You might also like
- Minimally Invasive Transcanal Removal of Attic CholesteatomaDocument7 pagesMinimally Invasive Transcanal Removal of Attic CholesteatomaAhmed HemdanNo ratings yet
- Endoscopicmanagement Ofcom&tympanoplastyDocument9 pagesEndoscopicmanagement Ofcom&tympanoplastyvipinNo ratings yet
- Timpanoplastia Tipo IDocument14 pagesTimpanoplastia Tipo ILuis De jesus SolanoNo ratings yet
- Beyond The Middle EarDocument12 pagesBeyond The Middle Earjay gauNo ratings yet
- Mastoidectomy and EpitympanectomyDocument18 pagesMastoidectomy and EpitympanectomyDrTarek Mahmoud Abo KammerNo ratings yet
- Canal Wall UP Mastoidecto MY: By: Dr. Aditya Tiwari, Resident, Dept. of ENTDocument90 pagesCanal Wall UP Mastoidecto MY: By: Dr. Aditya Tiwari, Resident, Dept. of ENTAdi SitaruNo ratings yet
- 90 217 1Document109 pages90 217 1jenishjsNo ratings yet
- Tympanoplasty Excellent Summary1Document29 pagesTympanoplasty Excellent Summary1DrMohmd ZidaanNo ratings yet
- Assessment of Anterior Tucking and Cartilage Support Tympanoplasty To Evaluate Graft Uptake and Hearing OutcomeDocument4 pagesAssessment of Anterior Tucking and Cartilage Support Tympanoplasty To Evaluate Graft Uptake and Hearing OutcomeAkanshaNo ratings yet
- Flexible Approach To TympanomastoidectomyDocument11 pagesFlexible Approach To Tympanomastoidectomyrahul varmaNo ratings yet
- Top of Page Patients and Methods Results Discussion Conclusion BibliographyDocument16 pagesTop of Page Patients and Methods Results Discussion Conclusion BibliographyentsrmcNo ratings yet
- VacioDocument17 pagesVacioKaren HolguinNo ratings yet
- Choanal AtresiaDocument8 pagesChoanal AtresiaDantowaluyo NewNo ratings yet
- Commonotologicsurgical Procedures: Clinical Decision-Making Pearls and The Role of ImagingDocument14 pagesCommonotologicsurgical Procedures: Clinical Decision-Making Pearls and The Role of ImagingyannecaNo ratings yet
- Congress Auricular Reconstruction AbstractsDocument92 pagesCongress Auricular Reconstruction AbstractsRocio RamirezNo ratings yet
- Choanal Atresia PDFDocument8 pagesChoanal Atresia PDFMonna Medani LysabellaNo ratings yet
- Revision OssiculoplastyDocument14 pagesRevision Ossiculoplastyapi-19500641No ratings yet
- ENT MCQforstudents AnswersDocument30 pagesENT MCQforstudents AnswersOlaNo ratings yet
- Alin PREZENTAREDocument32 pagesAlin PREZENTAREEdy MorarNo ratings yet
- Lateral Antrostomy For Max Sinus AugmentationDocument9 pagesLateral Antrostomy For Max Sinus AugmentationsevattapillaiNo ratings yet
- Mastoidectomy Intact Canal Wall ProcedureDocument13 pagesMastoidectomy Intact Canal Wall Proceduretaquiri12No ratings yet
- Jurnal THTDocument5 pagesJurnal THTSamuelRexyNo ratings yet
- Clinical Study of Retraction Pockets in Chronic Suppurative Otitis MediaDocument4 pagesClinical Study of Retraction Pockets in Chronic Suppurative Otitis Mediavivy iskandarNo ratings yet
- Ijo 25 063 PDFDocument8 pagesIjo 25 063 PDFyulianaNo ratings yet
- IJOHNS - 2016092715570757 Anababbabsbabbab Jaabbseuwhvegsushwbbs AjuzhehwuwuhDocument9 pagesIJOHNS - 2016092715570757 Anababbabsbabbab Jaabbseuwhvegsushwbbs AjuzhehwuwuhIsman SetiawanNo ratings yet
- Choanal Atresia1Document5 pagesChoanal Atresia1anurajoneNo ratings yet
- MastoidectomyDocument110 pagesMastoidectomySangam AdhikariNo ratings yet
- Https Emedicine - MedscapeDocument7 pagesHttps Emedicine - MedscapekarnoNo ratings yet
- Residual CholesteatomDocument6 pagesResidual CholesteatomikajuNo ratings yet
- Management of Chronic SuppurativeDocument8 pagesManagement of Chronic SuppurativeShebaTariganNo ratings yet
- Milo Ro 2010Document12 pagesMilo Ro 2010abdullah özelNo ratings yet
- Original Research Article: Amitkumar Rathi, Vinod Gite, Sameer Bhargava, Neeraj ShettyDocument8 pagesOriginal Research Article: Amitkumar Rathi, Vinod Gite, Sameer Bhargava, Neeraj ShettyAkanshaNo ratings yet
- Updateonmaxillarysinus Augmentation: Natasha Bhalla,, Harry DymDocument14 pagesUpdateonmaxillarysinus Augmentation: Natasha Bhalla,, Harry DymAlejandro FereñoNo ratings yet
- Tuberculous Otomastoiditis: Analysis of Otological TB With Intact Tympanic MembraneDocument8 pagesTuberculous Otomastoiditis: Analysis of Otological TB With Intact Tympanic MembraneNandini GuptaNo ratings yet
- Reliability of Two Surgical Methods For Oroantral Communication Closure A Clinical Study of 20 Patients 2161 119X.1000113Document4 pagesReliability of Two Surgical Methods For Oroantral Communication Closure A Clinical Study of 20 Patients 2161 119X.1000113AndreHidayatNo ratings yet
- Complications of OtoplastyDocument10 pagesComplications of OtoplastyLaineyNo ratings yet
- Surgical Options in Oroantral Fistula TreatmentDocument5 pagesSurgical Options in Oroantral Fistula TreatmentmartarayaniNo ratings yet
- Discovering Middle Ear Anatomy by Transcanal Endoscopic Ear Surgery: A Dissection ManualDocument8 pagesDiscovering Middle Ear Anatomy by Transcanal Endoscopic Ear Surgery: A Dissection ManualGuillermo Castro ContardoNo ratings yet
- Mastoidectomy and EpitympanectomyDocument18 pagesMastoidectomy and EpitympanectomyNodsiriNo ratings yet
- DownloadDocument12 pagesDownloadhasan nazzalNo ratings yet
- Endoscopic Septoplasty: Indications, Technique, and ResultsDocument5 pagesEndoscopic Septoplasty: Indications, Technique, and ResultsGabriel Vazquez RamosNo ratings yet
- Imaging of PediatricHearing LossDocument13 pagesImaging of PediatricHearing LossDianithus169No ratings yet
- Oroantral Communications. A Retrospective Analysis: Josué Hernando, Lorena Gallego, Luis Junquera, Pedro VillarrealDocument5 pagesOroantral Communications. A Retrospective Analysis: Josué Hernando, Lorena Gallego, Luis Junquera, Pedro VillarrealPla ParichartNo ratings yet
- 4 Oral Cavity ProceduresDocument10 pages4 Oral Cavity ProceduresAnne MarieNo ratings yet
- Full Article CWD MastoidectomyDocument5 pagesFull Article CWD MastoidectomyAbhishek Kumar RamadhinNo ratings yet
- The Translabyrinthine Approach: James Bowman, MBBS, BDSC, FracsDocument8 pagesThe Translabyrinthine Approach: James Bowman, MBBS, BDSC, FracsSebastianNo ratings yet
- Meningoencephalocele of The Temporal Bone-A Case Report: DR.B.V.N Muralidhar Reddy, DR K.V.V.RamjiDocument6 pagesMeningoencephalocele of The Temporal Bone-A Case Report: DR.B.V.N Muralidhar Reddy, DR K.V.V.RamjiNityaNo ratings yet
- 882 Frequency of Incus Bone Erosion On Mastoid Exploration in Chronic Suppurative Otitis Media With Middle Ear CholesteatomaDocument4 pages882 Frequency of Incus Bone Erosion On Mastoid Exploration in Chronic Suppurative Otitis Media With Middle Ear CholesteatomaRahul SahayNo ratings yet
- Cholesteatoma - Diagnosing The Unsafe EarDocument6 pagesCholesteatoma - Diagnosing The Unsafe EarGuillermo StipechNo ratings yet
- 5 Mastoidectomy and CholesteatomaDocument27 pages5 Mastoidectomy and CholesteatomaCondurache Ilie-AndreiNo ratings yet
- Relation Between Adenoid Size and Otitis Media With EffusionDocument4 pagesRelation Between Adenoid Size and Otitis Media With EffusionnadaNo ratings yet
- Nasopalatine Duct Cyst - A Delayed Complication To Successful Dental Implant Placement - Diagnosis and Surgical Management - As Published in The JOIDocument6 pagesNasopalatine Duct Cyst - A Delayed Complication To Successful Dental Implant Placement - Diagnosis and Surgical Management - As Published in The JOIHashem Motahir Ali Al-ShamiriNo ratings yet
- Incorporatingendoscopic Earsurgeryintoyour Clinicalpractice: Elliott D. Kozin,, Ruwan Kiringoda,, Daniel J. LeeDocument15 pagesIncorporatingendoscopic Earsurgeryintoyour Clinicalpractice: Elliott D. Kozin,, Ruwan Kiringoda,, Daniel J. LeeStanislaus Stanley SuhermanNo ratings yet
- 2000 J C. H S W A: Udson Ickey Cientific Riting WardDocument6 pages2000 J C. H S W A: Udson Ickey Cientific Riting WardPremshith CpNo ratings yet
- Condilectomia Intra OralDocument7 pagesCondilectomia Intra OralJuan Carlos MeloNo ratings yet
- 4.8 Ear Procedures and TreatmentsDocument2 pages4.8 Ear Procedures and Treatmentskwoke chizobaNo ratings yet
- Preauricular Sinus and Its ManagmentDocument12 pagesPreauricular Sinus and Its ManagmentDr. T. Balasubramanian100% (7)
- Oto EndosDocument3 pagesOto EndosMona BahrNo ratings yet
- Chapter 4 - Surgery For Choanal Atresia: Eugene N. MyersDocument4 pagesChapter 4 - Surgery For Choanal Atresia: Eugene N. MyersGloriaCorredorNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Applsci 11 11839 v2Document12 pagesApplsci 11 11839 v2Luis De jesus SolanoNo ratings yet
- Stapedotomy With Incus Vibroplasty - A Novel Surgical Solution of Advanced Otosclerosis and Its Place Among Existing Therapeutic Modalities - Hungarian Single Institutional ExperiencesDocument10 pagesStapedotomy With Incus Vibroplasty - A Novel Surgical Solution of Advanced Otosclerosis and Its Place Among Existing Therapeutic Modalities - Hungarian Single Institutional ExperiencesLuis De jesus SolanoNo ratings yet
- Signs and Symptoms of Obstructive Sleep Apnea and Upper Airway Resistance SyndromeDocument7 pagesSigns and Symptoms of Obstructive Sleep Apnea and Upper Airway Resistance SyndromeLuis De jesus SolanoNo ratings yet
- Drug-Induced Sleep Endoscopy (DISE)Document4 pagesDrug-Induced Sleep Endoscopy (DISE)Luis De jesus SolanoNo ratings yet
- Airway Evaluation in Obstructive Sleep ApneaDocument10 pagesAirway Evaluation in Obstructive Sleep ApneaLuis De jesus SolanoNo ratings yet
- Laryngeal Amyloidosis: ReviewDocument8 pagesLaryngeal Amyloidosis: ReviewLuis De jesus SolanoNo ratings yet
- Improving Decannulation Rates in Trauma Patients: Critical Care Medicine January 2019Document5 pagesImproving Decannulation Rates in Trauma Patients: Critical Care Medicine January 2019Luis De jesus SolanoNo ratings yet
- Icu-Related Dysphagia Epidemiology, Pathophysiology, Diagnostics and TreatmentDocument6 pagesIcu-Related Dysphagia Epidemiology, Pathophysiology, Diagnostics and TreatmentLuis De jesus SolanoNo ratings yet
- Optimal Time Delay Between Epinephrine Injection and Incision To Minimize BleedingDocument4 pagesOptimal Time Delay Between Epinephrine Injection and Incision To Minimize BleedingLuis De jesus SolanoNo ratings yet
- Revisiting The Relationship Between The Submandibular Duct, Lingual Nerve and Hypoglossal NerveDocument6 pagesRevisiting The Relationship Between The Submandibular Duct, Lingual Nerve and Hypoglossal NerveLuis De jesus SolanoNo ratings yet
- ENT UK Guidelines - Decontamination of Flexible and Rigid Endoscopes 2017Document14 pagesENT UK Guidelines - Decontamination of Flexible and Rigid Endoscopes 2017Luis De jesus SolanoNo ratings yet
- AnestheticsDocument2 pagesAnestheticsLuis De jesus SolanoNo ratings yet
- Professional Template For A 48x48 Case Report Poster PresentationDocument1 pageProfessional Template For A 48x48 Case Report Poster PresentationLuis De jesus SolanoNo ratings yet
- Septum de KornerDocument5 pagesSeptum de KornerLuis De jesus SolanoNo ratings yet
- Egyptian Journal of Ear, Nose, Throat and Allied SciencesDocument5 pagesEgyptian Journal of Ear, Nose, Throat and Allied SciencesLuis De jesus SolanoNo ratings yet
- Endoscopic Dacryocystorhinostomy - DCR - Surgical TechniqueDocument11 pagesEndoscopic Dacryocystorhinostomy - DCR - Surgical TechniqueLuis De jesus SolanoNo ratings yet
- Four Year Plan StandardDocument4 pagesFour Year Plan Standardapi-336266844No ratings yet
- Wheat Crop Development in Central Punjab (Faisalabad, 2020 - 21)Document32 pagesWheat Crop Development in Central Punjab (Faisalabad, 2020 - 21)Fuzail KhanNo ratings yet
- College of Pharmacy QA Unit: Dispensing of Medications: PHCL 701507-2: 5/ 9: 2Document19 pagesCollege of Pharmacy QA Unit: Dispensing of Medications: PHCL 701507-2: 5/ 9: 2hamam salih badriNo ratings yet
- Is Matter Around Us PureDocument25 pagesIs Matter Around Us PureGaurav MehndirattaNo ratings yet
- A Crazy Duck Cow My Dog and Cat Reading Comprehension For Grade 1Document4 pagesA Crazy Duck Cow My Dog and Cat Reading Comprehension For Grade 1Rika SuryaNo ratings yet
- DCL Report - Hygitech HSDocument2 pagesDCL Report - Hygitech HSFarhan RashidNo ratings yet
- Listing Down Classroom Rules: Observing Classroom Management RoutinesDocument5 pagesListing Down Classroom Rules: Observing Classroom Management RoutinesMariya QuedzNo ratings yet
- Indiana Contract With ID - MeDocument23 pagesIndiana Contract With ID - MeWTHR80% (5)
- Dialog AdmissionDocument3 pagesDialog AdmissionekaNo ratings yet
- Final Annual Report 2018Document31 pagesFinal Annual Report 2018Nirmal Kumar SharmaNo ratings yet
- English For ChemistryDocument53 pagesEnglish For ChemistryNoah FathiNo ratings yet
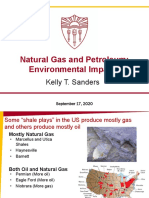
- FA2020 - ENE505 - L4.5 - Fossil Fuels - Oil & Gas Env ImpactsDocument43 pagesFA2020 - ENE505 - L4.5 - Fossil Fuels - Oil & Gas Env ImpactsTommy TrojanNo ratings yet
- Pregnancy and Birth in Denmark - April 2023Document4 pagesPregnancy and Birth in Denmark - April 2023valckefranNo ratings yet
- Multron AVD C500 Series Strobe and EA GD Pages 2 3Document2 pagesMultron AVD C500 Series Strobe and EA GD Pages 2 3tonnyNo ratings yet
- User Manuel - ESCODocument38 pagesUser Manuel - ESCOSerhat YıldırımNo ratings yet
- Actus ReusDocument7 pagesActus ReusSaffah Mohamed0% (1)
- Sugar Industry of PakistanDocument30 pagesSugar Industry of Pakistanadnaneconomist100% (9)
- 2011 NIPCC Interim ReportDocument432 pages2011 NIPCC Interim ReportMattParke100% (2)
- Kit SopDocument9 pagesKit SopSachin PrasadNo ratings yet
- Dereje Dairy Farm Project DraftDocument31 pagesDereje Dairy Farm Project DraftJemalNo ratings yet
- DISCIPLINESPECS - 20170810 - Standard Specifications For IT Network Configur.... PDF - DOC634349Document21 pagesDISCIPLINESPECS - 20170810 - Standard Specifications For IT Network Configur.... PDF - DOC634349Todd ENo ratings yet
- Ellipsoidal Dished EndsDocument28 pagesEllipsoidal Dished EndsRamakrishnan SrinivasanNo ratings yet
- Important Monthly Current Affairs Capsule - October 2022Document382 pagesImportant Monthly Current Affairs Capsule - October 2022FebzNo ratings yet
- History of Nestle: Nescafé Coffee Was LaunchedDocument5 pagesHistory of Nestle: Nescafé Coffee Was Launchednikhilgupta117No ratings yet
- DPSPS: The Advices of The ConstitutionDocument11 pagesDPSPS: The Advices of The ConstitutionNisha DixitNo ratings yet
- Financial Analysis of BioconDocument12 pagesFinancial Analysis of BioconNipun KothariNo ratings yet
- Wrought Cobalt - 28chromium - 6molybdenum Alloys For Surgical Implants (UNS R31537, UNS R31538, and UNS R31539)Document3 pagesWrought Cobalt - 28chromium - 6molybdenum Alloys For Surgical Implants (UNS R31537, UNS R31538, and UNS R31539)Gustavo SuarezNo ratings yet
- Drilling Mud CalculationDocument12 pagesDrilling Mud Calculationaditya imansyahNo ratings yet
- TriconexDocument38 pagesTriconexajmalahmed82No ratings yet
- Discover Biology The Core 6th Edition Singh Test BankDocument16 pagesDiscover Biology The Core 6th Edition Singh Test Bankkylebrownorjxwgecbq100% (16)