You might also like
- GERDDocument47 pagesGERDSutanto TanakaNo ratings yet
- GERDDocument15 pagesGERDAhmed EzzatNo ratings yet
- A6. Tukak PeptikDocument31 pagesA6. Tukak PeptikSartika NapitupuluNo ratings yet
- GI Guideline 1 - GERDDocument17 pagesGI Guideline 1 - GERDAnggie PratiwiNo ratings yet
- Gerd - Peptic Ulcer - GastritisDocument87 pagesGerd - Peptic Ulcer - GastritisErickson V. LibutNo ratings yet
- Konsensus GerdDocument44 pagesKonsensus GerdPink Pinky cimutNo ratings yet
- GERDDocument35 pagesGERDRoyster Cabral100% (1)
- Gastroenterology Division Internal Medicine Department FK-USU/Adam Malik HospitalDocument78 pagesGastroenterology Division Internal Medicine Department FK-USU/Adam Malik HospitalcarinasheliapNo ratings yet
- Gastroesophageal Reflux Disease (GERD) Diagnosis and TreatmentDocument43 pagesGastroesophageal Reflux Disease (GERD) Diagnosis and TreatmentRoselin Megasari MendrofaNo ratings yet
- Pediatric GERDDocument51 pagesPediatric GERDPatNo ratings yet
- Gerd DDRCDocument74 pagesGerd DDRCBoris Ariel Hernandez BrionesNo ratings yet
- GerdDocument69 pagesGerdopkhfdegNo ratings yet
- Prescription Practice II - PHAR 422.00 Peptic Ulcer Disease C. Voke Abobo ProfessorDocument34 pagesPrescription Practice II - PHAR 422.00 Peptic Ulcer Disease C. Voke Abobo Professorfasty1No ratings yet
- GERDDocument2 pagesGERDRee AhmedNo ratings yet
- GERD Pariet OkDocument53 pagesGERD Pariet OkSheila Regina TizaNo ratings yet
- Case-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Document53 pagesCase-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Ditia RahimNo ratings yet
- Erge NejmDocument10 pagesErge Nejmliz salcedoNo ratings yet
- Ulkus PeptikumDocument30 pagesUlkus PeptikumRizky Indah SorayaNo ratings yet
- Nejmcp 2114026Document10 pagesNejmcp 2114026Cristina Adriana PopaNo ratings yet
- SLIDE REDACID-dr ANDIDocument40 pagesSLIDE REDACID-dr ANDISyarif HidayatullahNo ratings yet
- GerdDocument38 pagesGerdHoney LaxNo ratings yet
- Gastroesophageal Reflux Disease: Causes, Symptoms, and TreatmentDocument38 pagesGastroesophageal Reflux Disease: Causes, Symptoms, and TreatmentShah Faisal99No ratings yet
- 3 Kuliah GERDDocument40 pages3 Kuliah GERDAnonymous vUEDx8No ratings yet
- Nejmcp 2114026Document10 pagesNejmcp 2114026Engin AltınkayaNo ratings yet
- Dyspepsia: Cengiz Pata Department of Gastroenterology Yeditepe University, IstanbulDocument31 pagesDyspepsia: Cengiz Pata Department of Gastroenterology Yeditepe University, IstanbullusiNo ratings yet
- Dr. K. Sendhil Kumar Dr. Piyush Patwa Dr. Latif Bagwan Gateway Clinic & Hospitals Coimbatore, INDIADocument62 pagesDr. K. Sendhil Kumar Dr. Piyush Patwa Dr. Latif Bagwan Gateway Clinic & Hospitals Coimbatore, INDIAJOPEARL MAE DELA TORRE100% (1)
- GerdDocument19 pagesGerdMuhammad HafizdNo ratings yet
- Managing GERDDocument43 pagesManaging GERDmayi_31kNo ratings yet
- G2 b1 GORDDocument5 pagesG2 b1 GORDJames MooreNo ratings yet
- Gastroesophageal Reflux DiseaseDocument47 pagesGastroesophageal Reflux DiseasePelaminan PekanbaruNo ratings yet
- Gastroesophageal Reflux Disease (GERD)Document37 pagesGastroesophageal Reflux Disease (GERD)CraciunElenaNo ratings yet
- Skdi GehDocument30 pagesSkdi GehviandamayantiNo ratings yet
- GIT DisordersDocument28 pagesGIT DisordersHadeer AnwarNo ratings yet
- Honorary Senior Clinical Lecturer, University of Sheffield Consultant Gastroenterologist Barnsley Hospital NHS Foundation Trust, UKDocument43 pagesHonorary Senior Clinical Lecturer, University of Sheffield Consultant Gastroenterologist Barnsley Hospital NHS Foundation Trust, UKFadilla Putri AmalyaNo ratings yet
- GerdDocument38 pagesGerdjetone472No ratings yet
- Lecture 16 GERDDocument44 pagesLecture 16 GERDSinthuNo ratings yet
- Internal Medicine Board ReviewDocument64 pagesInternal Medicine Board Reviewgrahamabra50% (2)
- Results of Short-And Long-Term Medical Treatment of Gastroesophageal Reflux Disease (GERD)Document7 pagesResults of Short-And Long-Term Medical Treatment of Gastroesophageal Reflux Disease (GERD)Aaquib AmirNo ratings yet
- Palliation of Dysphagia in Locally Advanced Carcinoma Esophagus - Exploration of Two Different Radiotherapy SchedulesDocument3 pagesPalliation of Dysphagia in Locally Advanced Carcinoma Esophagus - Exploration of Two Different Radiotherapy SchedulesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Understanding Peptic Ulcer Disease (PUD): Causes, Symptoms, and TreatmentDocument46 pagesUnderstanding Peptic Ulcer Disease (PUD): Causes, Symptoms, and TreatmentDAveyNo ratings yet
- Perforated Peptic Ulcer - Habib DanielluthDocument15 pagesPerforated Peptic Ulcer - Habib DanielluthDa JunNo ratings yet
- Gastroesophageal Reflux Disease: Scott Stolte, Pharm.D. Shenandoah UniversityDocument48 pagesGastroesophageal Reflux Disease: Scott Stolte, Pharm.D. Shenandoah UniversitymnmrznNo ratings yet
- Assignment: Applied MedicineDocument10 pagesAssignment: Applied MedicineKhadija BakhtawarNo ratings yet
- Oral Exam Gastro 2022Document88 pagesOral Exam Gastro 2022Salih AslaNo ratings yet
- Hiatal Hernia 1Document32 pagesHiatal Hernia 1Candace LongNo ratings yet
- Gerd Blok 2 6Document43 pagesGerd Blok 2 6Mus TofaNo ratings yet
- RGE 002 Consenso CanadaDocument21 pagesRGE 002 Consenso CanadaJavier Alonso Jara CánovasNo ratings yet
- Theodore Liakakos, George Karamanolis, Paul Patapis, and Evangelos P. MisiakosDocument7 pagesTheodore Liakakos, George Karamanolis, Paul Patapis, and Evangelos P. MisiakosDaniel AdityaNo ratings yet
- Sajid SurgeryDocument42 pagesSajid SurgerySajidNo ratings yet
- Gerd PDFDocument51 pagesGerd PDFaddfreNo ratings yet
- GerdDocument51 pagesGerdaddfre100% (1)
- esofagitis eosinofilikDocument13 pagesesofagitis eosinofilikDembabaNo ratings yet
- BMJ - GerdDocument43 pagesBMJ - Gerdwalit ukhri mukrinin0% (1)
- Hyperuricemia Case DiscussionDocument7 pagesHyperuricemia Case DiscussionVineth MartinNo ratings yet
- Case File GERDDocument9 pagesCase File GERDMutiara Shifa100% (1)
- Gerd GuidelineDocument8 pagesGerd Guidelinets8166No ratings yet
- Functional Dyspepsia: Evidences in Pathophysiology and TreatmentFrom EverandFunctional Dyspepsia: Evidences in Pathophysiology and TreatmentKazunari TominagaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Current and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryFrom EverandCurrent and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryNo ratings yet
- Physiology & Pathology of Esophagus (Compatibility Mode)Document39 pagesPhysiology & Pathology of Esophagus (Compatibility Mode)your babysurgeonNo ratings yet
- Diagnosis of Oesophagial Diseases (Compatibility Mode)Document37 pagesDiagnosis of Oesophagial Diseases (Compatibility Mode)your babysurgeonNo ratings yet
- Dysphagia Thinking Outside The BoxDocument15 pagesDysphagia Thinking Outside The Boxyour babysurgeonNo ratings yet
- Anatomy (Compatibility Mode)Document34 pagesAnatomy (Compatibility Mode)your babysurgeonNo ratings yet
- Surg in Ca Oesophagus (Compatibility Mode)Document43 pagesSurg in Ca Oesophagus (Compatibility Mode)your babysurgeonNo ratings yet
- GE Reflux (Compatibility Mode)Document17 pagesGE Reflux (Compatibility Mode)your babysurgeonNo ratings yet
- Carcinoma of Oesophagus Treatment and Survival RatesDocument42 pagesCarcinoma of Oesophagus Treatment and Survival Ratesyour babysurgeonNo ratings yet
- Chronic Pancreatitis: Ermias D (MD)Document30 pagesChronic Pancreatitis: Ermias D (MD)Santomi PratamaNo ratings yet
- Abdominal PainDocument44 pagesAbdominal PainAjo YayanNo ratings yet
- July 27, 2009 Exploratory Laparotomy and Transverse Loop Colostomy 1.Document8 pagesJuly 27, 2009 Exploratory Laparotomy and Transverse Loop Colostomy 1.MaRVNo ratings yet
- Laporan-Diagnosa Januari 2021Document231 pagesLaporan-Diagnosa Januari 2021Putri AnnisaNo ratings yet
- Seminar: Pere Ginès, Aleksander Krag, Juan G Abraldes, Elsa Solà, Núria Fabrellas, Patrick S KamathDocument18 pagesSeminar: Pere Ginès, Aleksander Krag, Juan G Abraldes, Elsa Solà, Núria Fabrellas, Patrick S KamathcastillojessNo ratings yet
- PH Le BotomyDocument15 pagesPH Le BotomyPatty MenéndezNo ratings yet
- Upper GI BleedingDocument70 pagesUpper GI BleedingMia MusNo ratings yet
- Professional Guide To Signs and Symptoms 6th Edition PDFDocument822 pagesProfessional Guide To Signs and Symptoms 6th Edition PDF1102sn83% (6)
- SurgicalDocument288 pagesSurgicalSalih Asla0% (1)
- Health Benefits of The Natural Squatting PositionDocument43 pagesHealth Benefits of The Natural Squatting PositionkeanshengNo ratings yet
- Colecistitis LitiasicaDocument25 pagesColecistitis LitiasicaLuis Adolfo Ramos CastilloNo ratings yet
- GallstonesDocument17 pagesGallstonesع ب و دNo ratings yet
- Diverticular DiseaseDocument8 pagesDiverticular Diseasenurse_enzo100% (1)
- Anatomy and Physiology of The Digestive System: Dipali HarkhaniDocument83 pagesAnatomy and Physiology of The Digestive System: Dipali HarkhaniPatel archiNo ratings yet
- Gastric SecretionDocument50 pagesGastric SecretionYanglem AmarjitNo ratings yet
- 1stQ SCIENCE - Answer Key-ADMU-Gr4Document4 pages1stQ SCIENCE - Answer Key-ADMU-Gr4flower.power11233986No ratings yet
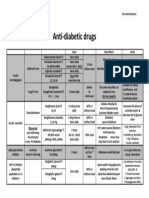
- Anti Diabetic DrugsDocument1 pageAnti Diabetic DrugsWael hadNo ratings yet
- Liver DiseaseDocument19 pagesLiver Diseasenishi kNo ratings yet
- CONSTIPATIONDocument4 pagesCONSTIPATIONKarl Angelo MontanoNo ratings yet
- Case Presentation (October 3)Document54 pagesCase Presentation (October 3)Ayessa Camelle DumileNo ratings yet
- PneumoperitoneumDocument15 pagesPneumoperitoneumMuhammad Dimas PangestuNo ratings yet
- 2020 Third PeriodicalDocument7 pages2020 Third PeriodicalJhun Jan DieNo ratings yet
- Prosiding BioMic AS7213619746078721548997505149 - Content - 1Document6 pagesProsiding BioMic AS7213619746078721548997505149 - Content - 1Nur KusmiyatiNo ratings yet
- Case 13 Case StudyDocument8 pagesCase 13 Case Studyklee100% (2)
- ESEGH 2021 ReportDocument4 pagesESEGH 2021 ReportAsif.N.IqbalNo ratings yet
- Frog DissectionDocument4 pagesFrog Dissection2110038No ratings yet
- Digestive System - SummaryDocument15 pagesDigestive System - Summarys.tinaja.marieantonetteNo ratings yet
- Balantidium ColiDocument5 pagesBalantidium Coliglorya barbessNo ratings yet
- Fisiologi DefekasiDocument9 pagesFisiologi DefekasiAmirullah AbdiNo ratings yet
- MSN I 25.06 .2020 AN Unit IV. Small Intestinal Malabsorption & ObstructionDocument92 pagesMSN I 25.06 .2020 AN Unit IV. Small Intestinal Malabsorption & ObstructionYAMINIPRIYAN0% (1)