You might also like
- Common Mistakes in Dimensional Calibration MethodsDocument16 pagesCommon Mistakes in Dimensional Calibration MethodssujudNo ratings yet
- Diabetes Mellitus: Dr. Sajid Abbas JaffriDocument37 pagesDiabetes Mellitus: Dr. Sajid Abbas JaffriMaham ZarrinNo ratings yet
- 1992SGSDesignersGuidetoPowerProductsApplicationManual2Ed 1182713547Document1,298 pages1992SGSDesignersGuidetoPowerProductsApplicationManual2Ed 1182713547analog changeNo ratings yet
- Factory made uPVC windows installationDocument2 pagesFactory made uPVC windows installationAmit Singh100% (2)
- Low Blood Sugar: The Nutritional Plan to Overcome Hypoglycaemia, with 60 RecipesFrom EverandLow Blood Sugar: The Nutritional Plan to Overcome Hypoglycaemia, with 60 RecipesNo ratings yet
- How to Manage Diabetes and Cure?: Dr. Alan's Step By Step Guide for Diabetes Management Including General Tips, Diet Plan, Exercise Routine and Much More!From EverandHow to Manage Diabetes and Cure?: Dr. Alan's Step By Step Guide for Diabetes Management Including General Tips, Diet Plan, Exercise Routine and Much More!No ratings yet
- Fire and Blast in The Future OffshoreDocument45 pagesFire and Blast in The Future OffshoredrgNo ratings yet
- HydrotherapyDocument52 pagesHydrotherapyMpt Sports100% (1)
- Diabetes MellitusDocument44 pagesDiabetes MellituslkristinNo ratings yet
- Hearing Aid InformationDocument22 pagesHearing Aid InformationDeepakRodeyNo ratings yet
- Diabetic KetoacidosisDocument12 pagesDiabetic Ketoacidosispolaris_027No ratings yet
- Hero LetterDocument3 pagesHero LetterArunachalam Muthiah0% (1)
- Diabetes ComplicationsDocument29 pagesDiabetes ComplicationsTom ThomasNo ratings yet
- Diabetes Mellitus Study GuideDocument5 pagesDiabetes Mellitus Study Guiderr5633No ratings yet
- Diabetes PresentationDocument32 pagesDiabetes PresentationsgolbariNo ratings yet
- Module 8 Assessment and Management of Patients With DiabetesDocument44 pagesModule 8 Assessment and Management of Patients With DiabetesBlessed GarcianoNo ratings yet
- Proficiency Testbuilder 4th EditionDocument27 pagesProficiency Testbuilder 4th EditionNgan LeNo ratings yet
- Acute Complications of Diabetes: DKA, HONK, HypoglycemiaDocument78 pagesAcute Complications of Diabetes: DKA, HONK, HypoglycemiaSukma WicaturatmashudiNo ratings yet
- Biochemical Basis of Diabetic KetoacidosisDocument21 pagesBiochemical Basis of Diabetic Ketoacidosisdaniyal kumarNo ratings yet
- DKA Diagnosis, Causes, Symptoms and TreatmentDocument11 pagesDKA Diagnosis, Causes, Symptoms and TreatmentAngelyn Bombase100% (1)
- Diabetes Millitus PDFDocument41 pagesDiabetes Millitus PDFAbdullah BhattiNo ratings yet
- Chapter 4 Carbohydrate DisorderDocument26 pagesChapter 4 Carbohydrate DisorderNida RidzuanNo ratings yet
- Classification: LiverDocument20 pagesClassification: LivertermskipopNo ratings yet
- Causes of Metabolic AcidosisDocument10 pagesCauses of Metabolic AcidosisKimberly Anne SP PadillaNo ratings yet
- Diabetes MellitusDocument34 pagesDiabetes MellitusKobby AmoahNo ratings yet
- W02 - Diabetic Emergencies in CCDocument36 pagesW02 - Diabetic Emergencies in CCHelene AlawamiNo ratings yet
- Komplikasi DMDocument7 pagesKomplikasi DMRhima KemalaNo ratings yet
- Pediatric DMDocument39 pagesPediatric DMmy Lord JesusNo ratings yet
- Nursing Care of PT With DiabetesDocument71 pagesNursing Care of PT With DiabetesEricka Lj Robles DimaculanganNo ratings yet
- Lecture - Paediatric Endocrine Emergencies PDFDocument51 pagesLecture - Paediatric Endocrine Emergencies PDFOnSolomonNo ratings yet
- DM Types and FactorsDocument35 pagesDM Types and FactorsIstanli CarrascalNo ratings yet
- Review Notes for Diabetes Mellitus Types, Pathophysiology, Complications & ManagementDocument8 pagesReview Notes for Diabetes Mellitus Types, Pathophysiology, Complications & ManagementEditha LucasNo ratings yet
- Diabetes ketoacidosis: Causes, symptoms, diagnosis and treatmentDocument42 pagesDiabetes ketoacidosis: Causes, symptoms, diagnosis and treatmentfebriNo ratings yet
- Dental Diabetes ManagementDocument30 pagesDental Diabetes ManagementChitrang KolawaleNo ratings yet
- Acute Complications of Diabetes Mellitus Type 2: AnasthasiaDocument25 pagesAcute Complications of Diabetes Mellitus Type 2: AnasthasiaAnasthasia ManaluNo ratings yet
- Diabetes Mellitus: Risks FactorsDocument5 pagesDiabetes Mellitus: Risks FactorsAmer Abdulla SachitNo ratings yet
- Presented By-Kamini SinghDocument52 pagesPresented By-Kamini SinghSupriyati RahayuNo ratings yet
- Diabetes For Dentists: DR Jackie Elliott Clinical Lecturer in DiabetesDocument37 pagesDiabetes For Dentists: DR Jackie Elliott Clinical Lecturer in DiabetesKevalChavdaNo ratings yet
- Module 08 - Endocrine DisordersDocument43 pagesModule 08 - Endocrine DisordersKarina LojaNo ratings yet
- Course Name: Pharmacology Ii Course Code:Shs.314 Credit Hours: 2Hrs Lectures: 20 INSTRUCTOR: Dr. KhurramDocument27 pagesCourse Name: Pharmacology Ii Course Code:Shs.314 Credit Hours: 2Hrs Lectures: 20 INSTRUCTOR: Dr. KhurramAmynah WasimNo ratings yet
- Paper ElektifDocument10 pagesPaper Elektifamyliadwi22No ratings yet
- Clinical Case 2Document13 pagesClinical Case 2Elen De QuirogaNo ratings yet
- Anesthesia and Diabetes: Marwa Ahmad MahrousDocument79 pagesAnesthesia and Diabetes: Marwa Ahmad MahrousAjengNo ratings yet
- Diabetes MellitusDocument24 pagesDiabetes MellitusIgwe SolomonNo ratings yet
- Acute Complications of Diabetes Mellitus: DR Yemane G (MD, Assis. Prof. EMCC)Document63 pagesAcute Complications of Diabetes Mellitus: DR Yemane G (MD, Assis. Prof. EMCC)yared getachewNo ratings yet
- Acute. KetoacidosisdocxDocument12 pagesAcute. KetoacidosisdocxShara SampangNo ratings yet
- 06.disorder of Carbohydrate MetabolismDocument47 pages06.disorder of Carbohydrate MetabolismRizka NizarNo ratings yet
- Diabetes Mellitus: WAHYUDI, S.Farm., AptDocument31 pagesDiabetes Mellitus: WAHYUDI, S.Farm., AptMayesti FransiskaNo ratings yet
- Diabetes Mellitus: - ClassificationDocument22 pagesDiabetes Mellitus: - ClassificationFernando Junior Parra UchasaraNo ratings yet
- Case PresentationDocument6 pagesCase PresentationYrrem UbaganNo ratings yet
- Endocrine - DI, DM I & II 04/13/2016: Review of Endocrine Pancreas: Endocrine and Exocrine Gland Alpha CellsDocument6 pagesEndocrine - DI, DM I & II 04/13/2016: Review of Endocrine Pancreas: Endocrine and Exocrine Gland Alpha Cellsapi-314805004No ratings yet
- GROUP 4 - HyperglikemiDocument5 pagesGROUP 4 - Hyperglikemiamyliadwi22No ratings yet
- Metabolic Disorders Diabetes HandoutDocument21 pagesMetabolic Disorders Diabetes HandoutEdelen GaleNo ratings yet
- Paper Reduction Project Progress Report Doc in White Blue Lines Style - 20240211 - 160421 - ٠٠٠٠Document35 pagesPaper Reduction Project Progress Report Doc in White Blue Lines Style - 20240211 - 160421 - ٠٠٠٠Ryan ReNo ratings yet
- Understanding Diabetes Mellitus TypesDocument27 pagesUnderstanding Diabetes Mellitus TypesÑùmãñ MùghãlNo ratings yet
- New Microsoft Word DocumentDocument6 pagesNew Microsoft Word DocumentKawther El-FikyNo ratings yet
- Diabetic Ketoacidosis: Michele Ritter, M.D. Argy Resident - February, 2007Document18 pagesDiabetic Ketoacidosis: Michele Ritter, M.D. Argy Resident - February, 2007poktaviantiNo ratings yet
- Hyperglycemic Hyperosmolar StateDocument17 pagesHyperglycemic Hyperosmolar StateAqila Mumtaz50% (2)
- Diabetes Mellitus PatientsDocument33 pagesDiabetes Mellitus PatientsShabeel PnNo ratings yet
- Laboratory FindingsDocument22 pagesLaboratory FindingseffiniasiregarNo ratings yet
- DIABETESDocument48 pagesDIABETESالعياده التخصصيه للسكريNo ratings yet
- Dka (Picucourse)Document33 pagesDka (Picucourse)surasuarezlopezNo ratings yet
- Acute Diabetes ComplicationsDocument7 pagesAcute Diabetes ComplicationsHala Salah IbrahimNo ratings yet
- DiabetesDocument81 pagesDiabetesJustin MutuaNo ratings yet
- Farmakoterapi Sistem Endokrin: Tim Dosen Farmasi KlinikDocument42 pagesFarmakoterapi Sistem Endokrin: Tim Dosen Farmasi KlinikAnonymous h76WT2cFdkNo ratings yet
- Soluzioni al Diabete e all'Ipoglicemia - Come prevenire e disfarsene naturalmente e senza medicineFrom EverandSoluzioni al Diabete e all'Ipoglicemia - Come prevenire e disfarsene naturalmente e senza medicineNo ratings yet
- Drug ClassificationDocument1 pageDrug Classificationhasan ismaelNo ratings yet
- CrofelemerDocument1 pageCrofelemerhasan ismaelNo ratings yet
- Newly Approved Medications Name Indication LorcaserinDocument1 pageNewly Approved Medications Name Indication Lorcaserinhasan ismaelNo ratings yet
- BetaquineeDocument1 pageBetaquineehasan ismaelNo ratings yet
- Saudi adverse drug reaction report formDocument2 pagesSaudi adverse drug reaction report formhasan ismaelNo ratings yet
- SFHM-PHR-FRM-064 Adverse Drug Reaction Report Form - Issue 3Document2 pagesSFHM-PHR-FRM-064 Adverse Drug Reaction Report Form - Issue 3hasan ismaelNo ratings yet
- SFHM-PHR-FRM-064 Adverse Drug Reaction Report Form - Issue 3Document2 pagesSFHM-PHR-FRM-064 Adverse Drug Reaction Report Form - Issue 3hasan ismaelNo ratings yet
- Chemical Spill: Quality Round Checklist FormDocument1 pageChemical Spill: Quality Round Checklist Formhasan ismaelNo ratings yet
- Fit For WashingDocument85 pagesFit For WashingIyaka YoeNo ratings yet
- Hook and Eye-Stories Form The MarginsDocument220 pagesHook and Eye-Stories Form The MarginsJefferson LiinNo ratings yet
- Tables in National Plumbing CodeDocument4 pagesTables in National Plumbing CodeMartin GragasinNo ratings yet
- 4 Floral ClockDocument4 pages4 Floral ClockmiguelibasterNo ratings yet
- F0a7c Compal LA-A994p r1.0 2014Document38 pagesF0a7c Compal LA-A994p r1.0 2014DeyProNo ratings yet
- New Patient Needing Continuous Renal Replacement Therapy (CRRT)Document9 pagesNew Patient Needing Continuous Renal Replacement Therapy (CRRT)sergey_1972No ratings yet
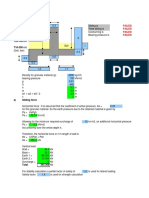
- Design Calculations of Thrust Blocks at Lower Indira: L&T Construction Water & Effluent Treatment ICDocument3 pagesDesign Calculations of Thrust Blocks at Lower Indira: L&T Construction Water & Effluent Treatment IClagnajit dasNo ratings yet
- Learn More: National Weather ServiceDocument2 pagesLearn More: National Weather Servicedamien boyerNo ratings yet
- Pasture FatteningDocument15 pagesPasture FatteningKartika PurnamasariNo ratings yet
- Postmodern EthicsDocument1 pagePostmodern Ethicsgeorge elerickNo ratings yet
- z1875 Caton (BMJ) Electric Currents of The BrainDocument23 pagesz1875 Caton (BMJ) Electric Currents of The BrainUnholy VladNo ratings yet
- Bio Sem2 EssayDocument2 pagesBio Sem2 EssayEileen WongNo ratings yet
- SGDJ PDFDocument334 pagesSGDJ PDFDouglas Rogério de CastroNo ratings yet
- Mobile Network Optimization MapDocument1 pageMobile Network Optimization MapShahzad Farooq100% (1)
- 09 Exp 11 Buffer SolutionsDocument8 pages09 Exp 11 Buffer SolutionsShainmaugne AdvientoNo ratings yet
- Binzel - Katalog MAGDocument64 pagesBinzel - Katalog MAGAdrian KustraNo ratings yet
- History of FlightDocument10 pagesHistory of FlightHanin AlanaziNo ratings yet
- MX 201110 enDocument1,203 pagesMX 201110 envajrahastaNo ratings yet
- Sliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallDocument4 pagesSliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallAbdul Aziz Julkarnain ZulkifliNo ratings yet
- 3 Pipe Mod For Vectra BDocument2 pages3 Pipe Mod For Vectra BEmirhan DöngelNo ratings yet
- Shat Karma ConciseDocument4 pagesShat Karma ConcisesarikaabhayNo ratings yet
- Kyocera Fs-6900 Parts ManualDocument28 pagesKyocera Fs-6900 Parts ManualNic CowpeNo ratings yet