkinDocument24 pagesFeverinthepediatricpatient: Robyn Wing,, Maya R. Dor,, Patricia A. McquilkinSebastian SalinasNo ratings yet
- Jurnal Seasonal Influenza Vaccination Among Older Adults in Jordan Prevalence Knowledge and AttitudesDocument6 pagesJurnal Seasonal Influenza Vaccination Among Older Adults in Jordan Prevalence Knowledge and AttitudesMusdaliva Tri Riskiani AlminNo ratings yet
- Serological Testing Prior To Dengue Vaccine AdministrationDocument8 pagesSerological Testing Prior To Dengue Vaccine AdministrationJemimah BureresNo ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptAndika ZuldiansyahNo ratings yet
- (R) Varicella VirusDocument8 pages(R) Varicella VirusEkkim Al KindiNo ratings yet
- Fped 09 599500Document8 pagesFped 09 599500Safira SalsabilaNo ratings yet
- Tambahan TransleteDocument9 pagesTambahan TransleteRamadhana PutraNo ratings yet
- An Observational Study of Febrile Seizures: The Importance of Viral Infection and ImmunizationDocument6 pagesAn Observational Study of Febrile Seizures: The Importance of Viral Infection and Immunizationnavali rahmaNo ratings yet
- Fiebre Sin Foco 0-36 MesesDocument28 pagesFiebre Sin Foco 0-36 MesesdanielentuxtlaNo ratings yet
- Breastfeeding Is Associated With Upward Social MobDocument4 pagesBreastfeeding Is Associated With Upward Social Mobdavidisnice123No ratings yet
- Atagi Recommendations On Pfizer Covid 19 Vaccine Use in Children Aged 5 To 11 YearsDocument11 pagesAtagi Recommendations On Pfizer Covid 19 Vaccine Use in Children Aged 5 To 11 YearsGanesh SahathevanNo ratings yet
- Risk Factors for Childhood TuberculosisDocument5 pagesRisk Factors for Childhood TuberculosisAnthony Huaman MedinaNo ratings yet
- Genetics and The Evaluation of The Febrile Child: EditorialDocument2 pagesGenetics and The Evaluation of The Febrile Child: EditorialYRRVNo ratings yet
- Eyes and EarsDocument7 pagesEyes and EarsNeenya SisonNo ratings yet
- Vital sign predictors of severe influenzaDocument11 pagesVital sign predictors of severe influenzaDesiska PriciliaNo ratings yet
- Key Clinical Research Priorities For The Pediatric Community During The COVID-19 PandemicDocument3 pagesKey Clinical Research Priorities For The Pediatric Community During The COVID-19 PandemicnpidasNo ratings yet
- Effects of One-Dose Varicella Vaccination On Disease Severity in Children During Outbreaks in Seoul, KoreaDocument5 pagesEffects of One-Dose Varicella Vaccination On Disease Severity in Children During Outbreaks in Seoul, KoreaNur WahyuningsihNo ratings yet
- International Journal of Pediatric Research Ijpr 9 112Document12 pagesInternational Journal of Pediatric Research Ijpr 9 112VsbshNo ratings yet
- HHS Public AccessDocument21 pagesHHS Public AccessA AnonimyNo ratings yet
- Risk of Seizures After Immunization in Children With Epilepsy: A Risk Interval AnalysisDocument7 pagesRisk of Seizures After Immunization in Children With Epilepsy: A Risk Interval AnalysisReziNo ratings yet
- Articulo NorovirusDocument2 pagesArticulo Norovirusmarianagonzalezgil11No ratings yet
- BongDocument1 pageBongRod Reynon BorceNo ratings yet
- en Measles Immunization and Vitamin A For PDocument6 pagesen Measles Immunization and Vitamin A For PM Iqbal TriansyahNo ratings yet
- Accepted ManuscriptDocument19 pagesAccepted Manuscripthilman lesmanaNo ratings yet
- 12701-50629-1-PB-1 AnakDocument4 pages12701-50629-1-PB-1 AnakAni RoseNo ratings yet
- Level of Exposure To Childhood Tuberculosis in Household Contacts With Adult Pulmonary TuberculosisDocument6 pagesLevel of Exposure To Childhood Tuberculosis in Household Contacts With Adult Pulmonary Tuberculosisdapajiangu asniNo ratings yet
- Typhoid fever disease burden and antimicrobial resistance in five Asian countriesDocument4 pagesTyphoid fever disease burden and antimicrobial resistance in five Asian countriesPutu SuartiniNo ratings yet
- VaccinestudiesDocument21 pagesVaccinestudiesapi-277588360No ratings yet
- 08 0119 PDFDocument8 pages08 0119 PDFAnailil MoralesNo ratings yet
- Prevalence and Causes of Childhood Urticaria: EditorialDocument2 pagesPrevalence and Causes of Childhood Urticaria: EditorialPutri Juita KhairatihNo ratings yet
- Typhoid Fever in Children Aged Less Than 5 Years: The Lancet August 1999Document5 pagesTyphoid Fever in Children Aged Less Than 5 Years: The Lancet August 1999Marian SplashNo ratings yet
- Jurnal 2Document11 pagesJurnal 2KikiNurAqidahNo ratings yet
- Health Effects in Vaccinated Versus Unvaccinated ChildrenDocument11 pagesHealth Effects in Vaccinated Versus Unvaccinated ChildrenMahesh JayaramanNo ratings yet
- Neumococo Minesota 2014Document10 pagesNeumococo Minesota 2014Milyta1092No ratings yet
- ECPE-03-SI-0012 Covid 19Document3 pagesECPE-03-SI-0012 Covid 19ijklmnopqurstNo ratings yet
- Part II - The Myth That Vaccination Equals ImmunizationDocument18 pagesPart II - The Myth That Vaccination Equals ImmunizationGary Null100% (4)
- Pharyngitis Case ReportDocument4 pagesPharyngitis Case ReportMelissa TiofanNo ratings yet
- Tuberculosis in Infants and ChildrenDocument29 pagesTuberculosis in Infants and ChildrenAnisah TifaniNo ratings yet
- 1 s2.0 S0929664621003892 MainDocument8 pages1 s2.0 S0929664621003892 Mainrheynamaulidar rumoninNo ratings yet
- Research Paper On Child VaccinationsDocument7 pagesResearch Paper On Child Vaccinationspwvgqccnd100% (1)
- Brief Education To Increase Uptake of Influenza Vaccine Among Pregnant Women: A Study Protocol For A Randomized Controlled TrialDocument7 pagesBrief Education To Increase Uptake of Influenza Vaccine Among Pregnant Women: A Study Protocol For A Randomized Controlled TrialTopan AzzuriniNo ratings yet
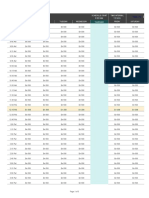
- Class Schedule: Schedule Start Time IntervalDocument3 pagesClass Schedule: Schedule Start Time IntervalPatrick TeodoroNo ratings yet
- Cba Edukasi PasienDocument5 pagesCba Edukasi Pasien419022 MELA ANANDA PUTRIANANo ratings yet
- Data Pengamatan Kelas ADocument39 pagesData Pengamatan Kelas A419022 MELA ANANDA PUTRIANANo ratings yet
- Dampak Jangka Panjang Dan Manfaat CBADocument12 pagesDampak Jangka Panjang Dan Manfaat CBA419022 MELA ANANDA PUTRIANANo ratings yet
- 06 11 2020 12.31.57Document3 pages06 11 2020 12.31.57419022 MELA ANANDA PUTRIANANo ratings yet
- Uti AimjDocument16 pagesUti AimjRoberto López Mata100% (1)
- Optimizing AB PharmacodynamicsDocument10 pagesOptimizing AB PharmacodynamicsFransisca Dhani KurniasihNo ratings yet
- DEXAMETHASONEDocument10 pagesDEXAMETHASONE419022 MELA ANANDA PUTRIANANo ratings yet
- DrycoughbookchapterDocument6 pagesDrycoughbookchapterhbjnjnsNo ratings yet
- Kardiovaskular 1Document92 pagesKardiovaskular 1419022 MELA ANANDA PUTRIANANo ratings yet
- A Review of Opioid Prescription in A Teaching Hospital in ColombiaDocument6 pagesA Review of Opioid Prescription in A Teaching Hospital in Colombia419022 MELA ANANDA PUTRIANANo ratings yet
- Fluconazol Isk AnakDocument3 pagesFluconazol Isk Anak419022 MELA ANANDA PUTRIANANo ratings yet
- Adult urinary tract infectionsDocument5 pagesAdult urinary tract infectionsBayu TrigunaNo ratings yet
- Case Write Up 3Document4 pagesCase Write Up 3E learningNo ratings yet
- Influenza Teaching Current Update 2023 by Dr.T.V.Rao MDDocument100 pagesInfluenza Teaching Current Update 2023 by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- The Reemergent 1977 H1N1 Strain and The Gain-of-Function DebateDocument6 pagesThe Reemergent 1977 H1N1 Strain and The Gain-of-Function Debateasta lavistaNo ratings yet
- Vaccine Administration Record For Children and TeensDocument2 pagesVaccine Administration Record For Children and TeensGian Franco ApesNo ratings yet
- Vaccinations: Slam Shraf AhmyDocument11 pagesVaccinations: Slam Shraf AhmyFahad Alkenani100% (1)
- Summary of Product Characteristics for Influenza VaccineDocument28 pagesSummary of Product Characteristics for Influenza VaccineEllaNo ratings yet
- Storage Conditions Vital for Pharmaceutical Product StabilityDocument18 pagesStorage Conditions Vital for Pharmaceutical Product StabilityVer OnischNo ratings yet
- RNSG 1260 - Well-Child Simulation: Medication WorksheetDocument4 pagesRNSG 1260 - Well-Child Simulation: Medication WorksheetelizabethenNo ratings yet
- Conscientious Objector Info Pack Part 2Document194 pagesConscientious Objector Info Pack Part 2Shot_infoNo ratings yet
- Flumist Case StudyDocument22 pagesFlumist Case StudyDeva Prayag0% (1)
- The Safety of Influenza Vaccines in Children An Institute For Vaccine Safety White PaperDocument67 pagesThe Safety of Influenza Vaccines in Children An Institute For Vaccine Safety White Papermaheshmuralinair6No ratings yet
- CBER List of Licensed Biologics Products 4-12-2019Document16 pagesCBER List of Licensed Biologics Products 4-12-2019PRIYANKA BABUNo ratings yet
- Vaccine: Aiko Shono, Masahide KondoDocument6 pagesVaccine: Aiko Shono, Masahide KondoAntonio MoncayoNo ratings yet
- Flu Vaccine RecommendationsDocument26 pagesFlu Vaccine Recommendationscharanmann9165No ratings yet
- Flumist PiDocument4 pagesFlumist Pijasonm2282No ratings yet
- Produksi VaksinDocument25 pagesProduksi Vaksinkehie HananielNo ratings yet
- Immunization Record FormDocument4 pagesImmunization Record FormLeonardo Zikri ArmandaNo ratings yet
- The Scientific Manipulation of Our Reality Noworldsystem - ComDocument29 pagesThe Scientific Manipulation of Our Reality Noworldsystem - ComferalmuttNo ratings yet
- Influenza y ParainfluenzaDocument14 pagesInfluenza y ParainfluenzaLaura Natalia Cordoba RiañoNo ratings yet
- Nurse Practitioner - Fitzgerald, Margaret A.Document535 pagesNurse Practitioner - Fitzgerald, Margaret A.Barbara Yoon95% (22)
- AstraZeneca Therapy R&D Pipeline Summary - December 7, 2007Document10 pagesAstraZeneca Therapy R&D Pipeline Summary - December 7, 2007jennabushNo ratings yet
- APhA Immunization Module 3Document49 pagesAPhA Immunization Module 3Gerald GamboaNo ratings yet
- Tugas Kelompok - Menganalisis Jurnal - Meet 3 - Kelompok 3Document4 pagesTugas Kelompok - Menganalisis Jurnal - Meet 3 - Kelompok 3Rizki HandayaniNo ratings yet
- 2005-10-04Document12 pages2005-10-04The University Daily KansanNo ratings yet
- InfluenzaDocument2 pagesInfluenzaSheva ChauNo ratings yet
- H1n1vaers InjectedDocument727 pagesH1n1vaers Injectedx2634No ratings yet
- Human Body Temperature and New Approaches To ConstDocument21 pagesHuman Body Temperature and New Approaches To ConstCarlos Apodman BellaNo ratings yet
- Influenza VaccineDocument59 pagesInfluenza VaccineVernon MonteiroNo ratings yet
- Influenza - NEJMGroup - Collection PDFDocument106 pagesInfluenza - NEJMGroup - Collection PDFPanayiotis StavroulakisNo ratings yet
- Protocol of Clinical StudyDocument54 pagesProtocol of Clinical StudyPalak GuptaNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)