You might also like
- Asme P NumberDocument2 pagesAsme P Numbersandesh_honraoNo ratings yet
- Manual Kenwood TM 710Document55 pagesManual Kenwood TM 710Lemos FerreiraNo ratings yet
- Weldability Test For Thin Sheet MaterialsDocument6 pagesWeldability Test For Thin Sheet MaterialsAnonymous FHkX0ANo ratings yet
- Lightning Brochure18Document2 pagesLightning Brochure18Matt GunnNo ratings yet
- Crisis Background GuideDocument21 pagesCrisis Background GuideJohn GiambalvoNo ratings yet
- US Navy Engineering Aid BasicsDocument41 pagesUS Navy Engineering Aid BasicsteddyNo ratings yet
- Welding Student TasksDocument157 pagesWelding Student TasksbilalyunusNo ratings yet
- Hot Forming/Bending: Material BS 806 ANSI B 31.1 DIN 17175 MannessmanDocument3 pagesHot Forming/Bending: Material BS 806 ANSI B 31.1 DIN 17175 Mannessmandnageshm4n244No ratings yet
- Basic Principles of Torque Wrenches & Bolt Tensioners - Sanger MetalDocument3 pagesBasic Principles of Torque Wrenches & Bolt Tensioners - Sanger Metalbalasekar100% (1)
- Welding Math (And Some Physics)Document4 pagesWelding Math (And Some Physics)wasim_akp9885100% (1)
- Introduction To Penetrant TestingDocument61 pagesIntroduction To Penetrant TestingjerryceppyNo ratings yet
- Guidelines For Welding Dissimilar Metals PDFDocument8 pagesGuidelines For Welding Dissimilar Metals PDFbanglvhNo ratings yet
- Welders Hand BookDocument23 pagesWelders Hand Booksamyqatar100% (2)
- Guideline For Hand Soldering PracticesDocument10 pagesGuideline For Hand Soldering PracticessrtrtyrtNo ratings yet
- F747-06 Standard Terminology Relating To Amusement Rides and DevicesDocument2 pagesF747-06 Standard Terminology Relating To Amusement Rides and DevicesachatsabmsNo ratings yet
- Fed STD 191aDocument946 pagesFed STD 191aSubdis MatbekNo ratings yet
- Weld Cost Calc XL1.3.2mmDocument3 pagesWeld Cost Calc XL1.3.2mmDhimas Surya NegaraNo ratings yet
- Australian EwDocument25 pagesAustralian Ewsuneerav17No ratings yet
- Sample WPS Form (GTAW & SMAW) Welding Procedure Specification (WPS)Document1 pageSample WPS Form (GTAW & SMAW) Welding Procedure Specification (WPS)Daniel Simar Herrera MorenoNo ratings yet
- Licensed by Information Handling Services Licensed by Information Handling ServicesDocument147 pagesLicensed by Information Handling Services Licensed by Information Handling Servicesrogel_ganaNo ratings yet
- Intro MIG Welding PDFDocument16 pagesIntro MIG Welding PDFHtet MyatNo ratings yet
- Ansi Z35 1 1968Document21 pagesAnsi Z35 1 1968Daniel ReyesNo ratings yet
- Welding Engineering - FALL2021-22 - Module 1Document44 pagesWelding Engineering - FALL2021-22 - Module 1dhaya nidhiNo ratings yet
- Advanced Gas Metal Arc Welding ProcDocument20 pagesAdvanced Gas Metal Arc Welding ProcjavadmohammadiNo ratings yet
- MIG Welding Basics On MIG Welding Machines.20121010.095920Document2 pagesMIG Welding Basics On MIG Welding Machines.20121010.095920anon_516042600No ratings yet
- Weld Test Stand Assembly ManualDocument9 pagesWeld Test Stand Assembly ManualLUIS CORDOVA ZANCHESNo ratings yet
- Welding: Subpart QDocument65 pagesWelding: Subpart QRathnakrajaNo ratings yet
- US Army Welding Operations IIDocument80 pagesUS Army Welding Operations IISpace_HulkerNo ratings yet
- Hydrogen Embrittlement of An Interstitia PDFDocument6 pagesHydrogen Embrittlement of An Interstitia PDFArdu StuffNo ratings yet
- Cutmaster 81Document4 pagesCutmaster 81Silverio JaimeNo ratings yet
- Welding For ReferenceDocument159 pagesWelding For ReferenceRomoex R RockNo ratings yet
- Mil HDBK Ultrasonic TestingDocument90 pagesMil HDBK Ultrasonic TestingJoel SequeiraNo ratings yet
- The Mortise and Tenon Joint: Best Results Come Directly From Chisel and SawDocument6 pagesThe Mortise and Tenon Joint: Best Results Come Directly From Chisel and SawAdrian Cocis100% (1)
- Arc Welding ProjectDocument11 pagesArc Welding ProjectLeahNo ratings yet
- G-0048 - Pitting and Crevice Corrosion Resistance of Stainless Steels and Related Alloys by Use of Ferric Chloride Solution PDFDocument11 pagesG-0048 - Pitting and Crevice Corrosion Resistance of Stainless Steels and Related Alloys by Use of Ferric Chloride Solution PDFEwan SutherlandNo ratings yet
- The Death of Welding InspectorDocument1 pageThe Death of Welding Inspectormekag94100% (1)
- Cow SpreadsheetDocument28 pagesCow SpreadsheetSunilGangwarNo ratings yet
- US Army Medical Course MD0033-100 - Tort Law, The Federal Tort Claims Act, and The Geneva ConventionDocument36 pagesUS Army Medical Course MD0033-100 - Tort Law, The Federal Tort Claims Act, and The Geneva ConventionGeorges100% (2)
- Welding DictionaryDocument59 pagesWelding DictionaryRathnakraja100% (1)
- Ionizing Radiation Safety Training GAoF1vzNDocument26 pagesIonizing Radiation Safety Training GAoF1vzN90x93 -No ratings yet
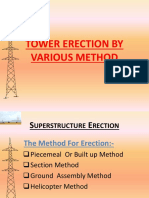
- Tower Erection by Various MethodDocument30 pagesTower Erection by Various MethodJaydip NathNo ratings yet
- AISE Anchor Bolt Details PDFDocument1 pageAISE Anchor Bolt Details PDFYash PaulNo ratings yet
- Lessons Learned From "Lessons Learned": The Evolution of Nuclear Power Safety After Accidents and Near-AccidentsDocument38 pagesLessons Learned From "Lessons Learned": The Evolution of Nuclear Power Safety After Accidents and Near-AccidentsLayla DawoodNo ratings yet
- Powermax1650 Operator ManualDocument98 pagesPowermax1650 Operator ManualcostelchelariuNo ratings yet
- Lawrence Ross FAQ 20200629Document31 pagesLawrence Ross FAQ 20200629John RangelNo ratings yet
- ANSI+NEMA+Z535.3-2011 Poin A Safety SignDocument13 pagesANSI+NEMA+Z535.3-2011 Poin A Safety SignPutu Gede Oka MNo ratings yet
- API 1110 Additional Procedure ReportDocument36 pagesAPI 1110 Additional Procedure ReportMohamed Mostafa100% (1)
- The Terms of The Contract-Rock and Roll and The Narrative of Self-Destruction in Don DeLillo, Neal Pollack, and Kurt CobainDocument19 pagesThe Terms of The Contract-Rock and Roll and The Narrative of Self-Destruction in Don DeLillo, Neal Pollack, and Kurt CobainTyler SmithNo ratings yet
- Cambering Steel BeamsDocument2 pagesCambering Steel BeamsFernando PizarroNo ratings yet
- Accident - Incident InvestigationDocument7 pagesAccident - Incident InvestigationAdeel AhmedNo ratings yet
- Hello!: I Am Abhishek PunyaniDocument32 pagesHello!: I Am Abhishek Punyanichirag goelNo ratings yet
- TACOM Weld Code - Alumn (12472301A)Document123 pagesTACOM Weld Code - Alumn (12472301A)mtcengineeringNo ratings yet
- 6010 5P+ Welding Rod-LincolnDocument4 pages6010 5P+ Welding Rod-LincolnjanprakkeNo ratings yet
- Pandemic Crisis PlanDocument50 pagesPandemic Crisis PlanMohan100% (1)
- Doh Irr Ra11332Document14 pagesDoh Irr Ra11332Creativ WorxNo ratings yet
- Knowledge, and Practice Towards Infection Control Measures For The Novel Corona Virus Among Nurses Working at Isolation DepartmentDocument49 pagesKnowledge, and Practice Towards Infection Control Measures For The Novel Corona Virus Among Nurses Working at Isolation DepartmentOmima MuhammedNo ratings yet
- Dossier 1 - Epidemics and Pandemics - General GuidelinesDocument20 pagesDossier 1 - Epidemics and Pandemics - General Guidelinestellmeprojecteu100% (1)
- University of Washington Comm Disease Outbreak Management Plan Feb 2020 Working DRAFTDocument39 pagesUniversity of Washington Comm Disease Outbreak Management Plan Feb 2020 Working DRAFTRaza Muhammad SoomroNo ratings yet
- Interim Clinical Guidelines On Severe Acute Respiratory Syndrome (SARS) For Health Facilities in The PhilippinesDocument21 pagesInterim Clinical Guidelines On Severe Acute Respiratory Syndrome (SARS) For Health Facilities in The PhilippinesAlma Bertos-AgubNo ratings yet
- Paho Moh Manual - Infection Prevention and Control PoliciesDocument59 pagesPaho Moh Manual - Infection Prevention and Control PoliciesElaine UrgeNo ratings yet
- The Vibration of Exceptional Health - Carol LookDocument5 pagesThe Vibration of Exceptional Health - Carol LookMichael CliftonNo ratings yet
- Section 2 Aerobic Gram Positive Bacilli: Susceptibility Manual MB 0810.08Document29 pagesSection 2 Aerobic Gram Positive Bacilli: Susceptibility Manual MB 0810.08Ahmed Goma'aNo ratings yet
- MARCH 2017 NDP Accomplishment Report Sulat Eastern SamarDocument21 pagesMARCH 2017 NDP Accomplishment Report Sulat Eastern SamarEden VblagasyNo ratings yet
- Heat Stress Toolbox TopicsDocument6 pagesHeat Stress Toolbox TopicsSammie WilliamsNo ratings yet
- Course SyllabusDocument6 pagesCourse Syllabusapi-356391957No ratings yet
- Ajmcr-10-10-2 PublishedDocument5 pagesAjmcr-10-10-2 PublishedsaNo ratings yet
- Airasia Goinsure Travel Insurance Protection - Return International PlanDocument55 pagesAirasia Goinsure Travel Insurance Protection - Return International Planjude1817No ratings yet
- Sample of Quick USMLE Review Notes2Document27 pagesSample of Quick USMLE Review Notes2filchibuffNo ratings yet
- COVID-Statement Leading To Infection.Document3 pagesCOVID-Statement Leading To Infection.William EnocNo ratings yet
- Shorewood Forest PortfolioDocument17 pagesShorewood Forest PortfolioJennifer GillNo ratings yet
- DeGowin's Diagnostic Examination (8th Ed)Document306 pagesDeGowin's Diagnostic Examination (8th Ed)Farah Syazana100% (1)
- Lecture 1 - Introduction To MicrobiologyDocument27 pagesLecture 1 - Introduction To Microbiologyapi-3703352100% (5)
- Nature or NurtureDocument32 pagesNature or NurtureSerendipity PaulNo ratings yet
- 06 Offline Module CourseDocument15 pages06 Offline Module CourseDylan Angelo AndresNo ratings yet
- Cannabis FactsDocument2 pagesCannabis FactsWes WeidleNo ratings yet
- Lifestyle PresentationDocument24 pagesLifestyle Presentationa2o1No ratings yet
- Verapamil HCL Drug StudyDocument3 pagesVerapamil HCL Drug StudyCheezy Bread100% (1)
- Manual of Procedures For The Surveillance Outbreak Investigation and Response To Microbial Agents of Food and Waterborne DiseasesDocument323 pagesManual of Procedures For The Surveillance Outbreak Investigation and Response To Microbial Agents of Food and Waterborne DiseasesGer-Anne BattulayanNo ratings yet
- BM I Chart GirlsDocument1 pageBM I Chart GirlscjgeronimoNo ratings yet
- Education Section On Psychosomatics: The Search For Meaning: The International Journal ofDocument23 pagesEducation Section On Psychosomatics: The Search For Meaning: The International Journal ofJorge LusagaNo ratings yet
- CHN Lecture Module 7 Doh Programs Related To Family HealthDocument42 pagesCHN Lecture Module 7 Doh Programs Related To Family HealthMhianne SarmientoNo ratings yet
- Free RecallDocument10 pagesFree RecallMarcelli T. MerinoNo ratings yet
- Hema, Onco, Cardiology Review NotesDocument9 pagesHema, Onco, Cardiology Review Notesjeshema100% (1)
- Pulmonary FibrosisDocument4 pagesPulmonary FibrosisDimpal Choudhary100% (2)
- Asta KarmasDocument11 pagesAsta KarmasAdriano BarbirNo ratings yet
- UntitledDocument340 pagesUntitledAlistair KohNo ratings yet
- The Medical Detectives PDFDocument3 pagesThe Medical Detectives PDFTharun kumarNo ratings yet
- Gluten-Free Diet TipsheetDocument2 pagesGluten-Free Diet Tipsheetapi-392216729100% (2)
- Lukoff - Mysticism and PsychosisDocument27 pagesLukoff - Mysticism and Psychosiscurfexxx100% (1)
- The Science of NutritionalDocument738 pagesThe Science of NutritionalMonching Adecer100% (1)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Triggers: How We Can Stop Reacting and Start HealingFrom EverandTriggers: How We Can Stop Reacting and Start HealingRating: 5 out of 5 stars5/5 (58)
- Embrace Your Weird: Face Your Fears and Unleash CreativityFrom EverandEmbrace Your Weird: Face Your Fears and Unleash CreativityRating: 4.5 out of 5 stars4.5/5 (124)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Are You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersFrom EverandAre You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersRating: 5 out of 5 stars5/5 (29)
- The Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.From EverandThe Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.Rating: 5 out of 5 stars5/5 (14)
- Vagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerFrom EverandVagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerRating: 4.5 out of 5 stars4.5/5 (16)
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1244)
- The Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItFrom EverandThe Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (107)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)