You might also like
- MannitolDocument20 pagesMannitolSabrina ShalhoutNo ratings yet
- For Intravenous Use and Urologic Irrigation: MANNITOL-mannitol Injection, S Olution Fres Enius Kabi USA, LLCDocument7 pagesFor Intravenous Use and Urologic Irrigation: MANNITOL-mannitol Injection, S Olution Fres Enius Kabi USA, LLCroykelumendekNo ratings yet
- 8.5 Infusion of Hypertonic Mannitol Solutions: Fluid PhysiologyDocument2 pages8.5 Infusion of Hypertonic Mannitol Solutions: Fluid Physiologyicen00bNo ratings yet
- Dailymed - Nlm.nih - Gov-20 Mannitol Injection USPDocument12 pagesDailymed - Nlm.nih - Gov-20 Mannitol Injection USPLip StickNo ratings yet
- ManitolDocument20 pagesManitolkr PadmanabhanNo ratings yet
- Obat - Obatan Di Bedah SarafDocument16 pagesObat - Obatan Di Bedah Sarafditya_madridistasNo ratings yet
- IV Mannitol - Expanding Perspectives For Use in Neurogenic Inflammation & Neuropathic PainDocument64 pagesIV Mannitol - Expanding Perspectives For Use in Neurogenic Inflammation & Neuropathic PainmuhammadNo ratings yet
- Mannitol Baxter Viaflo Sol F Inf ENGDocument10 pagesMannitol Baxter Viaflo Sol F Inf ENGBojan BjelajacNo ratings yet
- MannitolDocument2 pagesMannitolRyan OnellNo ratings yet
- MANITOL for edema and increased intracranial pressureDocument6 pagesMANITOL for edema and increased intracranial pressureIvana YunitaNo ratings yet
- Drug Study MannitolDocument2 pagesDrug Study Mannitoljasielle80% (5)
- MannitolDocument1 pageMannitolubaidNo ratings yet
- Jnacc Jnacc 31.17Document9 pagesJnacc Jnacc 31.17Shabrina Amalia SuciNo ratings yet
- Mannitol and PhenytoinDocument15 pagesMannitol and PhenytoinirmaNo ratings yet
- AcetazolamideDocument4 pagesAcetazolamideAmarnath SahNo ratings yet
- RX - Citicoline, Kalium, Ketosteril, Methycobal, Myonal, Lipolin GelDocument6 pagesRX - Citicoline, Kalium, Ketosteril, Methycobal, Myonal, Lipolin GelntootNo ratings yet
- Drugs Acting on the Gastrointestinal SystemDocument41 pagesDrugs Acting on the Gastrointestinal SystemDivya JoyNo ratings yet
- Medications: LorsartanDocument3 pagesMedications: LorsartanJoy DunwanNo ratings yet
- Hyperglycemic H-WPS OfficeDocument4 pagesHyperglycemic H-WPS OfficeShiehan Mae ForroNo ratings yet
- Drugs For Constipation and DiarrheaDocument40 pagesDrugs For Constipation and DiarrheagirgrayNo ratings yet
- Skema HipertensiDocument4 pagesSkema HipertensiAndri wijayaNo ratings yet
- Anti EmeticsDocument112 pagesAnti Emeticsjoel david knda mjNo ratings yet
- Gastrointestinal Disorders GuideDocument4 pagesGastrointestinal Disorders GuideCarissa Mae Tapec EstradaNo ratings yet
- Mannitol: It'S Place in Current Clinical PracticeDocument11 pagesMannitol: It'S Place in Current Clinical PracticecardiacanesthesiaNo ratings yet
- Pharma 2017Document48 pagesPharma 2017backupuoload85No ratings yet
- NR 446 ATI Weekly Tips Week 2 PharmacologyDocument9 pagesNR 446 ATI Weekly Tips Week 2 PharmacologyChristine Lansdown100% (1)
- Lipid Lowering Agents IDocument14 pagesLipid Lowering Agents IRALPH ELVIN MACANLALAYNo ratings yet
- M3 - Lesson 1bDocument20 pagesM3 - Lesson 1bLhara MañoNo ratings yet
- Drugs Acting On: Renal SystemDocument75 pagesDrugs Acting On: Renal SystemCarlojay IniegoNo ratings yet
- Pharm Review For Hesi From JanaDocument8 pagesPharm Review For Hesi From Janacheyenne.black5205100% (1)
- Monitoring side effects of octreotide acetateDocument32 pagesMonitoring side effects of octreotide acetatemelissamichellle100% (2)
- Unit VI Drugs used on urinary systemDocument46 pagesUnit VI Drugs used on urinary systemHarshika KDGNo ratings yet
- Meds Affecting Blood PressureDocument5 pagesMeds Affecting Blood PressuremikiNo ratings yet
- LECTURE 8 AntihypertensiveDocument18 pagesLECTURE 8 AntihypertensiveanaNo ratings yet
- MannitolDocument8 pagesMannitolkristiandiorcapiliNo ratings yet
- Drugs Increased Risk of DiabetesDocument5 pagesDrugs Increased Risk of Diabetesk9cfxtdfqmNo ratings yet
- Document 1Document4 pagesDocument 1kamaluNo ratings yet
- Pharma 2016Document48 pagesPharma 2016backupuoload85No ratings yet
- Mannitol: An Osmotic Diuretic AgentDocument3 pagesMannitol: An Osmotic Diuretic AgentAmit MartinNo ratings yet
- Liver cirrhosis complications and managementDocument39 pagesLiver cirrhosis complications and managementДенис КовшNo ratings yet
- MannitolDocument4 pagesMannitolConn_Casipe_8158100% (1)
- methotrexate-Anti-Asthmatic Drugs Toxicity-1Document9 pagesmethotrexate-Anti-Asthmatic Drugs Toxicity-1joonabil29No ratings yet
- Drugs Study Neh Jai2xDocument10 pagesDrugs Study Neh Jai2xjai2xNo ratings yet
- Drugs and Kidney DiseasesDocument46 pagesDrugs and Kidney Diseasesمرتضى محمد فاضل جرجوكNo ratings yet
- Mannitol for Medical UsesDocument7 pagesMannitol for Medical UsesJuri GallosNo ratings yet
- Drug Study UsesDocument2 pagesDrug Study UsesSHARMAINE ANNE POLICIOSNo ratings yet
- Mannitol and Dexamethasone Drug Study SummaryDocument8 pagesMannitol and Dexamethasone Drug Study SummaryKath RubioNo ratings yet
- Drugs Used in Gastrointestinal Diseases TreatmentDocument52 pagesDrugs Used in Gastrointestinal Diseases TreatmentWidia Isa Aprillia SujanaNo ratings yet
- Activity No. 5 Principles of DialysisDocument5 pagesActivity No. 5 Principles of DialysisKatrina Dela CruzNo ratings yet
- Drug StudyDocument7 pagesDrug Studykymsh_kimNo ratings yet
- Metformin 1 METFORMIN (500mg, 850mg and 1000mg Tablets) : New Zealand Data SheetDocument11 pagesMetformin 1 METFORMIN (500mg, 850mg and 1000mg Tablets) : New Zealand Data SheetAfifa ZainNo ratings yet
- Routes of Excretion Routes of Excretion Renal Excretion Non Renal Excretion Biliary ExcretionDocument5 pagesRoutes of Excretion Routes of Excretion Renal Excretion Non Renal Excretion Biliary Excretiontanuja reddyNo ratings yet
- Anesthesia in Hepatic DiseaseDocument3 pagesAnesthesia in Hepatic DiseaseRoxana SurliuNo ratings yet
- Urea Cycle Disorders - Management - UpToDateDocument21 pagesUrea Cycle Disorders - Management - UpToDatePIERINANo ratings yet
- Cardiotonic DrugsDocument67 pagesCardiotonic DrugsLady Mae Ramos100% (1)
- Central Diabetes InsipidusDocument8 pagesCentral Diabetes InsipidusasdwasdNo ratings yet
- Nalepsin: Presentation Drug InteractionsDocument1 pageNalepsin: Presentation Drug InteractionsAbid Hasan ZiKonNo ratings yet
- Management of Diarrhea: Non-Drug and Drug TherapyDocument40 pagesManagement of Diarrhea: Non-Drug and Drug TherapyNofilia Citra CandraNo ratings yet
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Tomassoni2008 PDFDocument23 pagesTomassoni2008 PDFMachlery KunNo ratings yet
- Tratamiento de Edema Cerebral 2020Document20 pagesTratamiento de Edema Cerebral 2020Nilger AlarconNo ratings yet
- Transform Hemoragik INA 2019Document8 pagesTransform Hemoragik INA 2019winnerfromparisNo ratings yet
- Hemoragik TransformasiDocument5 pagesHemoragik TransformasiPPDS Neurologi USK 12No ratings yet
- Absolute and Relative Contraindication To IV Rt-Pca For Acute Ischemic StrokeDocument12 pagesAbsolute and Relative Contraindication To IV Rt-Pca For Acute Ischemic StrokePPDS Neurologi USK 12No ratings yet
- Fact Shett - OSHADocument2 pagesFact Shett - OSHALuiz Rubens Souza CantelliNo ratings yet
- Material Transfer Agreement: Klinikum Rechts Der Isar Der Technischen Universität MünchenDocument9 pagesMaterial Transfer Agreement: Klinikum Rechts Der Isar Der Technischen Universität MünchenchristinaNo ratings yet
- Jean Kilbourne 1999 Can T Buy My Love. How Advertising Changes The Way We Think and FeelDocument28 pagesJean Kilbourne 1999 Can T Buy My Love. How Advertising Changes The Way We Think and FeelMads Den0% (1)
- AphasiaDocument28 pagesAphasiaEmilio Emmanué Escobar CruzNo ratings yet
- Flutter and Other DeviceDocument39 pagesFlutter and Other DeviceEira LopezNo ratings yet
- Dr. Vera CruzDocument9 pagesDr. Vera CruzPatrick John BatolNo ratings yet
- Congenital Adrenal HyperplasiaDocument5 pagesCongenital Adrenal HyperplasiaduapajNo ratings yet
- 2nd Announcement JakNews 2024Document19 pages2nd Announcement JakNews 2024Nando EllaNo ratings yet
- Skor Tokolitik PDFDocument5 pagesSkor Tokolitik PDFrahayu muhsiNo ratings yet
- INBDE Practice QuestionsDocument58 pagesINBDE Practice QuestionsFarhan Hossain100% (4)
- Mindray Beneview t1 Operator Manual (FDA)Document204 pagesMindray Beneview t1 Operator Manual (FDA)hernan1970No ratings yet
- PointersDocument4 pagesPointersJayson MontemayorNo ratings yet
- Phytochemical and Pharmacological Review of Maja (Aegle Marmelos)Document24 pagesPhytochemical and Pharmacological Review of Maja (Aegle Marmelos)h_rivaiNo ratings yet
- Bupivacaine (Marcaine)Document2 pagesBupivacaine (Marcaine)Michalis SpyridakisNo ratings yet
- BilastineDocument1 pageBilastineCharess Candelon - SengcoNo ratings yet
- Differential Diagnosis of WeaknessDocument6 pagesDifferential Diagnosis of WeaknessAna LydiaNo ratings yet
- Sleep, Dreams, & More (: Exploring Consciousness)Document46 pagesSleep, Dreams, & More (: Exploring Consciousness)Sheila G. DolipasNo ratings yet
- RIG WASH For BargesDocument5 pagesRIG WASH For BargesUnokhogie EmmanuelNo ratings yet
- Dr.T.V.Rao MD 1Document39 pagesDr.T.V.Rao MD 1tummalapalli venkateswara raoNo ratings yet
- E-Cat 2023 Medical Equipment Price List with Item DetailsDocument2 pagesE-Cat 2023 Medical Equipment Price List with Item Detailsade maulanaNo ratings yet
- HVAC Systems for Health Care Facilities ConferenceDocument75 pagesHVAC Systems for Health Care Facilities ConferenceAhmed AbdelzaherNo ratings yet
- Adoption of Plea Bargaining Framework in Drug CasesDocument10 pagesAdoption of Plea Bargaining Framework in Drug CasesMagtanggol HinirangNo ratings yet
- 9781907816444Document12 pages9781907816444Dr.yeasin Arafat100% (1)
- ) The Right Answer: Instructions:-Q.1 A. Multiple Choice Questions - 10 X 1 10Document2 pages) The Right Answer: Instructions:-Q.1 A. Multiple Choice Questions - 10 X 1 10swapnil goyalNo ratings yet
- Production of Anti-Bacterial Soap Using (Natural Ingredients)Document1 pageProduction of Anti-Bacterial Soap Using (Natural Ingredients)Nabilah MustafaNo ratings yet
- Research About Tuba TubaDocument20 pagesResearch About Tuba Tubakoala1388No ratings yet
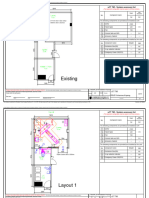
- Desain Ruangan CT-ScanDocument3 pagesDesain Ruangan CT-ScannewmanonmarsNo ratings yet
- Oxycodone OxycontinDocument5 pagesOxycodone Oxycontinjhay2112No ratings yet
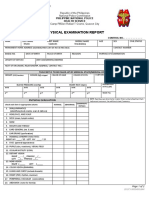
- PNP HS MS Form Physical ExamDocument2 pagesPNP HS MS Form Physical Examlara michelleNo ratings yet
- DECS Upholds Rule Barring 4th NMAT AttemptDocument6 pagesDECS Upholds Rule Barring 4th NMAT AttemptDanyNo ratings yet