You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Association Between Chronic Pain and ObesityDocument10 pagesThe Association Between Chronic Pain and ObesityEnzoNo ratings yet
- Pagano2015Document9 pagesPagano2015EnzoNo ratings yet
- Golijanin2006Document8 pagesGolijanin2006EnzoNo ratings yet
- Nascimento2020Document7 pagesNascimento2020EnzoNo ratings yet
- Carneiro2020Document7 pagesCarneiro2020EnzoNo ratings yet
- Peripheral Neuropathies After Bariatric Surgery: A Current ReviewDocument6 pagesPeripheral Neuropathies After Bariatric Surgery: A Current ReviewEnzoNo ratings yet
- Alternative Treatment of Fibromyalgia Using The Oxytocin - Hormonal-Nutrient Protocol To Increase Nitric OxideDocument25 pagesAlternative Treatment of Fibromyalgia Using The Oxytocin - Hormonal-Nutrient Protocol To Increase Nitric OxideEnzoNo ratings yet
- 1.phosphodiesterase Type 5 in Men With Vasculogenic and Post-Radical Prostatectomy Erectile Dysfunction Is There A MolecularDocument9 pages1.phosphodiesterase Type 5 in Men With Vasculogenic and Post-Radical Prostatectomy Erectile Dysfunction Is There A MolecularEnzoNo ratings yet
- Postbariatric Surgery Neuropathic Pain (PBSNP) : Case Report, Literature Review, and Treatment OptionsDocument9 pagesPostbariatric Surgery Neuropathic Pain (PBSNP) : Case Report, Literature Review, and Treatment OptionsEnzoNo ratings yet
- Oral Allergy Syndrome - Pollens and Cross-Reacting FoodsDocument1 pageOral Allergy Syndrome - Pollens and Cross-Reacting FoodsEnzoNo ratings yet
- Peripheral Nerve Complications After Bariatric SurgeryDocument2 pagesPeripheral Nerve Complications After Bariatric SurgeryEnzoNo ratings yet
- Implications of Bariatric Surgery On Chronic Pain and Opioid UseDocument4 pagesImplications of Bariatric Surgery On Chronic Pain and Opioid UseEnzoNo ratings yet
- Evaluation of Low Back Pain in Patients Who Underwent Bariatric SurgeryDocument6 pagesEvaluation of Low Back Pain in Patients Who Underwent Bariatric SurgeryEnzoNo ratings yet
- Chronic Pain Disorder Medical Treatment GuidelinesDocument51 pagesChronic Pain Disorder Medical Treatment GuidelinesEnzoNo ratings yet
- Chronic Pain Disorder Medical Treatment GuidelinesDocument51 pagesChronic Pain Disorder Medical Treatment GuidelinesEnzoNo ratings yet
- Chronic Abdominal Pain and Persistent Opioid Use After Bariatric SurgeryDocument13 pagesChronic Abdominal Pain and Persistent Opioid Use After Bariatric SurgeryEnzoNo ratings yet
- Low Back Health through Stabilization ExercisesDocument8 pagesLow Back Health through Stabilization ExercisesDavid StadkindNo ratings yet
- The Physiologic Effects of Pain On The Endocrine SystemDocument12 pagesThe Physiologic Effects of Pain On The Endocrine SystemEnzoNo ratings yet
- Oral Allergy SyndromeDocument3 pagesOral Allergy SyndromeEnzoNo ratings yet
- The Role of Reactive Oxygen Species (ROS) in The Biological Activities of Metallic NanoparticlesDocument21 pagesThe Role of Reactive Oxygen Species (ROS) in The Biological Activities of Metallic NanoparticlesEnzoNo ratings yet
- Review ArticleDocument24 pagesReview ArticleEnzoNo ratings yet
- Mitochondrial Dynamics, ROS, and Cell Signaling: A Blended OverviewDocument20 pagesMitochondrial Dynamics, ROS, and Cell Signaling: A Blended OverviewEnzoNo ratings yet
- The Role of Cellular Reactive Oxygen Species in Cancer ChemotherapyDocument10 pagesThe Role of Cellular Reactive Oxygen Species in Cancer ChemotherapyEnzoNo ratings yet
- Molecular Pathways: Reactive Oxygen Species Homeostasis in Cancer Cells and Implications For Cancer TherapyDocument7 pagesMolecular Pathways: Reactive Oxygen Species Homeostasis in Cancer Cells and Implications For Cancer TherapyEnzoNo ratings yet
- Effects of Steroid Hormones On Sleep DisordersDocument4 pagesEffects of Steroid Hormones On Sleep DisordersEnzoNo ratings yet
- Lakesla ApoptosisDocument16 pagesLakesla ApoptosisNikkiNo ratings yet
- Testosterone Is Related To GABA+ Levels in The Posterior-Cingulate in Unmedicated Depressed Women During Reproductive LifeDocument7 pagesTestosterone Is Related To GABA+ Levels in The Posterior-Cingulate in Unmedicated Depressed Women During Reproductive LifeEnzoNo ratings yet
- Steroid Dysregulation and Stomatodynia (Burning Mouth Syndrome)Document9 pagesSteroid Dysregulation and Stomatodynia (Burning Mouth Syndrome)EnzoNo ratings yet
- Regulation of Inflammation Pathways and Inflammasome by Sex Steroid Hormones in EndometriosisDocument17 pagesRegulation of Inflammation Pathways and Inflammasome by Sex Steroid Hormones in EndometriosisEnzoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ulator REV2 USA EXAMPLEDocument35 pagesUlator REV2 USA EXAMPLEMilton UrrozNo ratings yet
- 2021 - СРРРРРРС - 3 Course - GM - EnglDocument17 pages2021 - СРРРРРРС - 3 Course - GM - EnglAiganym AmanovaNo ratings yet
- Concise Review: Importance of Probiotics Yogurt For Human Health ImprovementDocument6 pagesConcise Review: Importance of Probiotics Yogurt For Human Health ImprovementIOSRjournalNo ratings yet
- Saran prasarana kepatuhan pada anemia aplastikDocument1 pageSaran prasarana kepatuhan pada anemia aplastikAlika Nigandiva41No ratings yet
- Oppenheim J.J., Feldmann M. - Introduction To The Role of Cytokines in Innate Host Defense and Adaptive Immunity (2000) PDFDocument18 pagesOppenheim J.J., Feldmann M. - Introduction To The Role of Cytokines in Innate Host Defense and Adaptive Immunity (2000) PDFHesbon MomanyiNo ratings yet
- Patient Case PresentationDocument26 pagesPatient Case PresentationKathleen B BaldadoNo ratings yet
- What Is Peripheral Arterial Disease (PAD) ?: Blood VesselsDocument6 pagesWhat Is Peripheral Arterial Disease (PAD) ?: Blood VesselsmainehoonaNo ratings yet
- Powerpoint of Undifferentiated SchizophreniaDocument14 pagesPowerpoint of Undifferentiated SchizophreniaGian Carlo Soriente0% (1)
- Gonadal Hormones and Their Pharmacological InhibitorsDocument7 pagesGonadal Hormones and Their Pharmacological InhibitorsHydieNo ratings yet
- Index BurgerDocument8 pagesIndex BurgerWasim ChaudhryNo ratings yet
- Hervita - Depression and Anxiety Disorder Management in IndonesiaDocument30 pagesHervita - Depression and Anxiety Disorder Management in IndonesiaPrissilma TaniaNo ratings yet
- TMDDocument170 pagesTMDVinaya Srinivasan100% (2)
- Rajiv Gandhi University Dissertation Topics in NursingDocument7 pagesRajiv Gandhi University Dissertation Topics in NursingBuyPsychologyPapersTulsaNo ratings yet
- Materi Pencegahan PlabsiDocument51 pagesMateri Pencegahan PlabsiAnonymous HXyd4E100% (1)
- Nursing Care Plan Urinary Tract Infection (UTI)Document2 pagesNursing Care Plan Urinary Tract Infection (UTI)deric95% (97)
- Simulation in Health Care Education: Perspectives in Biology and Medicine February 2008Document6 pagesSimulation in Health Care Education: Perspectives in Biology and Medicine February 2008Birendra MahatNo ratings yet
- 5 1 1113Document7 pages5 1 1113Adhitya Rizky IsnandyaNo ratings yet
- The Future of Gene EditingDocument23 pagesThe Future of Gene EditingAnurag KunwarNo ratings yet
- Anatomy Pathophysiology PreeclampsiaDocument4 pagesAnatomy Pathophysiology PreeclampsiaKeith Wesley YbutNo ratings yet
- Pelvic Inflammatory Disease: Dr. Indah Meyliza, M. KesDocument13 pagesPelvic Inflammatory Disease: Dr. Indah Meyliza, M. KesIndah MeylizaNo ratings yet
- Group 3 Cardiovascular ProblemDocument52 pagesGroup 3 Cardiovascular ProblemWARREN WILLIAM PERAN100% (3)
- Lung Abscess Bronchoectasis PleurisynDocument19 pagesLung Abscess Bronchoectasis Pleurisynmarco luenaNo ratings yet
- Care of The Older Adult Handouts PrelimsDocument7 pagesCare of The Older Adult Handouts PrelimsAmanda Joy TuizaNo ratings yet
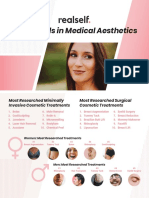
- RealSelf YearInReview OneSheetDocument2 pagesRealSelf YearInReview OneSheetDominico Adityo RaharjoNo ratings yet
- Ecg/EkgDocument29 pagesEcg/EkgbajaocNo ratings yet
- Basic Life SupportDocument8 pagesBasic Life SupportAdilla RachmawatiNo ratings yet
- Pediatric Nursing Course OutlineDocument6 pagesPediatric Nursing Course OutlineDaryl Adrian RecaidoNo ratings yet
- Emergency Assistance PlanDocument4 pagesEmergency Assistance PlanTerence100% (1)
- Immunization Verification Form 2018Document2 pagesImmunization Verification Form 2018Jawad JamilNo ratings yet
- Three Treasures Correspondences BrochureDocument4 pagesThree Treasures Correspondences Brochure292293709No ratings yet