You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Comparing CP Surveillance DefinitionDocument2 pagesComparing CP Surveillance DefinitionЯковлев АлександрNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Children With IntellectualDocument8 pagesChildren With IntellectualЯковлев АлександрNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Classification of Topographical PatternDocument7 pagesClassification of Topographical PatternЯковлев АлександрNo ratings yet
- Changing Views of Cerebral Palsy Over 35 YearsDocument8 pagesChanging Views of Cerebral Palsy Over 35 YearsЯковлев АлександрNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Cerebral Palsy BirthsDocument7 pagesCerebral Palsy BirthsЯковлев АлександрNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Changing Pattern of CP in The Southwest Region of FinlandDocument7 pagesChanging Pattern of CP in The Southwest Region of FinlandЯковлев АлександрNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Cerebral Palsy in NorwayDocument10 pagesCerebral Palsy in NorwayЯковлев АлександрNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Approach To Neonate With Low Birth WeightDocument40 pagesApproach To Neonate With Low Birth Weightnirajan khanalNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Doh Health Programs MaternalDocument82 pagesDoh Health Programs MaternalWilma Nierva BeraldeNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Why Love Turns Into Hate PDFDocument2 pagesWhy Love Turns Into Hate PDFindrani royNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Hyper Bilirubin Emi ADocument33 pagesHyper Bilirubin Emi AMateen ShukriNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- DEVPSY Module 4 InfancyDocument22 pagesDEVPSY Module 4 InfancyARCHIE MEDES BARTENo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Ten Steps To Successful Breastfeeding Policy ReviewDocument14 pagesTen Steps To Successful Breastfeeding Policy ReviewAndini PramonoNo ratings yet
- c1 Mother Friendly Care NewDocument20 pagesc1 Mother Friendly Care NewOng Teck Chong100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Physical Assessment of The Newborn: Julniar M Tasli Herman BermawiDocument39 pagesPhysical Assessment of The Newborn: Julniar M Tasli Herman BermawiiqiqiqiqiqNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Child Health Nursing 3year BSCN 23082012 1429Document21 pagesChild Health Nursing 3year BSCN 23082012 1429renjiniNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Kamus Bahasa Inggris KebidananDocument24 pagesKamus Bahasa Inggris KebidananKhofifah Indrianii100% (2)
- Clinical Presentation On Child With Neonatal SepsisDocument37 pagesClinical Presentation On Child With Neonatal SepsisSREEDEVI T SURESHNo ratings yet
- Hope Starts Here Detroit Full Framework 2017Document92 pagesHope Starts Here Detroit Full Framework 2017Beverly TranNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pink, Blue, and Gender: An UpdateDocument9 pagesPink, Blue, and Gender: An UpdateAnonymous RzKglABIkUNo ratings yet
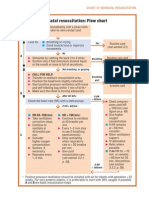
- Neonatal Resuscitation Program Flow ChartDocument3 pagesNeonatal Resuscitation Program Flow ChartChin Nam80% (5)
- College of DuPage Associate Degree Nursing Program Course Syllabus FallDocument64 pagesCollege of DuPage Associate Degree Nursing Program Course Syllabus FallThomas GrossNo ratings yet
- Umbilical Cord CareDocument6 pagesUmbilical Cord CareCarolin AgianNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- ESPGHAN Feeding The Late and Moderately Preterm InfantDocument12 pagesESPGHAN Feeding The Late and Moderately Preterm Infantkevin hernandezNo ratings yet
- Meal Planning for Infants and PreschoolersDocument21 pagesMeal Planning for Infants and PreschoolersHema MekalaNo ratings yet
- Breastfeeding A Guide For The Medical Profession Ruth A Lawrence Full ChapterDocument67 pagesBreastfeeding A Guide For The Medical Profession Ruth A Lawrence Full Chapterjulia.swanson282100% (5)
- Community Health Nursing Examination Part IDocument9 pagesCommunity Health Nursing Examination Part ITina Poquiz100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Ghana Essential Health Interventions Program: A Plausibility Trial of The Impact of Health Systems Strengthening On Maternal & Child SurvivalDocument12 pagesThe Ghana Essential Health Interventions Program: A Plausibility Trial of The Impact of Health Systems Strengthening On Maternal & Child SurvivalTizoon FaeyzaNo ratings yet
- Seminar On: Organisation and Management of Neonatal Services and NicuDocument27 pagesSeminar On: Organisation and Management of Neonatal Services and NicuDimple SweetbabyNo ratings yet
- Fleur McDonald - Crimson Dawn (Extract)Document32 pagesFleur McDonald - Crimson Dawn (Extract)Allen & UnwinNo ratings yet
- Pediatrics History and Physical ExamDocument16 pagesPediatrics History and Physical ExamstarrnewmanpaNo ratings yet
- Precipitous Labor/Delivery or Unplanned/Out-of-Hospital DeliveryDocument7 pagesPrecipitous Labor/Delivery or Unplanned/Out-of-Hospital DeliveryLei Ortega100% (1)
- Lectura 3 Obligatoria. Beebe y Lachmann (1994) - Tres Principios de SalienciaDocument37 pagesLectura 3 Obligatoria. Beebe y Lachmann (1994) - Tres Principios de SalienciaEbonnie DiazNo ratings yet
- Magic of TouchDocument28 pagesMagic of TouchkurniawatiNo ratings yet
- Bfhi Implementation 2018 AppendixDocument7 pagesBfhi Implementation 2018 AppendixssNo ratings yet
- Multimodality in Infancy Vocal-Motor and Speech-GeDocument14 pagesMultimodality in Infancy Vocal-Motor and Speech-GeTamiris AlvesNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)