You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Reslaj: Religion Education Social Laa Roiba JournalDocument19 pagesReslaj: Religion Education Social Laa Roiba Journalfebrian rahmatNo ratings yet
- Studi Komparasi Antara Teori Victor Frankl, Ester Ahn Kim Dan Elisabeth Kubler-Ross Tentang Kematian Bagi Konstruksi Pendampingan PastoralDocument19 pagesStudi Komparasi Antara Teori Victor Frankl, Ester Ahn Kim Dan Elisabeth Kubler-Ross Tentang Kematian Bagi Konstruksi Pendampingan Pastoralfebrian rahmatNo ratings yet
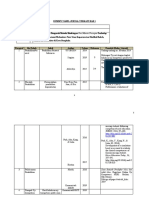
- Dummy Tabel Jurnal Terkait Bab 1Document9 pagesDummy Tabel Jurnal Terkait Bab 1febrian rahmatNo ratings yet
- Gambaran Professional Quality of Life Proqol GuruDocument7 pagesGambaran Professional Quality of Life Proqol Gurufebrian rahmatNo ratings yet
- Tests of Between-Subjects EffectsDocument3 pagesTests of Between-Subjects Effectsfebrian rahmatNo ratings yet
- Within-Subjects Factors: B B B B B B B BDocument7 pagesWithin-Subjects Factors: B B B B B B B Bfebrian rahmatNo ratings yet
- Elisabeth Ku Bler-Ross and The "Five Stages" Model in A Sampling of Recent Textbooks Published in 10 Countries Outside The United StatesDocument31 pagesElisabeth Ku Bler-Ross and The "Five Stages" Model in A Sampling of Recent Textbooks Published in 10 Countries Outside The United Statesfebrian rahmatNo ratings yet
- I'm Putting My Trust in Their HandsDocument8 pagesI'm Putting My Trust in Their Handsfebrian rahmatNo ratings yet
- Xviii + 135 Pages + Tables + Drawings + Schematics + AttachmentsDocument2 pagesXviii + 135 Pages + Tables + Drawings + Schematics + Attachmentsfebrian rahmatNo ratings yet
- 1465-Article Text-5566-1-10-20201127Document8 pages1465-Article Text-5566-1-10-20201127febrian rahmatNo ratings yet
- Trust Board: Board of Direction:: 9 No. 2 April - June 2015 Published Every 3 Month ISSN 1978 - 3744Document12 pagesTrust Board: Board of Direction:: 9 No. 2 April - June 2015 Published Every 3 Month ISSN 1978 - 3744febrian rahmatNo ratings yet
- Job Satisfaction and Career Intention of Australian General Practice Nurses: A Cross-Sectional SurveyDocument11 pagesJob Satisfaction and Career Intention of Australian General Practice Nurses: A Cross-Sectional Surveyfebrian rahmatNo ratings yet
- Eclinicalmedicine: Dianne Zakaria, Amanda Shaw, Lin XieDocument14 pagesEclinicalmedicine: Dianne Zakaria, Amanda Shaw, Lin Xiefebrian rahmatNo ratings yet
- Supervisi Berjenjang Di Era Pandemi Covid-19 Dalam Manajemen KeperawatanDocument10 pagesSupervisi Berjenjang Di Era Pandemi Covid-19 Dalam Manajemen Keperawatanfebrian rahmatNo ratings yet
- Ismail 2020Document10 pagesIsmail 2020febrian rahmatNo ratings yet
- 10 1016@j Clnu 2019 10 028Document6 pages10 1016@j Clnu 2019 10 028febrian rahmatNo ratings yet
- Johnson 2017Document4 pagesJohnson 2017febrian rahmatNo ratings yet
- Ruparelia 2019Document1 pageRuparelia 2019febrian rahmatNo ratings yet
- 23PH61 dcbH5Z t12Cb4 686q4u 310730Document7 pages23PH61 dcbH5Z t12Cb4 686q4u 310730febrian rahmatNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DOH Devolution Transition Plan 2022-2024Document589 pagesDOH Devolution Transition Plan 2022-2024Kristine De Luna TomananNo ratings yet
- Normal and Abnormal Present IonDocument31 pagesNormal and Abnormal Present IondeemNo ratings yet
- Rachel Elizabeth Jones Resume 1-17Document2 pagesRachel Elizabeth Jones Resume 1-17api-344942802No ratings yet
- Learning PlanDocument7 pagesLearning Planapi-283070240No ratings yet
- Narrowing Achievement Gap For Low Income KidsDocument80 pagesNarrowing Achievement Gap For Low Income KidsEducation JusticeNo ratings yet
- Cover Letters For Volunteer NurseDocument1 pageCover Letters For Volunteer Nursehanna_ong_2100% (2)
- Research General HospitalDocument14 pagesResearch General HospitalWILJHON EZROM BAUTISTANo ratings yet
- Knucle JointDocument2 pagesKnucle Joint12ranjNo ratings yet
- The Transplantation of Human Organs (Amendment) Act, 2011Document34 pagesThe Transplantation of Human Organs (Amendment) Act, 2011kamtiabhilash529No ratings yet
- Introduction To Developmental Anatomy: Dr. Nitin VishwakarmaDocument78 pagesIntroduction To Developmental Anatomy: Dr. Nitin Vishwakarmakissmyasthma69No ratings yet
- Surgical InstrumentsDocument7 pagesSurgical InstrumentsAna BananaNo ratings yet
- Sample Chapter 17Document20 pagesSample Chapter 17Fatimah Shellya ShahabNo ratings yet
- Coursebook-English For Nurses PDFDocument49 pagesCoursebook-English For Nurses PDFhimmatul aliyahNo ratings yet
- 11 PD Drug Interaction EngDocument14 pages11 PD Drug Interaction EngshahrukhziaNo ratings yet
- Stellate, Firm, Not Clearly Delineated From Surrounding TissueDocument1 pageStellate, Firm, Not Clearly Delineated From Surrounding TissueDestinee CapleNo ratings yet
- Senior-Loken Syndrome With Rare Manifestations: A Case ReportDocument5 pagesSenior-Loken Syndrome With Rare Manifestations: A Case ReportAndrie GunawanNo ratings yet
- Power Point Bio Ethical 2Document19 pagesPower Point Bio Ethical 2lkristinNo ratings yet
- TRIAGE and MCI 083104Document66 pagesTRIAGE and MCI 083104Nom Nom100% (1)
- Ebook First Aid For The Usmle Step 1 2023 33Rd Edition PDF Full Chapter PDFDocument67 pagesEbook First Aid For The Usmle Step 1 2023 33Rd Edition PDF Full Chapter PDFchristopher.feeney571100% (28)
- Trisomy 21Document17 pagesTrisomy 21Paul Michael BaguhinNo ratings yet
- AP PG Mock Part 1Document234 pagesAP PG Mock Part 1TargetNo ratings yet
- Bevacizumab in Combination With Chemotherapy For The Treatment of Advanced Ovarian CancerDocument13 pagesBevacizumab in Combination With Chemotherapy For The Treatment of Advanced Ovarian CancerPaulo Cesar Castañeda RuizNo ratings yet
- Plan of Dissertation-MadhaviDocument18 pagesPlan of Dissertation-MadhaviVijay ChhillarNo ratings yet
- Igich Emergency CommiteeDocument46 pagesIgich Emergency CommiteeSultan QuranmalNo ratings yet
- CANINE-Canine Elbow Joint Arthroscopy-Introduction and Descriptin of TechniqueDocument8 pagesCANINE-Canine Elbow Joint Arthroscopy-Introduction and Descriptin of Techniquetaner_soysurenNo ratings yet
- F. Daftar Pustaka (KIAN Lukman N 3)Document7 pagesF. Daftar Pustaka (KIAN Lukman N 3)Lukman SulistiyadiNo ratings yet
- Chapter 22 - Complications Occurring During LaborDocument6 pagesChapter 22 - Complications Occurring During LaborEunice CortésNo ratings yet
- Vaccination ChartDocument3 pagesVaccination ChartszawNo ratings yet
- OPT Plus Form 1 List of Preschoolers With Height Measurement and Identified Nutritional StatusDocument14 pagesOPT Plus Form 1 List of Preschoolers With Height Measurement and Identified Nutritional StatusMelanie Ordanel91% (11)
- Salman M., Roberto C. Heros, Edward R. Laws-Kempe's Operative Neurosurgery. Vol. I-II-Springer (2004)Document459 pagesSalman M., Roberto C. Heros, Edward R. Laws-Kempe's Operative Neurosurgery. Vol. I-II-Springer (2004)Silvia SanduNo ratings yet