You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Urban Mobility in Kathmandu: Status and TrendsDocument8 pagesUrban Mobility in Kathmandu: Status and TrendsAdwait LimayeNo ratings yet
- Forcetriad Value Analysis Brief - ValleyLabDocument10 pagesForcetriad Value Analysis Brief - ValleyLabmelquisedecNo ratings yet
- Psychological Test in Counselling (New)Document35 pagesPsychological Test in Counselling (New)Shiek LukmanNo ratings yet
- Research Paper Chapter 1 To 5 SlideshareDocument7 pagesResearch Paper Chapter 1 To 5 Slidesharepwvgqccnd100% (1)
- Hale, Are Lesbians Women PDFDocument6 pagesHale, Are Lesbians Women PDFTharántula MulatuNo ratings yet
- Natura Bisse Facial MenuDocument1 pageNatura Bisse Facial MenuRhea MuthaNo ratings yet
- SRM01-07A Keys To The AsylumDocument21 pagesSRM01-07A Keys To The AsylumMurillo Belvel FernandesNo ratings yet
- A Descriptive-Comparative StudyDocument32 pagesA Descriptive-Comparative StudyJanelle DionisioNo ratings yet
- At The Hospital Quick Reference Glossary PDFDocument12 pagesAt The Hospital Quick Reference Glossary PDFFaisal IqbalNo ratings yet
- Jaundice PDFDocument7 pagesJaundice PDFSib AsuncionNo ratings yet
- Skripsi Andi Rizal TaherDocument73 pagesSkripsi Andi Rizal Taherimanudin kamilNo ratings yet
- Health and Remedies Information Gap Activities - 141815Document6 pagesHealth and Remedies Information Gap Activities - 141815Andrés DíazNo ratings yet
- Assignment 3: Consumer LearningDocument4 pagesAssignment 3: Consumer LearninglaibaNo ratings yet
- Gendam TranslatedDocument37 pagesGendam TranslatedSaket RaiNo ratings yet
- Task 2 Engineering English (Redho Triwinoko, METO 5B)Document3 pagesTask 2 Engineering English (Redho Triwinoko, METO 5B)Redho TriwinokoNo ratings yet
- PressedDocument2 pagesPressedCathy ChuiNo ratings yet
- Dr. Agussalim Bukhari, M.Med, PH.D, SP - GK (K)Document47 pagesDr. Agussalim Bukhari, M.Med, PH.D, SP - GK (K)Vika LeiwaNo ratings yet
- The Mysterious Death of Dr. SebiDocument15 pagesThe Mysterious Death of Dr. SebiJason Carter100% (1)
- Njoro Canning Factory ContractDocument2 pagesNjoro Canning Factory ContractCannon GaddafiNo ratings yet
- Child Care and Child Abuse in Early Medieval EuropeDocument7 pagesChild Care and Child Abuse in Early Medieval EuropeMariana BarcenasNo ratings yet
- Definition, Etiology, and Clinical Manifestations of Transient Ischemic Attack - UpToDateDocument48 pagesDefinition, Etiology, and Clinical Manifestations of Transient Ischemic Attack - UpToDateHossdana JimenezNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) Is A Condition ofDocument12 pagesChronic Obstructive Pulmonary Disease (COPD) Is A Condition ofDiana Jalaynie S. SambolawanNo ratings yet
- Russell-Taylor Delta-Tibial Interlocking Nail TechniqueDocument30 pagesRussell-Taylor Delta-Tibial Interlocking Nail TechniquemikeydamanNo ratings yet
- MSDS UreaDocument4 pagesMSDS UreaSharjeel AhmedNo ratings yet
- Auditory DisordersDocument19 pagesAuditory DisordersJobelle AcenaNo ratings yet
- Benefits of HijamaDocument3 pagesBenefits of HijamaBateria MeaNo ratings yet
- UNKNOWNDocument13 pagesUNKNOWNnhayrahdicunugunNo ratings yet
- Rhetorical Analysis FinalDocument6 pagesRhetorical Analysis Finalapi-500722562No ratings yet
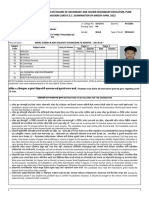
- Maharashtra State Board of Secondary and Higher Secondary Education, Pune Admission Card H.S.C. Examination of March-April 2022Document3 pagesMaharashtra State Board of Secondary and Higher Secondary Education, Pune Admission Card H.S.C. Examination of March-April 2022PANKAJ WANDHARENo ratings yet
- Executive Intelligence Rural Development Leadership and The Leadership of Prof - Dr.Krasae ChanawongseDocument90 pagesExecutive Intelligence Rural Development Leadership and The Leadership of Prof - Dr.Krasae ChanawongseadkittipongNo ratings yet