You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Comparison of The Ferno Scoop Stretcher With The Long Backboard For Spinal ImmobilizationDocument7 pagesComparison of The Ferno Scoop Stretcher With The Long Backboard For Spinal ImmobilizationLeandro NogueiraNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Current Thinking Cervical Collar Use in SMR May 2019Document5 pagesCurrent Thinking Cervical Collar Use in SMR May 2019Leandro NogueiraNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Schroeder 2018Document10 pagesSchroeder 2018Leandro NogueiraNo ratings yet
- Olaus Sen 2017Document7 pagesOlaus Sen 2017Leandro NogueiraNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Self-Extrication and Selective Spinal Immobilisation in A Polytrauma Patient With Spinal InjuriesDocument4 pagesSelf-Extrication and Selective Spinal Immobilisation in A Polytrauma Patient With Spinal InjuriesLeandro NogueiraNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 10 1016@j Amj 2020 07 009Document6 pages10 1016@j Amj 2020 07 009Leandro NogueiraNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Injury Patterns and Causes of Death in 953 Patients With Penetrating Abdominal War Wounds in A Civilian Independent Non-Governmental Organization Hospital in Lashkargah, AfghanistanDocument8 pagesInjury Patterns and Causes of Death in 953 Patients With Penetrating Abdominal War Wounds in A Civilian Independent Non-Governmental Organization Hospital in Lashkargah, AfghanistanLeandro NogueiraNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Jones 2014Document8 pagesJones 2014Leandro NogueiraNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
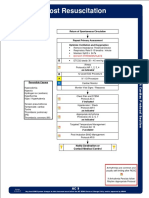
- AC 9 Post Resuscitation Protocol Final 2017 EditableDocument2 pagesAC 9 Post Resuscitation Protocol Final 2017 EditableLeandro NogueiraNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Ventilator Management of Adult Patients in The Emergency DepartmentDocument20 pagesVentilator Management of Adult Patients in The Emergency DepartmentLeandro NogueiraNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- START Versus SALT Triage: Which Is Preferred by The 21 Century Health Care Student?Document6 pagesSTART Versus SALT Triage: Which Is Preferred by The 21 Century Health Care Student?Leandro NogueiraNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Monro-Kellie 2.0: The Dynamic Vascular and Venous Pathophysiological Components of Intracranial PressureDocument13 pagesMonro-Kellie 2.0: The Dynamic Vascular and Venous Pathophysiological Components of Intracranial PressureLeandro NogueiraNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- E230 FullDocument10 pagesE230 FullLeandro NogueiraNo ratings yet
- JLG ANSI & CSA Standards Readiness GuideDocument8 pagesJLG ANSI & CSA Standards Readiness GuideAlfredo VSNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Favour Emmanuel - Resume - Data AnalystDocument3 pagesFavour Emmanuel - Resume - Data AnalystEmmanuel FavourNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Latest GPS Tracker Quotation From PST Mary (2012!07!23)Document2 pagesLatest GPS Tracker Quotation From PST Mary (2012!07!23)Hitendra Nath BarmmaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Impact of Thermal Aging On The Intermetallic Compound Particle Size andDocument9 pagesImpact of Thermal Aging On The Intermetallic Compound Particle Size andAamir JanNo ratings yet
- Us Navy Flight Test ManualDocument881 pagesUs Navy Flight Test ManualDavid Russo100% (8)
- Analisis GC MS Fusel OilDocument23 pagesAnalisis GC MS Fusel OilKarenLissNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Lab Heat Experment 2Document5 pagesLab Heat Experment 2حسين عمريNo ratings yet
- Mindfulness in Primary School Children ADocument15 pagesMindfulness in Primary School Children AMuhammad Irfan AneesNo ratings yet
- Impact TestDocument11 pagesImpact TestMohsin AbbasNo ratings yet
- Product Drawing: MillenniumDocument13 pagesProduct Drawing: Millenniumjuan991No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Chapter 16 - Nur-WPS OfficeDocument11 pagesChapter 16 - Nur-WPS Officemichelle marquezNo ratings yet
- 2016 MVP Tcode Key GuideDocument149 pages2016 MVP Tcode Key GuideEnrique GomezNo ratings yet
- 7QC ToolsDocument62 pages7QC ToolsRaiham EffendyNo ratings yet
- M MMMMMMMMMMDocument3 pagesM MMMMMMMMMMDavid R Paucara0% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Hartnell Governor Isochronous Speed Equations - Engineers EdgeDocument1 pageHartnell Governor Isochronous Speed Equations - Engineers Edgestallone21No ratings yet
- Coop Conference Proceeding (21-22aug 2022)Document585 pagesCoop Conference Proceeding (21-22aug 2022)oliviahuda75No ratings yet
- Consumer Markets andDocument35 pagesConsumer Markets andanon_159262080100% (1)
- Predictive Influence of Domestic Violence, Socioeconomic Status, Educational Level and Gender On The Martial Stability of CouplesDocument18 pagesPredictive Influence of Domestic Violence, Socioeconomic Status, Educational Level and Gender On The Martial Stability of CouplesayoNo ratings yet
- Morphology and Culture - MoldsDocument8 pagesMorphology and Culture - Moldslisa.angle204No ratings yet
- Fib Congress Freyssinet by ShushkewichDocument28 pagesFib Congress Freyssinet by ShushkewichpablokrahlNo ratings yet
- Array in Java (F)Document4 pagesArray in Java (F)Brajesh RajawatNo ratings yet
- Eurocode 7 Section 7 Pile FoundationsDocument20 pagesEurocode 7 Section 7 Pile FoundationsHoNo ratings yet
- 03 - Leviticus PDFDocument162 pages03 - Leviticus PDFGuZsolNo ratings yet
- Palmistry ExpertiseDocument65 pagesPalmistry ExpertisePawan AgrawalNo ratings yet
- List of Documents ISO 45001 Documentation Toolkit enDocument2 pagesList of Documents ISO 45001 Documentation Toolkit enCiciaSalatin100% (1)
- D375A-6 Cooling SystemDocument26 pagesD375A-6 Cooling Systemalcowo100% (3)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Vikash Babu Fundamentals of Gas Dynamic-45-62Document18 pagesVikash Babu Fundamentals of Gas Dynamic-45-62عمر ربيع المحلاوىNo ratings yet
- Bible - To Love, Honor and Vacuum PDFDocument9 pagesBible - To Love, Honor and Vacuum PDFDiana ArunNo ratings yet
- Modern Pentecostal Controversies (Fuiten)Document101 pagesModern Pentecostal Controversies (Fuiten)bratrekimNo ratings yet
- Technical Requirements For Medical DevicesDocument11 pagesTechnical Requirements For Medical DeviceshelloNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)