You might also like
- COVID-19: Impact on Education and BeyondFrom EverandCOVID-19: Impact on Education and BeyondNivedita Das KunduRating: 2 out of 5 stars2/5 (5)
- StrongSchools NC Toolkit 7.29.21 FINAL 1 - 0Document25 pagesStrongSchools NC Toolkit 7.29.21 FINAL 1 - 0judith retanaNo ratings yet
- COVID-19 and Education in Asia and the Pacific: Guidance NoteFrom EverandCOVID-19 and Education in Asia and the Pacific: Guidance NoteNo ratings yet
- StrongSchools NC Toolkit - 1.10.22 v2Document24 pagesStrongSchools NC Toolkit - 1.10.22 v2Curtis CardenNo ratings yet
- Pandemic Preparedness and Response Strategies: COVID-19 Lessons from the Republic of Korea, Thailand, and Viet NamFrom EverandPandemic Preparedness and Response Strategies: COVID-19 Lessons from the Republic of Korea, Thailand, and Viet NamNo ratings yet
- StrongSchools NC Toolkit 12.30.21Document24 pagesStrongSchools NC Toolkit 12.30.21Curtis CardenNo ratings yet
- Public Health Guidance For SchoolsDocument34 pagesPublic Health Guidance For SchoolsNeil StreetNo ratings yet
- Updated ISBE Public Health School GuidanceDocument33 pagesUpdated ISBE Public Health School GuidanceNewsTeam20No ratings yet
- PreK 12 Guidance For Mask Decisions School Districts 02182022 FINALDocument3 pagesPreK 12 Guidance For Mask Decisions School Districts 02182022 FINALHelen BennettNo ratings yet
- Covid Outbreak Guidance For Schools Managing Local Outbreaks v1 003Document4 pagesCovid Outbreak Guidance For Schools Managing Local Outbreaks v1 003Huyteang MengNo ratings yet
- K 12guidance2021 22Document12 pagesK 12guidance2021 22NewsChannel 9No ratings yet
- K-12 COVID RequirementsDocument19 pagesK-12 COVID RequirementsAisley Bryan Gastardo LuceroNo ratings yet
- Roadmap To RecoveryDocument16 pagesRoadmap To RecoveryJeff MorrisNo ratings yet
- School (Prek-12) Guidance: Covid-19: Please Distribute To All Appropriate StaffDocument19 pagesSchool (Prek-12) Guidance: Covid-19: Please Distribute To All Appropriate StaffMaga42No ratings yet
- Guidelines For Childcare Facilities and SchoolsDocument6 pagesGuidelines For Childcare Facilities and SchoolsPrimedia Broadcasting100% (7)
- Background and Context: Updates To DESE COVID-19 GuidanceDocument4 pagesBackground and Context: Updates To DESE COVID-19 Guidancedialynn dwyerNo ratings yet
- 820 105 K12Schools2021 2022Document24 pages820 105 K12Schools2021 2022Joel PanganibanNo ratings yet
- Rhode Island Department of Education: Pre K-12 Health and Safety Guidance For The 2021-2022 School YearDocument10 pagesRhode Island Department of Education: Pre K-12 Health and Safety Guidance For The 2021-2022 School YearNBC 10 WJARNo ratings yet
- Updated School GuidanceDocument13 pagesUpdated School GuidanceWLBT NewsNo ratings yet
- 07.23.2021 MDH MSDE School Childcare GuidanceDocument8 pages07.23.2021 MDH MSDE School Childcare GuidanceChris BerinatoNo ratings yet
- Malinao Lobaton ABM BravoDocument29 pagesMalinao Lobaton ABM Bravoaljon nueva espanaNo ratings yet
- 30 December 2021 NOVA School Leaders LetterDocument2 pages30 December 2021 NOVA School Leaders LetterABC7NewsNo ratings yet
- Protocols For Responding To COVID-19 ScenariosDocument19 pagesProtocols For Responding To COVID-19 ScenariosMike CarraggiNo ratings yet
- Letter To Parents - Statement On Safety Mitigation Measures December 8 2020Document2 pagesLetter To Parents - Statement On Safety Mitigation Measures December 8 2020api-267873540No ratings yet
- MDH and MDE K-12 Planning GuideDocument116 pagesMDH and MDE K-12 Planning GuideDuluth News Tribune100% (1)
- Considerations For School-Related Public Health Measures in The Context of COVID-19Document10 pagesConsiderations For School-Related Public Health Measures in The Context of COVID-19Iova Elena-corinaNo ratings yet
- 8.27.2021 Public Health OrderDocument5 pages8.27.2021 Public Health OrderTrevor DrewNo ratings yet
- Minnesota Fall School Planning Guide - Minnesota Department of HealthDocument16 pagesMinnesota Fall School Planning Guide - Minnesota Department of HealthPatch Minnesota100% (1)
- 01.06.2022 Memo School Childcare GuidanceDocument12 pages01.06.2022 Memo School Childcare GuidanceHolcz DánielNo ratings yet
- Portfolio Reflection 2Document3 pagesPortfolio Reflection 2api-468330934No ratings yet
- Problems EncounteredDocument37 pagesProblems EncounteredMagud, Jemverick Jan Leonard O.No ratings yet
- March 2, 2022 Letter To Mayor Adams, From Public Advocate Jumaane Williams and City Comptroller Brad LanderDocument4 pagesMarch 2, 2022 Letter To Mayor Adams, From Public Advocate Jumaane Williams and City Comptroller Brad LanderJen ChungNo ratings yet
- MINNESOTA SCHOOL COVID PLANNINGDocument24 pagesMINNESOTA SCHOOL COVID PLANNINGThe best gamer 15No ratings yet
- The National Academies PressDocument19 pagesThe National Academies PressTarique MasoodNo ratings yet
- JadeDocument3 pagesJadeGemar BaladiaNo ratings yet
- The Covid-19 Pandemic through Online learning and Lens of education in the Philippines A New NormalDocument12 pagesThe Covid-19 Pandemic through Online learning and Lens of education in the Philippines A New NormalKazuya KinoshitaNo ratings yet
- COVID 19 Vaccine Acceptability Among Public University Students in Bangladesh Highlighting Knowledge Perceptions and AttitudeDocument11 pagesCOVID 19 Vaccine Acceptability Among Public University Students in Bangladesh Highlighting Knowledge Perceptions and AttitudeAkash RahmanNo ratings yet
- 2020-2021 Planning Guide For Schools: Health Considerations For Navigating Covid-19Document19 pages2020-2021 Planning Guide For Schools: Health Considerations For Navigating Covid-19Tony GulliksonNo ratings yet
- PIDSP PPS Position Paper On Optional Masking Indoors in Schools 04nov2022Document3 pagesPIDSP PPS Position Paper On Optional Masking Indoors in Schools 04nov2022Cae OnghansengNo ratings yet
- New Covid FormatDocument30 pagesNew Covid Formatasmahdental1No ratings yet
- 2020-2021 Planning Guide For Schools: Health Considerations For Navigating Covid-19Document23 pages2020-2021 Planning Guide For Schools: Health Considerations For Navigating Covid-19Viens DiviNo ratings yet
- Thesis - Mallari - HOMEBASED-ONLINE-EDUCATION-REVISED FINALDocument113 pagesThesis - Mallari - HOMEBASED-ONLINE-EDUCATION-REVISED FINALJohn Carlo UkolNo ratings yet
- Ed Covid-19 Handbook: Strategies For Safely Reopening Elementary and Secondary SchoolsDocument30 pagesEd Covid-19 Handbook: Strategies For Safely Reopening Elementary and Secondary SchoolsHaidie QuilitNo ratings yet
- Preparing K-12 School Administrators For A Safe Return To School in Fall 2020 - CDCDocument15 pagesPreparing K-12 School Administrators For A Safe Return To School in Fall 2020 - CDCAustin ZilkerNo ratings yet
- 2 Healthcare Preparedness - Edited 4-5-22Document9 pages2 Healthcare Preparedness - Edited 4-5-22Jonathan Jaime GuerreroNo ratings yet
- VDH FAQs For Revised Interim Guidance For The Prevention of COVID-19 in Virginia K12 SchoolsDocument9 pagesVDH FAQs For Revised Interim Guidance For The Prevention of COVID-19 in Virginia K12 SchoolsChuck JacksonNo ratings yet
- SchoolReopening 08.17.21 FINALDocument7 pagesSchoolReopening 08.17.21 FINALNewsChannel 9No ratings yet
- Strict ProtocolsDocument1 pageStrict ProtocolsTemporary GuyNo ratings yet
- Genesee County Health Department 2021-2022 COVID-19 School Toolkit For Schools Without Universal Mask MandatesDocument26 pagesGenesee County Health Department 2021-2022 COVID-19 School Toolkit For Schools Without Universal Mask MandatesCourtney BennettNo ratings yet
- COVID-19 Guidance For Operating Schools Safely 728838 7Document3 pagesCOVID-19 Guidance For Operating Schools Safely 728838 7WXYZ-TV Channel 7 DetroitNo ratings yet
- Lived Experiences ofDocument20 pagesLived Experiences ofImee LabitadNo ratings yet
- SCDPH Mass COVID19 Vaccination PlanDocument32 pagesSCDPH Mass COVID19 Vaccination PlanNewsTeam20100% (1)
- Ii ContentDocument9 pagesIi ContentAyla KristelNo ratings yet
- PROJECT SEYPTI (PPAs) SampleDocument6 pagesPROJECT SEYPTI (PPAs) SampleJenny Vee LlanesNo ratings yet
- The Coronavirus Disease1Document4 pagesThe Coronavirus Disease1Tariro NgocheNo ratings yet
- DEPED DOH JMC No. 01 S. 2021Document27 pagesDEPED DOH JMC No. 01 S. 2021PetRe Biong PamaNo ratings yet
- Supplementary Information On Establishing An Evidence-Based COVID-19 Mitigation PolicyDocument7 pagesSupplementary Information On Establishing An Evidence-Based COVID-19 Mitigation PolicyAna TorresNo ratings yet
- PreK 12 COVID19 Transition Routine Prevention Control 02182022 FINALDocument3 pagesPreK 12 COVID19 Transition Routine Prevention Control 02182022 FINALHelen BennettNo ratings yet
- City of Hickory LawsuitDocument12 pagesCity of Hickory LawsuitCurtis CardenNo ratings yet
- LegislationDocument24 pagesLegislationCurtis CardenNo ratings yet
- Email StatementDocument1 pageEmail StatementCurtis CardenNo ratings yet
- Sycamore Brewing LawsuitDocument11 pagesSycamore Brewing LawsuitCurtis CardenNo ratings yet
- Beech Mountain Incident Reports - RedactedDocument6 pagesBeech Mountain Incident Reports - RedactedCurtis CardenNo ratings yet
- EST StudyDocument13 pagesEST StudyCurtis CardenNo ratings yet
- Union County Joint StatementDocument3 pagesUnion County Joint StatementCurtis CardenNo ratings yet
- House Bill 96 in North CarolinaDocument5 pagesHouse Bill 96 in North CarolinaCurtis CardenNo ratings yet
- Parent Letter Discipline 11.30.21Document1 pageParent Letter Discipline 11.30.21Curtis CardenNo ratings yet
- Ex-CEO From Taylorsville Court DocumentsDocument6 pagesEx-CEO From Taylorsville Court DocumentsCurtis CardenNo ratings yet
- 038 Affected Product LabelsDocument4 pages038 Affected Product LabelsCurtis CardenNo ratings yet
- StrongSchools NC Toolkit 19nov2021Document25 pagesStrongSchools NC Toolkit 19nov2021Curtis CardenNo ratings yet
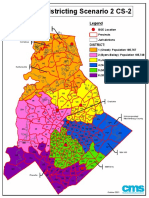
- Scenario 2 - BOE Redistricting CS-2Document1 pageScenario 2 - BOE Redistricting CS-2Curtis CardenNo ratings yet
- Union County Joint ResolutionDocument2 pagesUnion County Joint ResolutionCurtis CardenNo ratings yet
- DrSuttonMessage Nov0421Document2 pagesDrSuttonMessage Nov0421Curtis CardenNo ratings yet
- Message From Dr. Taylor 10.4.21Document1 pageMessage From Dr. Taylor 10.4.21Curtis CardenNo ratings yet
- 4231-5021-7263. Policy W Metric - RevisedDocument2 pages4231-5021-7263. Policy W Metric - RevisedCurtis CardenNo ratings yet
- REVISED BOH Revised Rule Suggested Revisions (Final)Document7 pagesREVISED BOH Revised Rule Suggested Revisions (Final)Curtis CardenNo ratings yet
- James Censure Resolution - 9-28-21Document3 pagesJames Censure Resolution - 9-28-21Curtis CardenNo ratings yet
- Araullo University OB WARD CLASSDocument40 pagesAraullo University OB WARD CLASSAlyza ShamaineNo ratings yet
- CBT Exam To PrintDocument55 pagesCBT Exam To Printdoreen pestanoNo ratings yet
- Menstruation 101: A Guide to Your First Period and Period CareDocument8 pagesMenstruation 101: A Guide to Your First Period and Period CareSheeba StalinNo ratings yet
- LEC 3 Study DesignsDocument44 pagesLEC 3 Study DesignsFaint Faint100% (1)
- Talent ShowDocument3 pagesTalent Showapi-514548596No ratings yet
- Placental Abruption in Term and Preterm.8 PDFDocument8 pagesPlacental Abruption in Term and Preterm.8 PDFMuhammad Riza FahlawiNo ratings yet
- Who Ucn GMP 2023.01 EngDocument447 pagesWho Ucn GMP 2023.01 EngSamantha BudiawanNo ratings yet
- Isolation Quarantine GuidelinesDocument7 pagesIsolation Quarantine GuidelinesDan Ver GawaranNo ratings yet
- CHN DOH ProgramsDocument158 pagesCHN DOH Programsjudd wilson100% (1)
- Full ReportDocument1,081 pagesFull ReportgmcatsupNo ratings yet
- Penilaian Kualitas DietDocument15 pagesPenilaian Kualitas DietWita AdisetyaNo ratings yet
- Vaping in Preganacy A Systematic ReviewDocument8 pagesVaping in Preganacy A Systematic ReviewMia LouwNo ratings yet
- UNICEF DRC - Factsheet On The Situation of Children in DRCDocument2 pagesUNICEF DRC - Factsheet On The Situation of Children in DRCUnicef RdCongoNo ratings yet
- CholeraDocument4 pagesCholeraJoanne Kaye TaylorNo ratings yet
- Physical Examination FormDocument2 pagesPhysical Examination Formapi-665904968No ratings yet
- Clinical Questions and PICO 2012Document18 pagesClinical Questions and PICO 2012Gogularaajan RajendranNo ratings yet
- Menopause Hormone Replacement TherapyDocument4 pagesMenopause Hormone Replacement Therapybidan22No ratings yet
- Background of The StudyDocument5 pagesBackground of The StudyDave PeriaNo ratings yet
- ZODDocument15 pagesZODJudyLynNo ratings yet
- Hep B & C prophylaxis, needle stick injury managementDocument25 pagesHep B & C prophylaxis, needle stick injury managementpoojaNo ratings yet
- Nota Kuliah 4: Kolej Vokasional Batu LanchangDocument8 pagesNota Kuliah 4: Kolej Vokasional Batu LanchangMuhamad Ismail Mohd JamilNo ratings yet
- Comprehensive Abortion Care GuideDocument42 pagesComprehensive Abortion Care GuideKate SantosNo ratings yet
- Class 12 CBSE Investigatory Project On EbolaDocument19 pagesClass 12 CBSE Investigatory Project On EbolaAdriana Dkhar Toi50% (8)
- Interventional Studies 2Document28 pagesInterventional Studies 2Abdul RazzakNo ratings yet
- Germany - DR Thomas Jendges Head of Clinic, Commits SuicideDocument11 pagesGermany - DR Thomas Jendges Head of Clinic, Commits Suicidepepetuel ueksNo ratings yet
- Philippine National Formulary Form For ExemptionDocument3 pagesPhilippine National Formulary Form For ExemptionCO OK-Yim BoholNo ratings yet
- Mandatory VaccinationsDocument7 pagesMandatory Vaccinationsapi-487208181No ratings yet
- Deteksi Keberadaan Bakteri Coliform Pada Depot Air Minum Isi Ulang Di Lingkar Kampus Terpadu Universitas Aisyiyah YogyakartaDocument10 pagesDeteksi Keberadaan Bakteri Coliform Pada Depot Air Minum Isi Ulang Di Lingkar Kampus Terpadu Universitas Aisyiyah YogyakartaVivi AkramNo ratings yet
- Laundry Infection Control ChecklistDocument2 pagesLaundry Infection Control ChecklistSea Gate100% (1)
- Sripal Vaccine CertificateDocument2 pagesSripal Vaccine CertificateGyan Pratap SinghNo ratings yet
- Building a Second Brain: A Proven Method to Organize Your Digital Life and Unlock Your Creative PotentialFrom EverandBuilding a Second Brain: A Proven Method to Organize Your Digital Life and Unlock Your Creative PotentialRating: 4.5 out of 5 stars4.5/5 (238)
- The PARA Method: Simplify, Organize, and Master Your Digital LifeFrom EverandThe PARA Method: Simplify, Organize, and Master Your Digital LifeRating: 4.5 out of 5 stars4.5/5 (3)
- 300+ PMP Practice Questions Aligned with PMBOK 7, Agile Methods, and Key Process Groups - 2024: First EditionFrom Everand300+ PMP Practice Questions Aligned with PMBOK 7, Agile Methods, and Key Process Groups - 2024: First EditionNo ratings yet
- The PARA Method: Simplify, Organize, and Master Your Digital LifeFrom EverandThe PARA Method: Simplify, Organize, and Master Your Digital LifeRating: 5 out of 5 stars5/5 (36)
- Agile: The Insights You Need from Harvard Business ReviewFrom EverandAgile: The Insights You Need from Harvard Business ReviewRating: 4.5 out of 5 stars4.5/5 (34)
- Project Management All-in-One For DummiesFrom EverandProject Management All-in-One For DummiesRating: 5 out of 5 stars5/5 (6)
- Change Management for Beginners: Understanding Change Processes and Actively Shaping ThemFrom EverandChange Management for Beginners: Understanding Change Processes and Actively Shaping ThemRating: 4.5 out of 5 stars4.5/5 (3)
- Managing Time (HBR 20-Minute Manager Series)From EverandManaging Time (HBR 20-Minute Manager Series)Rating: 4.5 out of 5 stars4.5/5 (47)
- The Complete Project Manager: Integrating People, Organizational, and Technical SkillsFrom EverandThe Complete Project Manager: Integrating People, Organizational, and Technical SkillsRating: 5 out of 5 stars5/5 (8)
- PMP Exam Prep: Master the Latest Techniques and Trends with this In-depth Project Management Professional Guide: Study Guide | Real-life PMP Questions and Detailed Explanation | 200+ Questions and AnswersFrom EverandPMP Exam Prep: Master the Latest Techniques and Trends with this In-depth Project Management Professional Guide: Study Guide | Real-life PMP Questions and Detailed Explanation | 200+ Questions and AnswersRating: 5 out of 5 stars5/5 (2)
- High Velocity Innovation: How to Get Your Best Ideas to Market FasterFrom EverandHigh Velocity Innovation: How to Get Your Best Ideas to Market FasterRating: 5 out of 5 stars5/5 (1)
- Harvard Business Review Project Management Handbook: How to Launch, Lead, and Sponsor Successful ProjectsFrom EverandHarvard Business Review Project Management Handbook: How to Launch, Lead, and Sponsor Successful ProjectsRating: 4.5 out of 5 stars4.5/5 (15)
- The Third Wave: An Entrepreneur's Vision of the FutureFrom EverandThe Third Wave: An Entrepreneur's Vision of the FutureRating: 4 out of 5 stars4/5 (63)
- The Myth of Multitasking: How "Doing It All" Gets Nothing DoneFrom EverandThe Myth of Multitasking: How "Doing It All" Gets Nothing DoneRating: 5 out of 5 stars5/5 (1)
- The Unwritten Rules of Managing Up: Project Management Techniques from the TrenchesFrom EverandThe Unwritten Rules of Managing Up: Project Management Techniques from the TrenchesRating: 3.5 out of 5 stars3.5/5 (5)
- Building a Second Brain: A Proven Method to Organize Your Digital Life and Unlock Your Creative PotentialFrom EverandBuilding a Second Brain: A Proven Method to Organize Your Digital Life and Unlock Your Creative PotentialRating: 4 out of 5 stars4/5 (113)
- PMP Exam Prep: How to pass the PMP Exam on your First Attempt – Learn Faster, Retain More and Pass the PMP ExamFrom EverandPMP Exam Prep: How to pass the PMP Exam on your First Attempt – Learn Faster, Retain More and Pass the PMP ExamRating: 4.5 out of 5 stars4.5/5 (3)
- Come Up for Air: How Teams Can Leverage Systems and Tools to Stop Drowning in WorkFrom EverandCome Up for Air: How Teams Can Leverage Systems and Tools to Stop Drowning in WorkRating: 4.5 out of 5 stars4.5/5 (7)
- Summary Guide: Blue Ocean Strategy: How to Create Uncontested Market Space and Make Competition Irrelevant: By W. Chan Kim & Renee Maurborgne | The Mindset Warrior Summary Guide: (Entrepreneurship, Innovation, Product Development, Value Proposition)From EverandSummary Guide: Blue Ocean Strategy: How to Create Uncontested Market Space and Make Competition Irrelevant: By W. Chan Kim & Renee Maurborgne | The Mindset Warrior Summary Guide: (Entrepreneurship, Innovation, Product Development, Value Proposition)Rating: 5 out of 5 stars5/5 (1)
- Crossing the Chasm, 3rd Edition: Marketing and Selling Disruptive Products to Mainstream CustomersFrom EverandCrossing the Chasm, 3rd Edition: Marketing and Selling Disruptive Products to Mainstream CustomersRating: 4.5 out of 5 stars4.5/5 (19)
- The Manager's Path: A Guide for Tech Leaders Navigating Growth and ChangeFrom EverandThe Manager's Path: A Guide for Tech Leaders Navigating Growth and ChangeRating: 4.5 out of 5 stars4.5/5 (99)
- ITIL 4: Digital and IT strategy: Reference and study guideFrom EverandITIL 4: Digital and IT strategy: Reference and study guideRating: 5 out of 5 stars5/5 (1)
- Project Management: The Ultimate Guide for Managing Projects, Productivity, Profits of Enterprises, Startups and Planning with Lean, Scrum, Agile.From EverandProject Management: The Ultimate Guide for Managing Projects, Productivity, Profits of Enterprises, Startups and Planning with Lean, Scrum, Agile.Rating: 4.5 out of 5 stars4.5/5 (3)
- The Red Pill Executive: Transform Operations and Unlock the Potential of Corporate CultureFrom EverandThe Red Pill Executive: Transform Operations and Unlock the Potential of Corporate CultureNo ratings yet