You might also like
- Background: Alpha ThalassemiaDocument24 pagesBackground: Alpha ThalassemiacristieristiieNo ratings yet
- Thalassaemia: Definition, Classification, Pathogenesis and Complications of This DisorderDocument37 pagesThalassaemia: Definition, Classification, Pathogenesis and Complications of This DisorderSheila MichaelsNo ratings yet
- Hemoglobinopathies (Hemoglobin Disorders)Document18 pagesHemoglobinopathies (Hemoglobin Disorders)Bravan AliennNo ratings yet
- Sickle Cell Disease in PregnancyDocument18 pagesSickle Cell Disease in Pregnancyapi-370504667% (3)
- PB 0783Document9 pagesPB 0783Mona HelouNo ratings yet
- Hemoglobinopathies & Thalasemia Learning ObjectivesDocument10 pagesHemoglobinopathies & Thalasemia Learning ObjectivesFatima AhmedNo ratings yet
- The Significance of The Hemoglobin A2Document18 pagesThe Significance of The Hemoglobin A2Paula MadureuraNo ratings yet
- Hemoglobin SynthesisDocument4 pagesHemoglobin Synthesismadison DeliNo ratings yet
- Talasemia HemoglobinopatiDocument103 pagesTalasemia Hemoglobinopatisanti kristianiNo ratings yet
- Hemoglobin ElectrophoresisDocument22 pagesHemoglobin ElectrophoresisMohamed IbrahimNo ratings yet
- Cme Anemia and ThalassemiaDocument80 pagesCme Anemia and Thalassemianurhadirah94No ratings yet
- HB Bart Fact SheetDocument2 pagesHB Bart Fact Sheetstrawberry pieNo ratings yet
- Detection and Quantitation of Normal and Variant Haemoglobins: An Analytical ReviewDocument15 pagesDetection and Quantitation of Normal and Variant Haemoglobins: An Analytical ReviewAmanda MatthewsNo ratings yet
- Erythrocyte Disorders in The Perinatal Period in AdversePregnancy Outcome and The Fetus:NeonateDocument12 pagesErythrocyte Disorders in The Perinatal Period in AdversePregnancy Outcome and The Fetus:Neonatethanhhien900No ratings yet
- Sickle Cell Anemia and Thalassemias: Paul R. EarlDocument21 pagesSickle Cell Anemia and Thalassemias: Paul R. EarlNavisatul MutmainahNo ratings yet
- Review Article Role Of Xmni Polymorphism In Hbf Induction In Hbe/Β And Β-Thalassaemia PatientsDocument10 pagesReview Article Role Of Xmni Polymorphism In Hbf Induction In Hbe/Β And Β-Thalassaemia PatientsRumana Mahtarin TrishaNo ratings yet
- HB H Disease Clinical Course and DiseaseDocument9 pagesHB H Disease Clinical Course and DiseaseLink BuiNo ratings yet
- Thalasemia MedscapeDocument21 pagesThalasemia MedscapeFenty IswarNo ratings yet
- 02 HemoglobinDocument78 pages02 HemoglobinpixiedustNo ratings yet
- Alpha-Thalassemia Syndromes: From Clinical and Molecular Diagnosis To Bedside ManagementDocument12 pagesAlpha-Thalassemia Syndromes: From Clinical and Molecular Diagnosis To Bedside Managementmayro simanjuntakNo ratings yet
- ThalassemiaDocument44 pagesThalassemiaitsshaswatNo ratings yet
- Alpha-Thalassemia: Authors: Renzo Galanello, MD Antonio Cao, MDDocument31 pagesAlpha-Thalassemia: Authors: Renzo Galanello, MD Antonio Cao, MDKiran KumarNo ratings yet
- Beta-zero (β0) mutations are characterized by the absence of beta-globin production,Document13 pagesBeta-zero (β0) mutations are characterized by the absence of beta-globin production,ririNo ratings yet
- Automated Capillary Electrophoresis in The ScreeningDocument9 pagesAutomated Capillary Electrophoresis in The Screeningsomething privateNo ratings yet
- HemoglobinDocument5 pagesHemoglobinAyioKunNo ratings yet
- B-Talasemias. N Engl J Med 2021.Document17 pagesB-Talasemias. N Engl J Med 2021.VirginiaÁlvarezYepesNo ratings yet
- HemoglobinDocument41 pagesHemoglobinSri Ram 07No ratings yet
- THALASSEMIADocument30 pagesTHALASSEMIAjismi vallachiraNo ratings yet
- Thalassemias: Alissa Martin,, Alexis A. ThompsonDocument9 pagesThalassemias: Alissa Martin,, Alexis A. ThompsonAmada RosalesNo ratings yet
- Alpha Thalassemia Genotyping Deletion by Polymerase Chain ReactionDocument5 pagesAlpha Thalassemia Genotyping Deletion by Polymerase Chain ReactionnadiaNo ratings yet
- ThalassaemiasDocument8 pagesThalassaemiasSalim UddinkhanNo ratings yet
- ThalassaemiasDocument8 pagesThalassaemiasSalim UddinkhanNo ratings yet
- ThalassemiaDocument22 pagesThalassemiaturky hadiNo ratings yet
- HemoglobinopathiesDocument37 pagesHemoglobinopathiesBabak Nami100% (1)
- 4 Genetics DiseaseDocument40 pages4 Genetics Diseasemouid0.2003No ratings yet
- LP 10 Anemia 3Document43 pagesLP 10 Anemia 3Anonymous elq7jZiSNo ratings yet
- Hem AssignmentDocument5 pagesHem Assignmentmalar_km43No ratings yet
- Pages From Download-2Document1 pagePages From Download-2Ra,i Al HaddadNo ratings yet
- Thalassemia and Related HemoglobinopathiesDocument6 pagesThalassemia and Related HemoglobinopathiesMelly SyafridaNo ratings yet
- Thalassaemia: Alpha Thalassaemia Beta Thalassaemia Delta-Beta ThalassaemiaDocument32 pagesThalassaemia: Alpha Thalassaemia Beta Thalassaemia Delta-Beta ThalassaemiaGovindaraju SubramaniNo ratings yet
- Compare and Contrast Alpha & Beta ThalDocument2 pagesCompare and Contrast Alpha & Beta ThalAlison HinesNo ratings yet
- Case Report Haemoglobin Lepore in A Malay Family: A Case ReportDocument5 pagesCase Report Haemoglobin Lepore in A Malay Family: A Case Reportimran ahmed siddiquiNo ratings yet
- Alpha-Thalassemia: Renzo Galanello, MD, and Antonio Cao, MDDocument6 pagesAlpha-Thalassemia: Renzo Galanello, MD, and Antonio Cao, MDLink BuiNo ratings yet
- Int J Lab Hematology - 2013 - Amato - Interpreting Elevated Fetal Hemoglobin in Pathology and Health at The BasicDocument7 pagesInt J Lab Hematology - 2013 - Amato - Interpreting Elevated Fetal Hemoglobin in Pathology and Health at The BasicdrngNo ratings yet
- Session 1 - Pathophysiology and Classification of Thalassemia - Prof. Dr. Manzur MorshedDocument33 pagesSession 1 - Pathophysiology and Classification of Thalassemia - Prof. Dr. Manzur MorshedShahidul Islam ChowdhuryNo ratings yet
- Talasemia Hb-PatiDocument68 pagesTalasemia Hb-PatiNoer HafniNo ratings yet
- Hemoglobinopatzhy PDFDocument16 pagesHemoglobinopatzhy PDFJoy CuanoNo ratings yet
- Talasemias RevisionDocument17 pagesTalasemias Revisionrodolfo venegasNo ratings yet
- Thalassaemias PDFDocument3 pagesThalassaemias PDFNidia100% (1)
- ThalassemiaDocument3 pagesThalassemiaArmandoNo ratings yet
- Alpha ThalassemiaDocument3 pagesAlpha ThalassemiaSravya PangaNo ratings yet
- Study On Hemoglobinopathies and G6PD Deficiency in Terai Districts of NepalDocument30 pagesStudy On Hemoglobinopathies and G6PD Deficiency in Terai Districts of NepalSaroj BhattaraiNo ratings yet
- Hemoglobin ElectrophoresisDocument68 pagesHemoglobin Electrophoresisdrafq2000No ratings yet
- Pages From Download-3Document1 pagePages From Download-3Ra,i Al HaddadNo ratings yet
- Alpha ThalassemiaDocument31 pagesAlpha ThalassemiaBen SabladaNo ratings yet
- Resistencia Genética A La MalariaDocument6 pagesResistencia Genética A La MalariaJuan Diego García sicchaNo ratings yet
- Alpha and Beta ThalassemiaDocument6 pagesAlpha and Beta ThalassemiaSi vis pacem...100% (1)
- HemoglobinopathiesDocument26 pagesHemoglobinopathiesSanjey GaneshNo ratings yet
- A Model for Gene Therapy: Gene Replacement in the Treatment of Sickle Cell Anemia and ThalassemiaFrom EverandA Model for Gene Therapy: Gene Replacement in the Treatment of Sickle Cell Anemia and ThalassemiaNo ratings yet
- Variant Analysis PPT 27.02.2013Document25 pagesVariant Analysis PPT 27.02.2013UMMID WashimNo ratings yet
- VARIANT - HPLC - Retention - Time - As - A - Diagnostic - Tool - For - HemogDocument13 pagesVARIANT - HPLC - Retention - Time - As - A - Diagnostic - Tool - For - HemogUMMID WashimNo ratings yet
- Sop of Interleukin-6 (IL-6) Testing: A.PurposeDocument7 pagesSop of Interleukin-6 (IL-6) Testing: A.PurposeUMMID WashimNo ratings yet
- Sop For Thalassemia Screening Wwith NbsDocument11 pagesSop For Thalassemia Screening Wwith NbsUMMID WashimNo ratings yet
- Project Implementation - Presentation DBT June 2019Document7 pagesProject Implementation - Presentation DBT June 2019UMMID WashimNo ratings yet
- TSH Screen Positive Protocol-SkDocument12 pagesTSH Screen Positive Protocol-SkUMMID WashimNo ratings yet
- Sop of Alkaline PhosphataseDocument6 pagesSop of Alkaline PhosphataseUMMID WashimNo ratings yet
- Sop For Hemoglobin Determination by HPLCDocument13 pagesSop For Hemoglobin Determination by HPLCUMMID WashimNo ratings yet
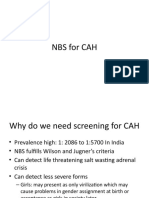
- NBS For CAH-skDocument10 pagesNBS For CAH-skUMMID WashimNo ratings yet
- Abnormal Hemoglobins: General Considerations: History and NomenclatureDocument19 pagesAbnormal Hemoglobins: General Considerations: History and NomenclatureUMMID WashimNo ratings yet
- Beta-Thalassemia: Authors: Antonio Cao, MD Renzo Galanello, MDDocument33 pagesBeta-Thalassemia: Authors: Antonio Cao, MD Renzo Galanello, MDUMMID WashimNo ratings yet
- HemoglobinopathiesDocument57 pagesHemoglobinopathiesdrafq2000100% (1)
- NBS - SOP - Galactosemia, BiotinidaseDocument13 pagesNBS - SOP - Galactosemia, BiotinidaseUMMID WashimNo ratings yet
- Problems With The Management of The Golden Apple Snail Pomacea Canaliculata: An Important Exotic Pest of Rice in AsiaDocument2 pagesProblems With The Management of The Golden Apple Snail Pomacea Canaliculata: An Important Exotic Pest of Rice in AsiaGerryanna MagbitangNo ratings yet
- Guideline For Prevention of Surgical Wound InfectionsDocument14 pagesGuideline For Prevention of Surgical Wound InfectionsosaqerNo ratings yet
- Anti Nutritional Factors in Feedstuff For Poultry (15-10-2019)Document19 pagesAnti Nutritional Factors in Feedstuff For Poultry (15-10-2019)Munir ullahNo ratings yet
- Todays SPSC Municipal Officer Comprehensive Soved Paper (28 May 2023)Document12 pagesTodays SPSC Municipal Officer Comprehensive Soved Paper (28 May 2023)Muhammad Mubeen SolangiNo ratings yet
- Eosinophilic DermatosesDocument15 pagesEosinophilic DermatosesmikelNo ratings yet
- Fennel CultivationDocument10 pagesFennel CultivationKannanRamamirthumNo ratings yet
- Talasemia de HB S y Talasemia de HB CDocument10 pagesTalasemia de HB S y Talasemia de HB CAlejandra NúñezNo ratings yet
- Endokrinologi - Kanker ProstatDocument11 pagesEndokrinologi - Kanker ProstatPutri Mustika SariNo ratings yet
- Chapter 1 Nutrition and MetabolismDocument19 pagesChapter 1 Nutrition and Metabolismbayan.grNo ratings yet
- Cactus Explorer 09 - Complete PDFDocument56 pagesCactus Explorer 09 - Complete PDFkhun sakNo ratings yet
- Invasive Species AssignmentDocument4 pagesInvasive Species AssignmentAmanda ChristineNo ratings yet
- Plant Diversity and Ethnobotany in Berehet District, North Shewa Zone of Amhara Region (Ethiopia) With Emphasis On Wild Edible PlantsDocument13 pagesPlant Diversity and Ethnobotany in Berehet District, North Shewa Zone of Amhara Region (Ethiopia) With Emphasis On Wild Edible Plantstrradhikashirke5583No ratings yet
- 27 Concepts of Growth and Development EditedDocument78 pages27 Concepts of Growth and Development Editedjaroh_20100% (4)
- ABO-Rh Blood Typing With Synthetic Blood: Teacher'S Manual and Student GuideDocument32 pagesABO-Rh Blood Typing With Synthetic Blood: Teacher'S Manual and Student GuideMylan Gaston100% (1)
- Calvin Lecture PDFDocument27 pagesCalvin Lecture PDFNaomi ElliotNo ratings yet
- S5LT-IIc-3.3.1-THE MENSTRUAL CYCLE PDFDocument5 pagesS5LT-IIc-3.3.1-THE MENSTRUAL CYCLE PDFMelyn BustamanteNo ratings yet
- 2024 Microbiology Hons Booklet - FINALDocument54 pages2024 Microbiology Hons Booklet - FINALchand198No ratings yet
- Contraceptive Physiology: by Dr.M.Anthony David MD Professor of PhysiologyDocument44 pagesContraceptive Physiology: by Dr.M.Anthony David MD Professor of PhysiologyFlavius AnghelNo ratings yet
- Evidence of Evolution PacketDocument8 pagesEvidence of Evolution PacketBeckett DeMossNo ratings yet
- Cellular REspiration Virtual Lab Snails and ElodeaDocument4 pagesCellular REspiration Virtual Lab Snails and Elodeasheisbonjing PHNo ratings yet
- How Do The Parts of The Integumentary System Work?: LessonDocument4 pagesHow Do The Parts of The Integumentary System Work?: LessonSyrill EsperoNo ratings yet
- Karin Knisely - A Student Handbook For Writing in BiologyDocument490 pagesKarin Knisely - A Student Handbook For Writing in BiologyHaley N67% (6)
- Anatomy MCQsDocument26 pagesAnatomy MCQsMuhammadsiddique khanNo ratings yet
- Mineral and Vitamin Interaction ChartDocument1 pageMineral and Vitamin Interaction ChartDrRameem BlochNo ratings yet
- Allegan County 23 November 2014 W14-267 ANTHRO - Final-SignedDocument4 pagesAllegan County 23 November 2014 W14-267 ANTHRO - Final-SignedFergus BurnsNo ratings yet
- Lab ReportDocument7 pagesLab ReportJade PategaNo ratings yet
- Volume 21 Opt Compressed ADocument205 pagesVolume 21 Opt Compressed AJeff TaylorNo ratings yet
- Postdoctoral Fellow in NeurochemistryDocument4 pagesPostdoctoral Fellow in Neurochemistrysaudagar_minang72No ratings yet
- Principles Of: BiochemistryDocument52 pagesPrinciples Of: BiochemistryShaden MasriNo ratings yet
- Durex Sexting EguideDocument9 pagesDurex Sexting EguidesciceptNo ratings yet