You might also like
- Anatomy and Physiology The Unity of Form and Function 8th Edition Saladin Solutions Manual Full Chapter PDFDocument27 pagesAnatomy and Physiology The Unity of Form and Function 8th Edition Saladin Solutions Manual Full Chapter PDFhuonghuyen2cp9ez100% (12)
- Stellabotte, Fred Straub, Rachel - Weight Training Without Injury Over 350 Step-By-Step Pictures Including What Not To Do! - Regalis Publishing (2016)Document308 pagesStellabotte, Fred Straub, Rachel - Weight Training Without Injury Over 350 Step-By-Step Pictures Including What Not To Do! - Regalis Publishing (2016)Tom PaschalisNo ratings yet
- Shoulder and Upper Extremity InjuriesDocument107 pagesShoulder and Upper Extremity InjuriesStaen KisNo ratings yet
- Preseason Strength Training For Rugby Union - The General and Speci C Preparatory PhasesDocument9 pagesPreseason Strength Training For Rugby Union - The General and Speci C Preparatory PhasesHani Assi100% (1)
- EX-150 Electronic Experiment Kit PDFDocument163 pagesEX-150 Electronic Experiment Kit PDFpkrajniNo ratings yet
- Movement Analysis of Kicking A Soccer Ball: Kendra Alberts - Kyleah Bowder - Kelsey TimmermanDocument15 pagesMovement Analysis of Kicking A Soccer Ball: Kendra Alberts - Kyleah Bowder - Kelsey TimmermanSYAFINAS SALAMNo ratings yet
- Rehabilitation in OsteoarthritisDocument6 pagesRehabilitation in OsteoarthritisnudyanbethaNo ratings yet
- Determinants of GaitDocument35 pagesDeterminants of GaitAnup Pednekar50% (2)
- Osteoarthritis of The Knee Exercises PDFDocument4 pagesOsteoarthritis of The Knee Exercises PDFPooja jainNo ratings yet
- Guide To The Dissection of The Dog, 8th EditionDocument346 pagesGuide To The Dissection of The Dog, 8th Editionmaria da matosNo ratings yet
- 2012 Scapular-Focused Treatment in Patients With ShoulderDocument13 pages2012 Scapular-Focused Treatment in Patients With ShoulderIsrael Matías Chandia Ramírez100% (1)
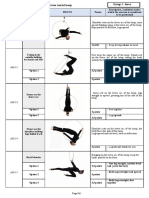
- Appendix 2 Compulsory Exercises Aerial Hoop 2018 EngDocument28 pagesAppendix 2 Compulsory Exercises Aerial Hoop 2018 Engtito1628100% (1)
- Ajnr 7 4 2 PDFDocument8 pagesAjnr 7 4 2 PDFniaNo ratings yet
- Effectiveness of Exercise and Cyriax Physiotherapy in Patients With Tennis Elbow (2012)Document8 pagesEffectiveness of Exercise and Cyriax Physiotherapy in Patients With Tennis Elbow (2012)Sufi Muzahid HussainNo ratings yet
- To Compare The Effects of Maitland MobilizationDocument4 pagesTo Compare The Effects of Maitland MobilizationravichandragoudaNo ratings yet
- JCVJS 8 44Document6 pagesJCVJS 8 44Rvo ProductionNo ratings yet
- This Item Is The Archived Peer-Reviewed Author-Version ofDocument12 pagesThis Item Is The Archived Peer-Reviewed Author-Version ofK scuddsNo ratings yet
- ShoulderDocument4 pagesShoulderRadwa MostafaNo ratings yet
- Frozen Shoulder InjectionDocument10 pagesFrozen Shoulder InjectionTariq Maqsood KhanNo ratings yet
- Effectiveness of Kinesiologic Tape Application in Rotator Cuff InjuriesDocument6 pagesEffectiveness of Kinesiologic Tape Application in Rotator Cuff InjuriesdarisNo ratings yet
- Ijpr 2022 156Document5 pagesIjpr 2022 156winda athyaNo ratings yet
- Bmri2022 4133883Document8 pagesBmri2022 4133883aaNo ratings yet
- HombroDocument10 pagesHombroDr. AlonsoNo ratings yet
- ptrs009 03 03 PDFDocument6 pagesptrs009 03 03 PDFGusti Ayu KrisnayantiNo ratings yet
- 7 Cochrane - UltrasoundGuided Percutaneous Electrolysis andDocument10 pages7 Cochrane - UltrasoundGuided Percutaneous Electrolysis andFranco Suazo MoralesNo ratings yet
- What Is Better For Rotator Cuff Tendinopathy: Dextrose Prolotherapy, Platelet-Rich Plasma, or Corticosteroid Injections? A Randomized Controlled StudyDocument7 pagesWhat Is Better For Rotator Cuff Tendinopathy: Dextrose Prolotherapy, Platelet-Rich Plasma, or Corticosteroid Injections? A Randomized Controlled StudyFreddy ChurataNo ratings yet
- A Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategie - 20170730120051Document8 pagesA Blinded, Randomized, Controlled Trial Assessing Conservative Management Strategie - 20170730120051sebafigueroa94No ratings yet
- Physiotherapeutic Management of Adhesive Capsulitis: A Review of LiteratureDocument9 pagesPhysiotherapeutic Management of Adhesive Capsulitis: A Review of LiteratureevaNo ratings yet
- MET Vs ConventionalDocument6 pagesMET Vs ConventionalPoorvin ShahNo ratings yet
- Manipulation Under Anesthesia Versus Physiotherapy Treatment in Stage Two of A Frozen Shoulder: A Study Protocol For A Randomized Controlled TrialDocument12 pagesManipulation Under Anesthesia Versus Physiotherapy Treatment in Stage Two of A Frozen Shoulder: A Study Protocol For A Randomized Controlled TrialKristiyan winniNo ratings yet
- Full TextDocument7 pagesFull TextJuan Pablo Casanova AnguloNo ratings yet
- Functional Treatment Versus Plaster For Simple Elbow Dislocations (Funcsie) : A Randomized TrialDocument7 pagesFunctional Treatment Versus Plaster For Simple Elbow Dislocations (Funcsie) : A Randomized TrialTekhaDwiNo ratings yet
- Randomizado-Cetoprofeno e Polisacarideo FonoDocument9 pagesRandomizado-Cetoprofeno e Polisacarideo FonoELONo ratings yet
- Clinical StudyDocument8 pagesClinical Studylilis pratiwiNo ratings yet
- 1 s2.0 S0031940610001100 MainDocument11 pages1 s2.0 S0031940610001100 MainkkkjaegiNo ratings yet
- Physiotherapy of Adhesive Capsulitis: A Review: Kaushik GuhaDocument5 pagesPhysiotherapy of Adhesive Capsulitis: A Review: Kaushik GuhaVeby JabirNo ratings yet
- Clinical ResearcheffectsDocument7 pagesClinical ResearcheffectsJackielyn C. AportaderaNo ratings yet
- Jurnal Rms 3Document9 pagesJurnal Rms 3zuhuda piliNo ratings yet
- Intra-Articular Injection, Subacromial Injection, and Hydrodilatation For Primary Frozen Shoulder: A Randomized Clinical TrialDocument8 pagesIntra-Articular Injection, Subacromial Injection, and Hydrodilatation For Primary Frozen Shoulder: A Randomized Clinical TrialAbhishek JirelNo ratings yet
- 03IJPHY840Document6 pages03IJPHY840Dzihan NabilahNo ratings yet
- Stuck-Moving Needle Acupuncture Myofascial Trigger Point To Treat Idiopathic Frozen Shoulder: Study Protocol For A Randomized Controlled TrialDocument13 pagesStuck-Moving Needle Acupuncture Myofascial Trigger Point To Treat Idiopathic Frozen Shoulder: Study Protocol For A Randomized Controlled TrialCarl MacCordNo ratings yet
- Arthritis Care Research - 2016 - de Rooij - Efficacy of Tailored Exercise Therapy On Physical Functioning in PatientsDocument10 pagesArthritis Care Research - 2016 - de Rooij - Efficacy of Tailored Exercise Therapy On Physical Functioning in PatientsToli kkakrNo ratings yet
- F0602044753 PDFDocument7 pagesF0602044753 PDFArif Adi FatuhrokhmanNo ratings yet
- Quadriceps Arthrogenic Muscle Inhibition: The Effects of Experimental Knee Joint Effusion On Motor Cortex ExcitabilityDocument7 pagesQuadriceps Arthrogenic Muscle Inhibition: The Effects of Experimental Knee Joint Effusion On Motor Cortex ExcitabilityPedro SimõesNo ratings yet
- Effectiveness of Therapeutic Ultrasound in Adhesive Capsulitis PDFDocument6 pagesEffectiveness of Therapeutic Ultrasound in Adhesive Capsulitis PDFlalududiNo ratings yet
- Comparison of Mulligan Technique Versus Muscle Energy Technique in Patients (Ingles)Document5 pagesComparison of Mulligan Technique Versus Muscle Energy Technique in Patients (Ingles)mauricio castroNo ratings yet
- 291-297 Jopct1Document7 pages291-297 Jopct1efi hudriahNo ratings yet
- The Effectiveness of The Combination of Neuromuscular Taping (NMT) and Codman Pendulum Exercise To Improve The Functional Ability of The Shoulder in Patients With Frozen ShouldersDocument3 pagesThe Effectiveness of The Combination of Neuromuscular Taping (NMT) and Codman Pendulum Exercise To Improve The Functional Ability of The Shoulder in Patients With Frozen ShouldersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Clinical Study: Autologous Blood Injection and Wrist Immobilisation For Chronic Lateral EpicondylitisDocument6 pagesClinical Study: Autologous Blood Injection and Wrist Immobilisation For Chronic Lateral EpicondylitistriptykhannaNo ratings yet
- A Review of Current Treatment Options For CoccygodyniaDocument8 pagesA Review of Current Treatment Options For CoccygodyniaClara ViMiNo ratings yet
- Poster PapersDocument262 pagesPoster PapersLeonardo RodríguezNo ratings yet
- Toorthj 11 327Document8 pagesToorthj 11 327Apri PerdanaNo ratings yet
- A Comparative Study To Find Out The Effects of Capsular Stretching Over Muscle Energy Technique in The Management of Frozen ShoulderDocument50 pagesA Comparative Study To Find Out The Effects of Capsular Stretching Over Muscle Energy Technique in The Management of Frozen ShoulderjojiNo ratings yet
- Effect of Cupping Massage and Modified Spinal Decompression Therapy With Exercise Therapy in Neck Radiculopathy SyndromeDocument9 pagesEffect of Cupping Massage and Modified Spinal Decompression Therapy With Exercise Therapy in Neck Radiculopathy SyndromeKhadiga AhmadNo ratings yet
- TheEffectofDeepFrictionMassageversus PDFDocument8 pagesTheEffectofDeepFrictionMassageversus PDFRiniaridhaNo ratings yet
- LaserDocument8 pagesLaserALİ YAVUZ KARAHANNo ratings yet
- Mccre Esh 2013Document1 pageMccre Esh 2013Francisco Javier Luza RamosNo ratings yet
- CapsulitisDocument12 pagesCapsulitisLuis Briones Lau.LiNo ratings yet
- Efficacy of High-Intensity Home Mechanical Stretch Therapy For Treatment of Shoulder Stiffness A Retrospective Review PDFDocument9 pagesEfficacy of High-Intensity Home Mechanical Stretch Therapy For Treatment of Shoulder Stiffness A Retrospective Review PDFDaniel Ruiz VallejoNo ratings yet
- DexamethasoneDocument12 pagesDexamethasoneDenilson BarbosaNo ratings yet
- A Regenerative Interventional Approach To The Management of Degenerative Low Back PainDocument16 pagesA Regenerative Interventional Approach To The Management of Degenerative Low Back PainAthenaeum Scientific PublishersNo ratings yet
- PNF Ombro 05Document19 pagesPNF Ombro 05Isaias AlmeidaNo ratings yet
- BBRC Vol 14 No 04 2021-80Document5 pagesBBRC Vol 14 No 04 2021-80Dr Sharique AliNo ratings yet
- s12891 019 2796 5 PDFDocument22 pagess12891 019 2796 5 PDFAndré MesquitaNo ratings yet
- Effects of Heavy Slow Resistance Training Combined With Corticosteroid Injections or Tendon Needling in Patients With Lateral Elbow TendinopathyDocument10 pagesEffects of Heavy Slow Resistance Training Combined With Corticosteroid Injections or Tendon Needling in Patients With Lateral Elbow TendinopathyaaNo ratings yet
- Assessment of Rotator Cuff Muscle Strength and Shoulder Rotation Range of Motion in Subjects With Lateral EpicondylitisDocument5 pagesAssessment of Rotator Cuff Muscle Strength and Shoulder Rotation Range of Motion in Subjects With Lateral Epicondylitispedrovsky702No ratings yet
- 1471-2474-13-81 KonsulDocument7 pages1471-2474-13-81 KonsulGustan AriadiNo ratings yet
- Ultrasound Features of Adhesive CapsulitisDocument15 pagesUltrasound Features of Adhesive CapsulitisMarco Antonio Morales OsorioNo ratings yet
- Sports Hernia and Athletic Pubalgia: Diagnosis and TreatmentFrom EverandSports Hernia and Athletic Pubalgia: Diagnosis and TreatmentDavid R. DiduchNo ratings yet
- Xbox Accessories en PT FR Es - Us Ca LatamDocument44 pagesXbox Accessories en PT FR Es - Us Ca LatamMarcus YoonNo ratings yet
- Ryuichi Sakamoto Merry Christmas MR LawrenceDocument6 pagesRyuichi Sakamoto Merry Christmas MR LawrenceMarcus YoonNo ratings yet
- George Winston Canon VariationDocument2 pagesGeorge Winston Canon VariationMarcus YoonNo ratings yet
- Classical Music Mp3 DownloadDocument5 pagesClassical Music Mp3 DownloadMarcus YoonNo ratings yet
- Adhesive Capsulitis Anew Management Protocolto Improve Passive Rangeof MotionDocument6 pagesAdhesive Capsulitis Anew Management Protocolto Improve Passive Rangeof MotionMarcus YoonNo ratings yet
- Indications For Hydrodilatation For Frozen ShoulderDocument7 pagesIndications For Hydrodilatation For Frozen ShoulderMarcus YoonNo ratings yet
- Your Coronavirus Test Is Positive. Maybe It Shouldn't BeDocument6 pagesYour Coronavirus Test Is Positive. Maybe It Shouldn't BeMarcus YoonNo ratings yet
- 'Pavane+pour+une+Infante+Defunte'+ (Contributed+by+L Meyer) +-+might+not+be+legal+to+download+into+franceDocument4 pages'Pavane+pour+une+Infante+Defunte'+ (Contributed+by+L Meyer) +-+might+not+be+legal+to+download+into+franceMarcus YoonNo ratings yet
- ShingrixDocument6 pagesShingrixMarcus YoonNo ratings yet
- 노바벡스 효과와 안전성Document5 pages노바벡스 효과와 안전성Marcus YoonNo ratings yet
- 노바벡스 효과와 안전성Document5 pages노바벡스 효과와 안전성Marcus YoonNo ratings yet
- Covid Vaccine Adjuvant Matrix MDocument13 pagesCovid Vaccine Adjuvant Matrix MMarcus YoonNo ratings yet
- Med 2047 - Dewit Chapter Pretests Directions: Answer The Following Multiple-Choice QuestionsDocument9 pagesMed 2047 - Dewit Chapter Pretests Directions: Answer The Following Multiple-Choice QuestionsMarcelyn Chupoco CataligNo ratings yet
- Pemeriksaan Fisik Elbow (Lanjutan) : Presentan: Dr. Sylvia Evelyn Aritonang Pembimbing: Dr. Tri Damiati Pandji, SPKFRDocument45 pagesPemeriksaan Fisik Elbow (Lanjutan) : Presentan: Dr. Sylvia Evelyn Aritonang Pembimbing: Dr. Tri Damiati Pandji, SPKFRsingle_ladyNo ratings yet
- Anatomy Lecture 3: (The Muscular System)Document35 pagesAnatomy Lecture 3: (The Muscular System)Marikit2012No ratings yet
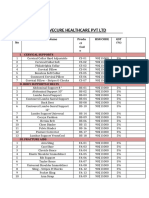
- Drivecure Healthcare PVT LTD: S. No Product Name Produ CT Cod e HSN Code GST (%)Document4 pagesDrivecure Healthcare PVT LTD: S. No Product Name Produ CT Cod e HSN Code GST (%)DRIVECURENo ratings yet
- وضعيات التصوير الشعاعي 1Document30 pagesوضعيات التصوير الشعاعي 1عبدالرحمن الاريانيNo ratings yet
- Sciatica BookDocument13 pagesSciatica BookKostas GhinisNo ratings yet
- Post Parturition Back PainDocument35 pagesPost Parturition Back PainARF TYONo ratings yet
- Epidemiology of Injuries in The Philippines An Analysis of Secondary DataDocument7 pagesEpidemiology of Injuries in The Philippines An Analysis of Secondary DataPriscilla Jean UmenganNo ratings yet
- Paley2002 Anatomical AxisDocument37 pagesPaley2002 Anatomical Axisprajwal guptaNo ratings yet
- Vascular Anatomy and Blood Supply To The Femoral Head: Marcin Zlotorowicz and Jaroslaw CzubakDocument8 pagesVascular Anatomy and Blood Supply To The Femoral Head: Marcin Zlotorowicz and Jaroslaw CzubakAzmi FarhadiNo ratings yet
- Rehab Medik LBPDocument19 pagesRehab Medik LBPWikha AprianNo ratings yet
- Anatomy of Anterior Cruciate LigamentDocument60 pagesAnatomy of Anterior Cruciate LigamentYusuf BrilliantNo ratings yet
- GROUP B Muscle InjuryDocument26 pagesGROUP B Muscle InjurySandy GodartNo ratings yet
- 2.supracondylar Humerus FracturesDocument26 pages2.supracondylar Humerus FracturesDabessa MosissaNo ratings yet
- ISAKMetry - Edilberto - Aguiar - Restricted - 11-13-2022 - Edilberto AguiarDocument3 pagesISAKMetry - Edilberto - Aguiar - Restricted - 11-13-2022 - Edilberto Aguiar012 timeNo ratings yet
- Pott's DiseaseDocument30 pagesPott's DiseaseBipin SolankiNo ratings yet
- Embedded and Impacted TeethDocument2 pagesEmbedded and Impacted TeethAhmed MawardiNo ratings yet
- Exercise Therapy AssignmentDocument13 pagesExercise Therapy AssignmentApoorvNo ratings yet
- The Sliding Filament TheoryDocument4 pagesThe Sliding Filament TheoryJinno VeldadNo ratings yet
- Regenerative Injection Therapy: (Prolotherapy)Document7 pagesRegenerative Injection Therapy: (Prolotherapy)M Al KautsarNo ratings yet
- Movement Analysis ProjectDocument13 pagesMovement Analysis ProjectPatrickNo ratings yet