You might also like
- Fatal Invention: How Science, Politics, and Big Business Re-create Race in the Twenty-First CenturyFrom EverandFatal Invention: How Science, Politics, and Big Business Re-create Race in the Twenty-First CenturyRating: 4 out of 5 stars4/5 (23)
- How - Race - Becomes - BiologyDocument11 pagesHow - Race - Becomes - BiologyMinea Merlina Sánchez CrispínNo ratings yet
- Mapping "Race": Critical Approaches to Health Disparities ResearchFrom EverandMapping "Race": Critical Approaches to Health Disparities ResearchNo ratings yet
- Gravlee How Race Becomes BiologyDocument11 pagesGravlee How Race Becomes BiologyzipoliteNo ratings yet
- Structural Competency in Mental Health and Medicine: A Case-Based Approach to Treating the Social Determinants of HealthFrom EverandStructural Competency in Mental Health and Medicine: A Case-Based Approach to Treating the Social Determinants of HealthNo ratings yet
- Gravlee 2009 Racismo AJPADocument11 pagesGravlee 2009 Racismo AJPADominique Gromez BadaloniNo ratings yet
- 2009-Gravlee - How Race Becomes BiologyDocument11 pages2009-Gravlee - How Race Becomes BiologywernerbhNo ratings yet
- Refashioning Race - Dna and The Politics of Health Care. Anne Fausto-SterlingDocument37 pagesRefashioning Race - Dna and The Politics of Health Care. Anne Fausto-SterlingOntologiaNo ratings yet
- 5 Artigo Citado Williams DR (1997) - Raça e SaúdeDocument12 pages5 Artigo Citado Williams DR (1997) - Raça e SaúdePaola BarcellosNo ratings yet
- Biology and IdentityDocument24 pagesBiology and IdentityOntologiaNo ratings yet
- Racial SegregationDocument5 pagesRacial SegregationJames MungaiNo ratings yet
- Race and SocietyDocument17 pagesRace and SocietyJohn Micah MalateNo ratings yet
- Annals of The New York Academy of Sciences - 2010 - Williams - Race Socioeconomic Status and Health ComplexitiesDocument33 pagesAnnals of The New York Academy of Sciences - 2010 - Williams - Race Socioeconomic Status and Health ComplexitiesMahmudul Hasan SakilNo ratings yet
- Topic 5 - Handbook of Medical Sociology Ch4 - 2Document23 pagesTopic 5 - Handbook of Medical Sociology Ch4 - 2AngellaNo ratings yet
- NIH Public Access: Structural Racism and Health InequitiesDocument20 pagesNIH Public Access: Structural Racism and Health Inequitiesbob antonioNo ratings yet
- Everyday Narratives On Race and Health in BrazilDocument21 pagesEveryday Narratives On Race and Health in BrazilMargaret Zelle HariNo ratings yet
- 2009 Article 9079Document5 pages2009 Article 9079Rodrigo BonsaverNo ratings yet
- Final PaperDocument18 pagesFinal Paperapi-548037854No ratings yet
- BiDil As A Case StudyDocument26 pagesBiDil As A Case StudyAli AlmerzaNo ratings yet
- Race-Ethnicity in ResearchDocument32 pagesRace-Ethnicity in ResearchashankarNo ratings yet
- Adler Stewart 2010 - Health Disparities Across The LifespanDocument19 pagesAdler Stewart 2010 - Health Disparities Across The LifespanAndy DewNo ratings yet
- The Cultural Theory and Model of Suicide (2010)Document16 pagesThe Cultural Theory and Model of Suicide (2010)Aulia Kusuma Wardani 'elDhe'No ratings yet
- Karlsen Nazroo 2011 Relation Between Racial Discrimination Social Class and Health Among Ethnic Minority GroupsDocument8 pagesKarlsen Nazroo 2011 Relation Between Racial Discrimination Social Class and Health Among Ethnic Minority GroupslunamadalengoitiafrancoNo ratings yet
- Raza, Etnicidad y RacismoDocument25 pagesRaza, Etnicidad y RacismoJean WolfNo ratings yet
- Hannah VSIethnicityamendedDocument12 pagesHannah VSIethnicityamendedManish Pratap RaghavNo ratings yet
- Van Der Ven Susser 2023 Structural Racism and Risk of SchizophreniaDocument3 pagesVan Der Ven Susser 2023 Structural Racism and Risk of SchizophreniaLink079No ratings yet
- RACE FOR CURES FinalDocument15 pagesRACE FOR CURES FinalJamileBorgesNo ratings yet
- Stem Reaserch Project 2 - 2022 1Document6 pagesStem Reaserch Project 2 - 2022 1api-655430418No ratings yet
- Saperstein, A., & Penner, A. M. (2012) - Racial Fluidity and Inequality in The United StatesDocument53 pagesSaperstein, A., & Penner, A. M. (2012) - Racial Fluidity and Inequality in The United StatesValquiria AlmeidaNo ratings yet
- 2009 - Stephen Ousley - UnderstandingraceandhumanvariationWhyforensicanthr (Retrieved-2015!11!28)Document9 pages2009 - Stephen Ousley - UnderstandingraceandhumanvariationWhyforensicanthr (Retrieved-2015!11!28)Masi SultanNo ratings yet
- Sociology Final PaperDocument11 pagesSociology Final Paperapi-579640700No ratings yet
- Health Care, Race and CultureDocument6 pagesHealth Care, Race and Culturef5kt8ydcqvNo ratings yet
- We Should Abandon "Race" As A Biological Category in Biomedical ResearchDocument2 pagesWe Should Abandon "Race" As A Biological Category in Biomedical ResearchMa. Fer RomeroNo ratings yet
- Fulltext PDFDocument9 pagesFulltext PDFCSilva16No ratings yet
- Burt MedDietDocument12 pagesBurt MedDietVikram KalekaNo ratings yet
- Race and RacismDocument9 pagesRace and RacismKeloka ConsultantsNo ratings yet
- Obesity Research PaperDocument5 pagesObesity Research PaperRyan Washington100% (1)
- Milner, Franz & Braddock (2020)Document6 pagesMilner, Franz & Braddock (2020)ImpRosinNo ratings yet
- Erin Stephens - [Template] Annotated Bibliography (2)Document3 pagesErin Stephens - [Template] Annotated Bibliography (2)n8r2m8bwj4No ratings yet
- 2004 Social Inequality and Depressive Disorders in Bahia, Brazil - Interactions of Gender, Ethnicity, and Social ClassDocument15 pages2004 Social Inequality and Depressive Disorders in Bahia, Brazil - Interactions of Gender, Ethnicity, and Social ClassNaomar Almeida-FilhoNo ratings yet
- Social MobilityDocument10 pagesSocial Mobilitynicholas geamNo ratings yet
- SSM - Population Health: Rourke O'Brien, Tiffany Neman, Nathan Seltzer, Linnea Evans, Atheendar VenkataramaniDocument6 pagesSSM - Population Health: Rourke O'Brien, Tiffany Neman, Nathan Seltzer, Linnea Evans, Atheendar Venkataramanimandeep kaurNo ratings yet
- The Continuing Significance of RaceDocument18 pagesThe Continuing Significance of RaceKakuNo ratings yet
- Psychoneuroendocrinology: A 1 B B BDocument7 pagesPsychoneuroendocrinology: A 1 B B BJuni TaliqueNo ratings yet
- On The Concept of RaceDocument5 pagesOn The Concept of Raceapi-284455138No ratings yet
- Ps. Understanding The Breast Cancer Experience ofDocument28 pagesPs. Understanding The Breast Cancer Experience ofSYLVIA RAMIS ASENJONo ratings yet
- English Language SBA M.FDocument11 pagesEnglish Language SBA M.Fnajairgrant14No ratings yet
- Women ColDocument2 pagesWomen Colrani214No ratings yet
- MigraciónDocument82 pagesMigraciónnoehernandezcortezNo ratings yet
- Ethnic Differences in Eating Disorder Prevalence, Risk Factors, and Predictive Effects of Risk Factors Among Young WomenDocument21 pagesEthnic Differences in Eating Disorder Prevalence, Risk Factors, and Predictive Effects of Risk Factors Among Young WomenCamila CesteroNo ratings yet
- Euthanasia RP 2Document3 pagesEuthanasia RP 2SHIVINo ratings yet
- Euthanasia RP 2Document3 pagesEuthanasia RP 2SHIVINo ratings yet
- Genetic Structure, Self-Identified Race/Ethnicity, and Confounding in Case-Control Association StudiesDocument8 pagesGenetic Structure, Self-Identified Race/Ethnicity, and Confounding in Case-Control Association StudiesFadhilla SetyaNo ratings yet
- How Does RaceDocument4 pagesHow Does Racerodgers wekesaNo ratings yet
- M2-Cola 11Document6 pagesM2-Cola 11ANA MARIA RAPAELA MANDAPNo ratings yet
- Impacts of Racial Discrimination On People's Health and Public Health Systems in Multicultural SocietiesDocument22 pagesImpacts of Racial Discrimination On People's Health and Public Health Systems in Multicultural Societiesmarkoperic2014No ratings yet
- Native American Health Disparities PDFDocument14 pagesNative American Health Disparities PDFShatabdiDas100% (1)
- American J Hum Biol - 2022 - Meloni - A Biosocial Return To Race A Cautionary View For The Postgenomic EraDocument24 pagesAmerican J Hum Biol - 2022 - Meloni - A Biosocial Return To Race A Cautionary View For The Postgenomic EraJosé Pereira da SilvaNo ratings yet
- The Status of The Race Concept in Physical AnthropologyDocument36 pagesThe Status of The Race Concept in Physical AnthropologyVictor RosezNo ratings yet
- 30.08.22 - Article 2 - Ethnic Disparities in Health - The Public's Role in Working For EqualityDocument3 pages30.08.22 - Article 2 - Ethnic Disparities in Health - The Public's Role in Working For EqualityPola PhotographyNo ratings yet
- WGSST FinalDocument2 pagesWGSST FinalMani KamaliNo ratings yet
- Comm 1100 Syllabus PotockiDocument19 pagesComm 1100 Syllabus PotockiMani KamaliNo ratings yet
- 2421 Lab 3Document4 pages2421 Lab 3Mani KamaliNo ratings yet
- Neil Falkner - The Fundamentals of Higher Mathematics-XanEdu (2021)Document191 pagesNeil Falkner - The Fundamentals of Higher Mathematics-XanEdu (2021)Mani KamaliNo ratings yet
- CS 2421 Lab 2Document4 pagesCS 2421 Lab 2Mani KamaliNo ratings yet
- Filing Form Cover Letter: Name To The Attention ofDocument6 pagesFiling Form Cover Letter: Name To The Attention ofMani KamaliNo ratings yet
- Audit - 2022-02-14 - 13 10 15.0 - Mon - Feb - 14 - 17 45 59 - EST - 2022Document5 pagesAudit - 2022-02-14 - 13 10 15.0 - Mon - Feb - 14 - 17 45 59 - EST - 2022Mani KamaliNo ratings yet
- Louis Pasteur and The Hidden WorldDocument144 pagesLouis Pasteur and The Hidden WorldtoniledoNo ratings yet
- Intl Journal of Cancer - 2014 - Lakritz - Beneficial Bacteria Stimulate Host Immune Cells To Counteract Dietary and GeneticDocument12 pagesIntl Journal of Cancer - 2014 - Lakritz - Beneficial Bacteria Stimulate Host Immune Cells To Counteract Dietary and GeneticTrang MốcNo ratings yet
- ICD10 Coding InstructionsDocument55 pagesICD10 Coding Instructionsanton_susanto10No ratings yet
- History of KapanganDocument13 pagesHistory of KapanganLevia May100% (4)
- C Difficile SporesDocument3 pagesC Difficile SporesEda SopNo ratings yet
- Anatomy and Physiology of Adrenal GlandDocument26 pagesAnatomy and Physiology of Adrenal GlandYAMINIPRIYANNo ratings yet
- DSM-IV ADHD Symptom Checklist-Child and Adolescent Version # 6177Document1 pageDSM-IV ADHD Symptom Checklist-Child and Adolescent Version # 6177Chris100% (2)
- Kirk D. Strosahl PHD, Patricia J. Robinson PHD - in This Moment - Five Steps To Transcending Stress Using Mindfulness and Neuroscience (2015, New Harbinger Publications)Document133 pagesKirk D. Strosahl PHD, Patricia J. Robinson PHD - in This Moment - Five Steps To Transcending Stress Using Mindfulness and Neuroscience (2015, New Harbinger Publications)Fábio Vacaro CulauNo ratings yet
- Griffin Binocular AnomaliesDocument599 pagesGriffin Binocular AnomaliesBalder GamaNo ratings yet
- 6 Pap Smear Staining ProeduresDocument26 pages6 Pap Smear Staining Proeduresnguyenvu2412100% (2)
- Ravi Home Tutions: 1 Maek Test 1Document22 pagesRavi Home Tutions: 1 Maek Test 1Silva scary svNo ratings yet
- Diverticular DiseaseDocument15 pagesDiverticular DiseaseRogie SaludoNo ratings yet
- Material Safety Data Sheet: BCA Protein Assay Reagent A, 500 MLDocument6 pagesMaterial Safety Data Sheet: BCA Protein Assay Reagent A, 500 MLCharls DeimoyNo ratings yet
- LEAK REPAIR PROGRAMSDocument2 pagesLEAK REPAIR PROGRAMSPradip GuptaNo ratings yet
- Chemical Fact SheetDocument2 pagesChemical Fact SheetAnonymous dp5b3X1NANo ratings yet
- Recat Medical BoardDocument5 pagesRecat Medical BoardNavara Naveen kumarNo ratings yet
- Cardiology & Ekgs: Archer Nclex ReviewDocument59 pagesCardiology & Ekgs: Archer Nclex Reviewdaphne farleyNo ratings yet
- MeridiansDocument11 pagesMeridiansa2017399883% (6)
- JR Science Quiz 19-20 Class VI - VIIIDocument43 pagesJR Science Quiz 19-20 Class VI - VIIIDAVV IQACNo ratings yet
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- Restorative & Alternative Medicine: Gaurang JoshiDocument1 pageRestorative & Alternative Medicine: Gaurang JoshiKhushi PansuriaNo ratings yet
- Colibacillosis in Poultry A Disease Overview and TDocument14 pagesColibacillosis in Poultry A Disease Overview and TMonik TanNo ratings yet
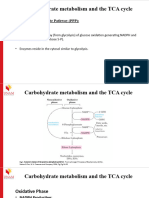
- Carbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Document17 pagesCarbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Frolian MichaelNo ratings yet
- Module 13 Taking Charge of Ones Health 1Document18 pagesModule 13 Taking Charge of Ones Health 1Jandrei Ezekiel LausNo ratings yet
- Animais TransgênicosDocument11 pagesAnimais TransgênicosCleidson OliveiraNo ratings yet
- Veterinary Medicine 7th EditionDocument2 pagesVeterinary Medicine 7th EditionpintuNo ratings yet
- Journal of Traditional and Complementary Medicine: Marhasiyah Rahim, Foong Kiew Ooi, Wan Zuraida Wan Abdul HamidDocument7 pagesJournal of Traditional and Complementary Medicine: Marhasiyah Rahim, Foong Kiew Ooi, Wan Zuraida Wan Abdul HamidKholifatur RohmaNo ratings yet
- Bacteria - Definition, Shapes, Characteristics, Types & ExamplesDocument2 pagesBacteria - Definition, Shapes, Characteristics, Types & ExamplesBaikuntha SabarNo ratings yet
- Rheumatoid Arthritis Drug StudyDocument2 pagesRheumatoid Arthritis Drug StudyChristaNo ratings yet
- Anti Dengue Campaign ProposalDocument2 pagesAnti Dengue Campaign Proposalprithib0% (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (24)
- Nonviolent Communication by Marshall B. Rosenberg - Book Summary: A Language of LifeFrom EverandNonviolent Communication by Marshall B. Rosenberg - Book Summary: A Language of LifeRating: 4.5 out of 5 stars4.5/5 (50)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeNo ratings yet
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)






































![Erin Stephens - [Template] Annotated Bibliography (2)](https://imgv2-1-f.scribdassets.com/img/document/720372381/149x198/2ac584ebff/1712336740?v=1)