You might also like
- G12 IB Math SL Probability and Probability DistributionsDocument2 pagesG12 IB Math SL Probability and Probability DistributionsFerdinand AguilaNo ratings yet
- TiKi TaKa CK Preventive MedicineDocument3 pagesTiKi TaKa CK Preventive MedicinenonsNo ratings yet
- Exercise Therapy For The Management of Osteoarthritis of The Hip JointDocument33 pagesExercise Therapy For The Management of Osteoarthritis of The Hip JointVictor Andrés Olivares IbarraNo ratings yet
- NICE Way to Cure COVID -19From EverandNICE Way to Cure COVID -19Rating: 4.5 out of 5 stars4.5/5 (8)
- IBM TapeDocument11 pagesIBM TapeDaWheng VargasNo ratings yet
- CV-X Series Setup Manual (3D) - ESPDocument122 pagesCV-X Series Setup Manual (3D) - ESPJuan Antonio SánchezNo ratings yet
- Nokia 7750 SR-a Service Router Customer Overview Presentation (Level 1)Document38 pagesNokia 7750 SR-a Service Router Customer Overview Presentation (Level 1)NisaiyhoutNo ratings yet
- Drug Study: Francisco Tampos JRDocument37 pagesDrug Study: Francisco Tampos JRCarlmeister Ambray JudillaNo ratings yet
- Green Book, Methods For The Determination of Possible Damage, CPR 16EDocument337 pagesGreen Book, Methods For The Determination of Possible Damage, CPR 16Ejeremyg998100% (8)
- Brief Communication: Infectious Diseases, Microbiology & ParasitologyDocument6 pagesBrief Communication: Infectious Diseases, Microbiology & ParasitologyMiguel Angel Tovar PirelaNo ratings yet
- Liu2020 Article ClinicalAndBiochemicalIndexesFDocument11 pagesLiu2020 Article ClinicalAndBiochemicalIndexesFGabriel Ibarra TrujilloNo ratings yet
- Jurnal Chen Et AlDocument31 pagesJurnal Chen Et AlUtami MNo ratings yet
- Epidemiological and Clinical Characteristics of 671 COVID-19 Patients in Henan Province, ChinaDocument11 pagesEpidemiological and Clinical Characteristics of 671 COVID-19 Patients in Henan Province, ChinaOrlando JúniorNo ratings yet
- Jkms 35 E149Document8 pagesJkms 35 E149TEO COAQUIRANo ratings yet
- JMV 25815Document2 pagesJMV 25815fadil ahmadiNo ratings yet
- NEJM. COVID CHINA. 10.1056@NEJMoa2002032Document13 pagesNEJM. COVID CHINA. 10.1056@NEJMoa2002032Boris CabreraNo ratings yet
- Journal Pre-Proof: Journal of Clinical VirologyDocument12 pagesJournal Pre-Proof: Journal of Clinical VirologymiNo ratings yet
- Clinical Microbiology and InfectionDocument6 pagesClinical Microbiology and InfectionRaghu NadhNo ratings yet
- Aksungar 2007Document10 pagesAksungar 2007twarrenNo ratings yet
- Journal Pre-Proof: Journal of Microbiology, Immunology and InfectionDocument22 pagesJournal Pre-Proof: Journal of Microbiology, Immunology and InfectionLulut KusumawatiNo ratings yet
- Clinico-Radiological Profile in Covid - 19 PatientsDocument6 pagesClinico-Radiological Profile in Covid - 19 PatientsInternational Journal of Innovative Science and Research Technology100% (1)
- A Case Series Describing The Epidemiology and Clinical Characteristics of COVID-19 Infection in Jilin ProvinceDocument4 pagesA Case Series Describing The Epidemiology and Clinical Characteristics of COVID-19 Infection in Jilin Provinceabeer alrofaeyNo ratings yet
- Nejmoa 2002032Document13 pagesNejmoa 2002032Juan Antonio LópezNo ratings yet
- Effective Treatment of Severe COVID-19 Patients With TocilizumabDocument12 pagesEffective Treatment of Severe COVID-19 Patients With TocilizumabManuel PérezNo ratings yet
- 2019 Novel Coronavirus Disease (COVID-19) in Taiwan: Reports of Two Cases From Wuhan, ChinaDocument4 pages2019 Novel Coronavirus Disease (COVID-19) in Taiwan: Reports of Two Cases From Wuhan, ChinaClaav HugNo ratings yet
- Clinical Characteristics of CoronavirusDocument13 pagesClinical Characteristics of Coronavirusleonardo almeidaNo ratings yet
- Clinical Characteristics of Coronavirus Disease 2019 in ChinaDocument13 pagesClinical Characteristics of Coronavirus Disease 2019 in ChinaprimaNo ratings yet
- 04 OFIDHighdose IVIGasatherapeuticoptionDocument7 pages04 OFIDHighdose IVIGasatherapeuticoptionmy accountNo ratings yet
- Pulmonary Pathology of Early-Phase 2019 Novel Coronavirus (COVID-19) Pneumonia in Two Patients With Lung CancerDocument5 pagesPulmonary Pathology of Early-Phase 2019 Novel Coronavirus (COVID-19) Pneumonia in Two Patients With Lung Cancermuhammad RidoNo ratings yet
- Dysregulation of Immune Response in Patients With COVID-19 in Wuhan, ChinaDocument24 pagesDysregulation of Immune Response in Patients With COVID-19 in Wuhan, ChinaChavdarNo ratings yet
- Research Letters: Co-Infection With Sars-Cov-2 and Influenza A Virus in Patient With Pneumonia, ChinaDocument3 pagesResearch Letters: Co-Infection With Sars-Cov-2 and Influenza A Virus in Patient With Pneumonia, Chinajitesh141No ratings yet
- High-Dose Intravenous Immunoglobulin As A Therapeutic Option For Deteriorating Patients With Coronavirus Disease 2019Document6 pagesHigh-Dose Intravenous Immunoglobulin As A Therapeutic Option For Deteriorating Patients With Coronavirus Disease 2019my accountNo ratings yet
- Edrada2020 Article FirstCOVID-19InfectionsInThePhDocument7 pagesEdrada2020 Article FirstCOVID-19InfectionsInThePhMeryl QuinteroNo ratings yet
- Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, ChinaDocument7 pagesDysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, Chinacika daraNo ratings yet
- MainDocument8 pagesMainWilsonR.CorzoNiñoNo ratings yet
- Estudo DiabetesDocument9 pagesEstudo DiabetesFulano de TalNo ratings yet
- Epidemiologic and Clinical Characteristics of 91 Hospitalized Patients With COVID-19 in Zhejiang, China: A Retrospective, Multi-Centre Case SeriesDocument9 pagesEpidemiologic and Clinical Characteristics of 91 Hospitalized Patients With COVID-19 in Zhejiang, China: A Retrospective, Multi-Centre Case SeriesVeloz RedNo ratings yet
- InternacionalDocument9 pagesInternacionalbryan ronaldNo ratings yet
- Curso Clinico y Factores de RiesgoDocument9 pagesCurso Clinico y Factores de RiesgoEliana TorresNo ratings yet
- 0 - 041 - Early PDFDocument7 pages0 - 041 - Early PDFsome buddyyNo ratings yet
- Covid-19 in South Korea - Challenges of Subclinical ManifestationsDocument2 pagesCovid-19 in South Korea - Challenges of Subclinical ManifestationsSuwandi ChangNo ratings yet
- Value of ICON in CoVid-19 Patients-2Document50 pagesValue of ICON in CoVid-19 Patients-2Mutiara PertiwiNo ratings yet
- 0063JKMS - Jkms 35 E388Document11 pages0063JKMS - Jkms 35 E388Kevin EsquivelNo ratings yet
- Viral Load Kinetics of Sars-Cov-2 Infection in First Two Patients in KoreaDocument7 pagesViral Load Kinetics of Sars-Cov-2 Infection in First Two Patients in KoreaSalvador Tavera MosquedaNo ratings yet
- Clinical Characteristics of Coronavirus Disease 2019 in ChinaDocument13 pagesClinical Characteristics of Coronavirus Disease 2019 in ChinaAzuraa DarmawanNo ratings yet
- Tian Early PhaseDocument12 pagesTian Early PhaseAurelian CârsteaNo ratings yet
- ARTIKELDocument6 pagesARTIKELandi susiloNo ratings yet
- Asymptomatic and Human To Human Transmission of SARS COV 2Document3 pagesAsymptomatic and Human To Human Transmission of SARS COV 2belinda thaniaNo ratings yet
- Clinical Characteristics of Children With Coronavirus Disease 2019 in Hubei, ChinaDocument6 pagesClinical Characteristics of Children With Coronavirus Disease 2019 in Hubei, ChinaBobanBisercicNo ratings yet
- Ciaa242 2 PDFDocument8 pagesCiaa242 2 PDFHesbon MomanyiNo ratings yet
- 1 s2.0 S1473309920300670 Main PDFDocument2 pages1 s2.0 S1473309920300670 Main PDFAdilla Shafryantyo PurnomoNo ratings yet
- TAC COVID 19. LEC-S3-SEM1pdfDocument9 pagesTAC COVID 19. LEC-S3-SEM1pdfJimena Obregon GarciaNo ratings yet
- Clinical Characteristics of Imported Cases of COVID-19 in Jiangsu Province A Multicenter Descriptive StudyDocument23 pagesClinical Characteristics of Imported Cases of COVID-19 in Jiangsu Province A Multicenter Descriptive StudyAna Maria Romero IbagonNo ratings yet
- Fimmu 11 00827Document7 pagesFimmu 11 00827yangxiao9511No ratings yet
- First COVID-19 Infections in The Philippines: A Case Report: Tropical Medicine and HealthDocument7 pagesFirst COVID-19 Infections in The Philippines: A Case Report: Tropical Medicine and HealthTaliNo ratings yet
- Fmed 08 684864Document10 pagesFmed 08 684864nadhia rahdaNo ratings yet
- Tongue Diagnosis and Treatment in Traditional Chinese Medicine For Severe COVID-19: A Case ReportDocument8 pagesTongue Diagnosis and Treatment in Traditional Chinese Medicine For Severe COVID-19: A Case Reportwr48f26rjmNo ratings yet
- DunnoDocument8 pagesDunnoprastiaNo ratings yet
- Clinical Features and Multidisciplinary Treatment Outcome of COVID-19 Pneumonia: A Report of Three CasesDocument8 pagesClinical Features and Multidisciplinary Treatment Outcome of COVID-19 Pneumonia: A Report of Three CasesPutri NoviaNo ratings yet
- Clinical Microbiology and InfectionDocument6 pagesClinical Microbiology and InfectionMiguel AngelNo ratings yet
- Journal Pre-Proof: International Journal of Infectious DiseasesDocument18 pagesJournal Pre-Proof: International Journal of Infectious DiseasesKenya EspinozaNo ratings yet
- Nejmc 2001272Document3 pagesNejmc 2001272Isx HdzNo ratings yet
- ShowimgDocument19 pagesShowimgInayattullah KhamkerNo ratings yet
- About The Author: Research LettersDocument4 pagesAbout The Author: Research LettersSonia Capirosi AyuningtiasNo ratings yet
- Jiang Et Al-2020-Journal of General Internal Medicine1Document6 pagesJiang Et Al-2020-Journal of General Internal Medicine1Farida MurtianiNo ratings yet
- Journal Pre-Proof: Journal of Microbiology, Immunology and InfectionDocument16 pagesJournal Pre-Proof: Journal of Microbiology, Immunology and Infectionbrip selNo ratings yet
- 1.clinical Characteristics of 28 PatientsDocument7 pages1.clinical Characteristics of 28 PatientsTeguh WibowoNo ratings yet
- Guidance for COVID-19: Prevention, Control, Diagnosis and ManagementFrom EverandGuidance for COVID-19: Prevention, Control, Diagnosis and ManagementNo ratings yet
- TransferirDocument15 pagesTransferirigorNo ratings yet
- Industrial Instrumentation-Lec-04Document43 pagesIndustrial Instrumentation-Lec-04Haseeb JatoiNo ratings yet
- Tax Types QuestionsDocument5 pagesTax Types QuestionsJoseph Tinio CruzNo ratings yet
- What Are Fossil FuelsDocument8 pagesWhat Are Fossil Fuels03. Thu AnhNo ratings yet
- Exam AERO3002 2009aprilDocument11 pagesExam AERO3002 2009apriljonthemesNo ratings yet
- A Method For Measuring The Presampled MTF of Digital Radiographic Systems Using An Edge Test DeviceDocument12 pagesA Method For Measuring The Presampled MTF of Digital Radiographic Systems Using An Edge Test DevicetekellamerZ aka tekellamerNo ratings yet
- Soil Cation Exchange Capacity (CEC)Document2 pagesSoil Cation Exchange Capacity (CEC)Ardianto IrsadNo ratings yet
- Body Point CatalogoDocument28 pagesBody Point Catalogojosuevargas17No ratings yet
- 6th Sem Mech Mid Sem Question Bank-1Document14 pages6th Sem Mech Mid Sem Question Bank-1dharmeshNo ratings yet
- Technip3-Petroleum Refining 3 Conversion Processes PDFDocument650 pagesTechnip3-Petroleum Refining 3 Conversion Processes PDFNhat Cao100% (2)
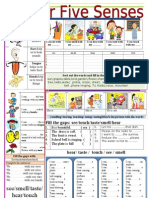
- Five Senses WorksheetDocument1 pageFive Senses WorksheetMauricio MuñozNo ratings yet
- Biggest Wonder of The World 55 63Document9 pagesBiggest Wonder of The World 55 63Leela Kirtaneswari Devi DasiNo ratings yet
- Uv Spectrophotometric Determination of Ranitidine Hydrochloride in Pure and Pharmaceutical FormulationDocument3 pagesUv Spectrophotometric Determination of Ranitidine Hydrochloride in Pure and Pharmaceutical FormulationDaniela PopaNo ratings yet
- Aspire S7-191 Wistron Helium UMADocument103 pagesAspire S7-191 Wistron Helium UMAWieslaw ZadenkoNo ratings yet
- Erp ImplementationsDocument8 pagesErp ImplementationsAJ Nicolas ApostolNo ratings yet
- RVR Meander A Toolbox For Re-Meandering PDFDocument10 pagesRVR Meander A Toolbox For Re-Meandering PDFELINo ratings yet
- Puran c1Document22 pagesPuran c1dennis gamisNo ratings yet
- Schluter Jolly Trim - WallsDocument8 pagesSchluter Jolly Trim - WallsmarkNo ratings yet
- Project Portfolio: A List of Projects Completed by Sukra Helitek and Their BriefsDocument33 pagesProject Portfolio: A List of Projects Completed by Sukra Helitek and Their BriefsDing DongNo ratings yet
- Narrative ReportDocument12 pagesNarrative ReportShaira MukaramNo ratings yet
- US02VABSC02 EnvironmentalStudiesDocument3 pagesUS02VABSC02 EnvironmentalStudiesn5018pNo ratings yet
- Test Bank For Essentials of Contract Law 2nd EditionDocument36 pagesTest Bank For Essentials of Contract Law 2nd Editionstripperinveigle.7m8qg9100% (43)