You might also like
- HSNS362Document16 pagesHSNS362mandyNo ratings yet
- PrognosisDocument7 pagesPrognosispenyimpanankoas8No ratings yet
- Lactobacillus Acidophilus and Bifidobacterium Bifidum Atored at Ambient Temperature Are Effective in The Treatment of Acute DiarrhoeaDocument7 pagesLactobacillus Acidophilus and Bifidobacterium Bifidum Atored at Ambient Temperature Are Effective in The Treatment of Acute DiarrhoeaEvelynRuizNo ratings yet
- Lactobacillus Therapy For Acute Infectious Diarrhea in Children A Meta-AnalysisDocument9 pagesLactobacillus Therapy For Acute Infectious Diarrhea in Children A Meta-AnalysisfahrunisaNo ratings yet
- Art:10.1007/s00431 007 0419 XDocument8 pagesArt:10.1007/s00431 007 0419 XDini NanamiNo ratings yet
- Homeopathic Treatment of Acute Childhood Diarrhea: Results From A Clinical Trial in NepalDocument10 pagesHomeopathic Treatment of Acute Childhood Diarrhea: Results From A Clinical Trial in NepalKiran DalabanjanNo ratings yet
- 388Document6 pages388anhiramdhaniNo ratings yet
- Children in The Tropics: Lactobacillus GG and Acute Diarrhoea in YoungDocument4 pagesChildren in The Tropics: Lactobacillus GG and Acute Diarrhoea in YoungRaluca ElenaNo ratings yet
- Diarrhea in Preschool Children and Lactobacillus 2017Document9 pagesDiarrhea in Preschool Children and Lactobacillus 2017Karindha Handayani HelisusantoNo ratings yet
- Efficacy of Probiotics in Acute Diarrhoea in Children: Original Research ArticleDocument5 pagesEfficacy of Probiotics in Acute Diarrhoea in Children: Original Research ArticledwimellyndaNo ratings yet
- A Randomized Controlled Trial of Probiotics For Clostridium Dif Cile Infection in AdultsDocument4 pagesA Randomized Controlled Trial of Probiotics For Clostridium Dif Cile Infection in Adults林新中No ratings yet
- FTP PDFDocument2 pagesFTP PDFMannu palNo ratings yet
- Peptic Ulcer Research Paper PDFDocument8 pagesPeptic Ulcer Research Paper PDFscxofyplg100% (1)
- Relationship Between Helicobacter PyloriDocument9 pagesRelationship Between Helicobacter PyloriTamirat BelaynaNo ratings yet
- Bacillus Clausii As An Adjuvant Therapy in Acute Childhood DiarrhoeaDocument3 pagesBacillus Clausii As An Adjuvant Therapy in Acute Childhood DiarrhoeaIOSRjournalNo ratings yet
- Are Probiotics Money Down The Toilet? or Worse?: January 30, 2019Document5 pagesAre Probiotics Money Down The Toilet? or Worse?: January 30, 2019Horhe NairbNo ratings yet
- Total Nutritional Therapy: A Nutrition Education Program For PhysiciansDocument7 pagesTotal Nutritional Therapy: A Nutrition Education Program For PhysiciansTia WasrilNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyMuhammad AsrizalNo ratings yet
- Gelatine Tannate in The Management of Acute GastroenteritisDocument39 pagesGelatine Tannate in The Management of Acute Gastroenteritiszaky ariandyNo ratings yet
- 5 FullDocument7 pages5 FullBeatrice KoesmarsonoNo ratings yet
- Psyllium Fiber Reduces Abdominal Pain in Children With IbsDocument12 pagesPsyllium Fiber Reduces Abdominal Pain in Children With IbsEmilia JonatanNo ratings yet
- Prática Antibiótico AlhoDocument6 pagesPrática Antibiótico Alhoapi-3736634No ratings yet
- Full Text Jurnal LactobasilusDocument10 pagesFull Text Jurnal Lactobasilusrisda aulia putriNo ratings yet
- GasiDocument36 pagesGasiAdy Fitra Saragih100% (1)
- Prescript-Assist Probiotic-Prebiotic Treatment For Bacterial Diarrhea - Clinical Experience in Ecuador (8 PP)Document8 pagesPrescript-Assist Probiotic-Prebiotic Treatment For Bacterial Diarrhea - Clinical Experience in Ecuador (8 PP)Xavier SauconyNo ratings yet
- Lactobacillus Rhamnosus GG Versus Placebo For Acute Gastroenteritis in ChildrenDocument21 pagesLactobacillus Rhamnosus GG Versus Placebo For Acute Gastroenteritis in ChildrenMarsella Epifania SuwignyoNo ratings yet
- Case Studies DetailsDocument36 pagesCase Studies Detailssiachen26100% (1)
- Scholar Blueberry and CognitionDocument12 pagesScholar Blueberry and CognitionCéline Van wolputteNo ratings yet
- Diarr 20Document4 pagesDiarr 20Pablo Pinaya SotomayorNo ratings yet
- Rebamipide, A Gastro-Protective and Anti-Inflammatory Drug, Promotes Gastric Ulcer Healing Following Eradication TherapyDocument4 pagesRebamipide, A Gastro-Protective and Anti-Inflammatory Drug, Promotes Gastric Ulcer Healing Following Eradication TherapySilvester HenryNo ratings yet
- Dyspepsia Journal PediatricDocument11 pagesDyspepsia Journal PediatricFatt ZakiNo ratings yet
- TELAAH JURNAL INTERNASIONAL - Antik KritiyaniDocument12 pagesTELAAH JURNAL INTERNASIONAL - Antik Kritiyaniandrea viqiNo ratings yet
- Anaemia+in+pregnancy 27042016Document5 pagesAnaemia+in+pregnancy 27042016Alma AwaliyahNo ratings yet
- Pengaruh Pemberian Heat-Killed Probiotic Complex Pada Usia 6 - 24 Bulan Terhadap Perjalanan Dan Kesembuhan Diare AkutDocument3 pagesPengaruh Pemberian Heat-Killed Probiotic Complex Pada Usia 6 - 24 Bulan Terhadap Perjalanan Dan Kesembuhan Diare AkutDonnie DityaNo ratings yet
- Curs3 12Document15 pagesCurs3 12Monica AdamNo ratings yet
- Three-Combination Probiotics Therapy in Children With Salmonella and Rotavirus GastroenteritisDocument6 pagesThree-Combination Probiotics Therapy in Children With Salmonella and Rotavirus Gastroenteritisnadin nNo ratings yet
- Ncologist: S M S CDocument4 pagesNcologist: S M S CFardani MaknunNo ratings yet
- Kelompok BDocument6 pagesKelompok Bcheese schedarNo ratings yet
- Feeding The Open Abdomen: Journal of Parenteral and Enteral Nutrition September 2007Document7 pagesFeeding The Open Abdomen: Journal of Parenteral and Enteral Nutrition September 2007Risda AlwaritsiNo ratings yet
- Multicenter Trial of A Combination Probiotic For Children With GastroenteritisDocument12 pagesMulticenter Trial of A Combination Probiotic For Children With GastroenteritisCTV CalgaryNo ratings yet
- Study Consipation Howaru-TransitDocument8 pagesStudy Consipation Howaru-TransitMộc MộcNo ratings yet
- Article 2 - OPEN Study - Subar AM - Am J Epid 2003Document13 pagesArticle 2 - OPEN Study - Subar AM - Am J Epid 2003Prajna AdityaraniNo ratings yet
- A Therapeutic Maneuver For Oropharyngeal Dysphagia in Patients With PDDocument6 pagesA Therapeutic Maneuver For Oropharyngeal Dysphagia in Patients With PDmajid mirzaeeNo ratings yet
- Reading Journal ALYADocument14 pagesReading Journal ALYAAlya AnnisaNo ratings yet
- Probiotics in The Treatment of Acute Diarrhea in Young ChildrenDocument4 pagesProbiotics in The Treatment of Acute Diarrhea in Young ChildrenJaTi NurwigatiNo ratings yet
- Multicentre, Cluster-Randomized Clinical Trial of Algorithms For Critical-Care Enteral and Parenteral Therapy (ACCEPT)Document8 pagesMulticentre, Cluster-Randomized Clinical Trial of Algorithms For Critical-Care Enteral and Parenteral Therapy (ACCEPT)eryxspNo ratings yet
- Instructor Gastroenteritis TexasDocument20 pagesInstructor Gastroenteritis TexasJulio VeraNo ratings yet
- 28 - MatthewDocument6 pages28 - MatthewRosa PerezNo ratings yet
- Pediatrics 2014 Queen E23 9Document10 pagesPediatrics 2014 Queen E23 9Desrainy InhardiniNo ratings yet
- ProbiotikDocument6 pagesProbiotikEssaLoyalLitaLestariNo ratings yet
- DiareDocument10 pagesDiareNanda Putri SeptianaNo ratings yet
- Artikel 2 DheaDocument16 pagesArtikel 2 Dheadayana nopridaNo ratings yet
- Jurnal 2 AnakDocument5 pagesJurnal 2 AnakHafich ErnandaNo ratings yet
- Rebecca JacklDocument5 pagesRebecca Jacklmija2No ratings yet
- Early Total Enteral Feeding in Stable Very Low Birth Weight Infants: A Before and After StudyDocument7 pagesEarly Total Enteral Feeding in Stable Very Low Birth Weight Infants: A Before and After StudySupriya M A SuppiNo ratings yet
- Afifi Et Al, 2017. Dietary Behaviors in Psoriasis Patient-Reported PDFDocument16 pagesAfifi Et Al, 2017. Dietary Behaviors in Psoriasis Patient-Reported PDFPaola StarioloNo ratings yet
- Nutritional Therapy For Infants With Diarrhea Lif Schitz 1990Document10 pagesNutritional Therapy For Infants With Diarrhea Lif Schitz 1990Kristina Joy HerlambangNo ratings yet
- Efficacy of A New Hypotonic Oral Rehydration Solution Containing Zinc and Prebiotics in The Treatment of Childhood Acute Diarrhea: A Randomized Controlled TrialDocument6 pagesEfficacy of A New Hypotonic Oral Rehydration Solution Containing Zinc and Prebiotics in The Treatment of Childhood Acute Diarrhea: A Randomized Controlled TrialOlpinNo ratings yet
- Module 6 - Case Study Exercise Gastroenteritis at A College: Learning ObjectivesDocument9 pagesModule 6 - Case Study Exercise Gastroenteritis at A College: Learning ObjectivesdlsajdlkasNo ratings yet
- The EffectDocument4 pagesThe EffectDahlia WahyuningsihNo ratings yet
- The Changing Landscape of IBD: Emerging Concepts in Patient ManagementFrom EverandThe Changing Landscape of IBD: Emerging Concepts in Patient ManagementNo ratings yet
- Nausea, Vomiting, and DiarrheaDocument2 pagesNausea, Vomiting, and DiarrheaShanaka KasthuriarachchiNo ratings yet
- 21st Century Approaches To Addressing Childhood Diarrhea in Low ADocument121 pages21st Century Approaches To Addressing Childhood Diarrhea in Low AShanaka KasthuriarachchiNo ratings yet
- Crofelemerreview Cottreau Exp Rev 2012Document8 pagesCrofelemerreview Cottreau Exp Rev 2012Shanaka KasthuriarachchiNo ratings yet
- 2016 Acute DiarrheaDocument21 pages2016 Acute DiarrheaVenny HilleryNo ratings yet
- Guidelines For Treatment of Acute Infectious Diarrhea in AdultsDocument9 pagesGuidelines For Treatment of Acute Infectious Diarrhea in AdultsShanaka KasthuriarachchiNo ratings yet
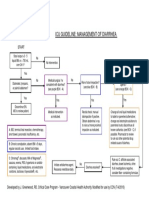
- Icu Guideline: Management of Diarrhea: StartDocument1 pageIcu Guideline: Management of Diarrhea: StartShanaka KasthuriarachchiNo ratings yet
- Guidelines For Treatment of Acute Infectious Diarrhea in AdultsDocument9 pagesGuidelines For Treatment of Acute Infectious Diarrhea in AdultsShanaka KasthuriarachchiNo ratings yet
- Diarrhea NotesDocument8 pagesDiarrhea Notesgodeberta18No ratings yet
- 21st Century Approaches To Addressing Childhood Diarrhea in Low ADocument121 pages21st Century Approaches To Addressing Childhood Diarrhea in Low AShanaka KasthuriarachchiNo ratings yet
- Preventionof DiarrheaDocument16 pagesPreventionof DiarrheaShanaka KasthuriarachchiNo ratings yet
- Approach To The Patient With Chronic Diarrhea: Eric M. Osgard MD FACG Gastroenterology Consultants Reno, NVDocument36 pagesApproach To The Patient With Chronic Diarrhea: Eric M. Osgard MD FACG Gastroenterology Consultants Reno, NVShanaka KasthuriarachchiNo ratings yet
- Globaldiarrhea508c PDFDocument4 pagesGlobaldiarrhea508c PDFRindaNo ratings yet
- Diarrheal DiseasesDocument123 pagesDiarrheal DiseasesShanaka KasthuriarachchiNo ratings yet
- Acute Diarrhoeal DiseasesDocument47 pagesAcute Diarrhoeal DiseasesKumara GuruNo ratings yet
- Acute Diarrhoeal DiseasesDocument47 pagesAcute Diarrhoeal DiseasesKumara GuruNo ratings yet
- Approach To The Patient With Chronic Diarrhea: Eric M. Osgard MD FACG Gastroenterology Consultants Reno, NVDocument36 pagesApproach To The Patient With Chronic Diarrhea: Eric M. Osgard MD FACG Gastroenterology Consultants Reno, NVShanaka KasthuriarachchiNo ratings yet
- Diarrhea 508Document8 pagesDiarrhea 508Xie Xin XinNo ratings yet
- 2019 Theoretical & Applied Science 09-4 PDFDocument105 pages2019 Theoretical & Applied Science 09-4 PDFirina ugrekhelidzeNo ratings yet
- Resolution AgeismDocument7 pagesResolution AgeismRoseAnn DivinaNo ratings yet
- Communicative English 2 (Due30022) Lecturer'S Name: Mr. Mohamad Sobri Bin SuhailiDocument5 pagesCommunicative English 2 (Due30022) Lecturer'S Name: Mr. Mohamad Sobri Bin SuhailiWang Ja RimNo ratings yet
- Skolastik - Literasi Bahasa Inggris - Predicting The Paragraph (SOAL)Document5 pagesSkolastik - Literasi Bahasa Inggris - Predicting The Paragraph (SOAL)annisa auliaNo ratings yet
- Preboards 2 - NP3 (Printable)Document10 pagesPreboards 2 - NP3 (Printable)Joana Marie DomingoNo ratings yet
- Recalls (Legmed)Document8 pagesRecalls (Legmed)Jam PanumpangNo ratings yet
- Articulo 4Document6 pagesArticulo 4Eduardo GarcíaNo ratings yet
- Comparison of Chest X-Ray Findings Between Primary and Secondary Multidrug Resistant Pulmonary TuberculosisDocument8 pagesComparison of Chest X-Ray Findings Between Primary and Secondary Multidrug Resistant Pulmonary TuberculosismahyaNo ratings yet
- Para MCQDocument2 pagesPara MCQMohamed HaridyNo ratings yet
- Charney1998parte1 PDFDocument11 pagesCharney1998parte1 PDFmarielaNo ratings yet
- English For Nurse 5: 5. Reading Unit A. MR Jansen Has Had A Myocardial InfarctionDocument4 pagesEnglish For Nurse 5: 5. Reading Unit A. MR Jansen Has Had A Myocardial InfarctiondnnssnNo ratings yet
- Act Assessment Practice Reading PassageDocument3 pagesAct Assessment Practice Reading PassageThanh HàNo ratings yet
- A Good Time To Dance A Mixed-Methods Approach of The Effects of Dance Movement Therapy For Breast Cancer Patients During and After RadiotherapyDocument10 pagesA Good Time To Dance A Mixed-Methods Approach of The Effects of Dance Movement Therapy For Breast Cancer Patients During and After RadiotherapysetautoNo ratings yet
- Millet Grains: Nutritional Quality, Processing, and Potential Health BenefitsDocument16 pagesMillet Grains: Nutritional Quality, Processing, and Potential Health BenefitsBala NairNo ratings yet
- Kidde - 3M - Novec - 1230 - Safety - Data - Sheet - 05312019Document9 pagesKidde - 3M - Novec - 1230 - Safety - Data - Sheet - 05312019Victor ChuaNo ratings yet
- Dysphagia and Swallowing Disorders, MC Carty E. (2021)Document16 pagesDysphagia and Swallowing Disorders, MC Carty E. (2021)Irving Santiago SandovalNo ratings yet
- GEO129 Chapter 1Document6 pagesGEO129 Chapter 1suhardin laodeNo ratings yet
- What Are The Classification of HospitalsDocument11 pagesWhat Are The Classification of HospitalsLily Jane PakiwonNo ratings yet
- Article 1619692941Document6 pagesArticle 1619692941Pooja MehtaNo ratings yet
- Disseminated Intravascular Coagulation Is A Condition in Which Small Blood Clots DevelopDocument4 pagesDisseminated Intravascular Coagulation Is A Condition in Which Small Blood Clots DevelopRiaz JiwaNo ratings yet
- Quiz No.1Document5 pagesQuiz No.1Charina AubreyNo ratings yet
- Epidemiology - AMBOSSDocument13 pagesEpidemiology - AMBOSSFlowerNo ratings yet
- Tugas Laporan Literasi Bahasa Inggris Phobia? No Way!': Jasmine Syifa Hermawan Xi Ips 1Document6 pagesTugas Laporan Literasi Bahasa Inggris Phobia? No Way!': Jasmine Syifa Hermawan Xi Ips 1JasmineNo ratings yet
- CAPC Key Messages Re - COVID-19-Center To Advance Palliative Care PDFDocument1 pageCAPC Key Messages Re - COVID-19-Center To Advance Palliative Care PDFSergio Rafael Medina VillelaNo ratings yet
- Mycotoxins in Feed Ingredients PDFDocument8 pagesMycotoxins in Feed Ingredients PDFUmar ChaudharyNo ratings yet
- Advocacy Project 2 FinalDocument5 pagesAdvocacy Project 2 Finalapi-742583747No ratings yet
- Week 6 - Antiparkinsonism AgentsDocument18 pagesWeek 6 - Antiparkinsonism AgentsDino MicaNo ratings yet
- Occupational Therapy Interventions To Improve PDFDocument9 pagesOccupational Therapy Interventions To Improve PDFPaula FariaNo ratings yet
- Practices in Paediatric Gastrointestinal Endoscopy at Kenyatta National Hospital and Gertrudes Children's Hospital in Nairobi KenyaDocument11 pagesPractices in Paediatric Gastrointestinal Endoscopy at Kenyatta National Hospital and Gertrudes Children's Hospital in Nairobi Kenyafrankline nyabutoNo ratings yet