You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Anatomy of The Coronary Arteries and VeinsDocument80 pagesAnatomy of The Coronary Arteries and Veinstreelife111No ratings yet
- Minimally Invasive ProceduresDocument35 pagesMinimally Invasive ProceduresAlex Pieces100% (2)
- A Toxic Triangle of Destructive Leadership at Bristol Royal InfirmaryDocument19 pagesA Toxic Triangle of Destructive Leadership at Bristol Royal InfirmaryJesicca DeviyantiNo ratings yet
- NAC Protocol PrintableDocument21 pagesNAC Protocol Printablemaadyyy123100% (1)
- Zoloft Sertraline Drug CardDocument1 pageZoloft Sertraline Drug CardSheri490100% (1)
- ملزمة دكتور ضياء التدريب الصيفيDocument128 pagesملزمة دكتور ضياء التدريب الصيفيReyam Sadek95100% (2)
- Atrial Septal Defect (ASD)Document35 pagesAtrial Septal Defect (ASD)Nur Arifah Astri100% (2)
- Lung Cancer (Nursing Care)Document5 pagesLung Cancer (Nursing Care)heiyuNo ratings yet
- Tooth MobilityDocument47 pagesTooth Mobilityc4rm3LNo ratings yet
- Cell Culture Reactor Design FedDocument13 pagesCell Culture Reactor Design Fedyourladys AcostaNo ratings yet
- 10 1016@j Compchemeng 2010 03 010Document9 pages10 1016@j Compchemeng 2010 03 010yourladys AcostaNo ratings yet
- Enzimatic Kinetic Acosta Y. - Altamar R. - Vargas S.Document11 pagesEnzimatic Kinetic Acosta Y. - Altamar R. - Vargas S.yourladys AcostaNo ratings yet
- Building and Environment: F. Yang, X.N. Wu, J.J. Peng, T.S. Ge, Y.J. Dai, R.Z. WangDocument11 pagesBuilding and Environment: F. Yang, X.N. Wu, J.J. Peng, T.S. Ge, Y.J. Dai, R.Z. Wangyourladys AcostaNo ratings yet
- Applied Thermal Engineering: SciencedirectDocument12 pagesApplied Thermal Engineering: Sciencedirectyourladys AcostaNo ratings yet
- Energy Conversion and Management: Latif Aref, Rasoul Fallahzadeh, Vahid Madadi AvarganiDocument12 pagesEnergy Conversion and Management: Latif Aref, Rasoul Fallahzadeh, Vahid Madadi Avarganiyourladys AcostaNo ratings yet
- Effect of Humidification Water On Semi-Dry Flue Gas DesulfurizationDocument6 pagesEffect of Humidification Water On Semi-Dry Flue Gas Desulfurizationyourladys AcostaNo ratings yet
- 2019 BerryDocument15 pages2019 BerrybryaneatscamerasNo ratings yet
- Constipation in ChildrenDocument14 pagesConstipation in ChildrenCarmen OpreaNo ratings yet
- Philippine Dental Association Covid 19 Monitoring FormDocument1 pagePhilippine Dental Association Covid 19 Monitoring Formrhusolano rhusolanoNo ratings yet
- Care For Client With Oxygenation Problem: OutcomesDocument19 pagesCare For Client With Oxygenation Problem: OutcomesPaul JacksonNo ratings yet
- DeltaCut PrimoCut GBDocument8 pagesDeltaCut PrimoCut GBRaj KumarNo ratings yet
- BMJ Avian FluDocument49 pagesBMJ Avian Flualiakbar178No ratings yet
- NCP Pedia WardDocument2 pagesNCP Pedia WardSyrelle GomezNo ratings yet
- 3 Giving Suggestion (About Health)Document7 pages3 Giving Suggestion (About Health)Iryana KusumaNo ratings yet
- Week 1 IntroductionDocument13 pagesWeek 1 Introductionobai AlhwimelNo ratings yet
- Genomic Characterization of Co-Existing Neoplasia and Carcinoma Lesions Reveals Distinct Evolutionary Paths of Gallbladder CancerDocument11 pagesGenomic Characterization of Co-Existing Neoplasia and Carcinoma Lesions Reveals Distinct Evolutionary Paths of Gallbladder CancerleartaNo ratings yet
- Using Myxoma Virus To Understand The Intrinsic Immune Properties of SAMD9 ProteinDocument1 pageUsing Myxoma Virus To Understand The Intrinsic Immune Properties of SAMD9 ProteinJennifer ChenNo ratings yet
- Concept Map MarwahDocument5 pagesConcept Map MarwahAsniah Hadjiadatu AbdullahNo ratings yet
- 2 Jaundice in The NBDocument33 pages2 Jaundice in The NBCheru DugaseNo ratings yet
- Abstracts 2018Document363 pagesAbstracts 2018Osa RafshodiaNo ratings yet
- Cardiac GlycosidesDocument8 pagesCardiac GlycosidesShan Sicat100% (1)
- ATI Flash Cards 03, Medications Affecting Immune SystemDocument40 pagesATI Flash Cards 03, Medications Affecting Immune Systemensoooooooooo0% (1)
- Urinary Tract Infections and Asymptomatic Bacteriuria in Pregnancy - UpToDateDocument20 pagesUrinary Tract Infections and Asymptomatic Bacteriuria in Pregnancy - UpToDateEdward MarteNo ratings yet
- HLTWHS002 PDFDocument4 pagesHLTWHS002 PDFJase Harrison25% (4)
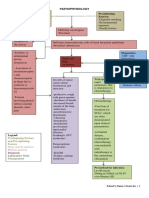
- Pathophysiology Precipitating Factors: Predisposing FactorsDocument2 pagesPathophysiology Precipitating Factors: Predisposing FactorsChristine Pialan SalimbagatNo ratings yet
- Bacterial KeratitisDocument31 pagesBacterial KeratitisMuhammad Rehan SarfrazNo ratings yet
- Endocrine SystemDocument61 pagesEndocrine Systemfanboiitsme20No ratings yet