You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
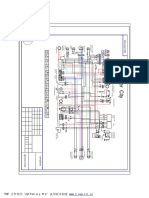
- Cpi Oliver City EldiagramDocument1 pageCpi Oliver City EldiagramHenry BraunNo ratings yet
- The Organic Farmer's Business Handbook by Richard Wiswall (Book Preview)Document26 pagesThe Organic Farmer's Business Handbook by Richard Wiswall (Book Preview)Chelsea Green Publishing100% (65)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- BELLA Automatic Electric Spiralizer Recipe Book PDFDocument28 pagesBELLA Automatic Electric Spiralizer Recipe Book PDFJai's EpicenterNo ratings yet
- Case Control StudyDocument6 pagesCase Control StudyAndre ChundawanNo ratings yet
- 10.4: Eukaryotic Gene RegulationDocument7 pages10.4: Eukaryotic Gene RegulationFlorence Gaone GaongalelweNo ratings yet
- Group 4: Diet For Healthy Teath BonesDocument26 pagesGroup 4: Diet For Healthy Teath Bonesknowledge chanall chanallNo ratings yet
- Ime56350g 2 Felcom15Document51 pagesIme56350g 2 Felcom15SergeyNo ratings yet
- XY Plotter V2.0 Laser Engraver Upgrade Pack User Guide MDraw Version 1.0Document41 pagesXY Plotter V2.0 Laser Engraver Upgrade Pack User Guide MDraw Version 1.0franklinNo ratings yet
- Elastic Compressive-Flexural-Torsional Buckling in Structural MembersDocument36 pagesElastic Compressive-Flexural-Torsional Buckling in Structural MembersArindam SarkarNo ratings yet
- Being and Nothingness The Look SartreDocument3 pagesBeing and Nothingness The Look Sartremaximomore50% (4)
- Sample Course Overview - TemplateDocument2 pagesSample Course Overview - TemplateSingam SridharNo ratings yet
- UntitledDocument2 pagesUntitledSergey ShashminNo ratings yet
- Sandy Point Brochure 2016Document7 pagesSandy Point Brochure 2016miller999No ratings yet
- Introduction To Revit ArchitectureDocument99 pagesIntroduction To Revit ArchitectureOgunwusi Olubodun Samuel100% (1)
- The Thai Spirit House: by Marisa Cranfill YoungDocument2 pagesThe Thai Spirit House: by Marisa Cranfill Youngsian017No ratings yet
- Evap-Lt 60 KV CG ShimaDocument439 pagesEvap-Lt 60 KV CG ShimaDax CasraNo ratings yet
- Clause - 1 FansDocument441 pagesClause - 1 Fansvel mech100% (1)
- Module 2. Classification and Selection of InstrumentsDocument5 pagesModule 2. Classification and Selection of InstrumentsAmit Kr GodaraNo ratings yet
- Matrices Worksheet IDocument2 pagesMatrices Worksheet Icaroline_amideast8101No ratings yet
- Drought Mandals of APDocument20 pagesDrought Mandals of APG Gopala Krishna GudladonaNo ratings yet
- 145kV GTP BPDBDocument4 pages145kV GTP BPDBJRC TestingNo ratings yet
- PHD Thesis Cell CultureDocument5 pagesPHD Thesis Cell Culturefc4qgsp7100% (2)
- Ak95S Error Code ListDocument118 pagesAk95S Error Code ListEnderson Ramos100% (2)
- 1.smart Light, Temperature, Air Condition ControlDocument4 pages1.smart Light, Temperature, Air Condition ControlFatin Nur Syahirah AzharNo ratings yet
- Nasib Ahmad Faqirzada Resume CVDocument4 pagesNasib Ahmad Faqirzada Resume CVNasib Ahmad FaqirzadaNo ratings yet
- Nuccore ResultDocument2,189 pagesNuccore ResultJohanS.Acebedo0% (1)
- Chemistry Revision NotesDocument7 pagesChemistry Revision NotesFarhan RahmanNo ratings yet
- Octavius Tea OfflineDocument7 pagesOctavius Tea Offlineapi-323468541No ratings yet
- Electrix TweakerDocument1 pageElectrix TweakerUSER58679No ratings yet