You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Hardness TestDocument20 pagesHardness TestJake Tee Hon YiNo ratings yet
- Sanyo Denki TapeReader Model 2702 Instruction ManualDocument18 pagesSanyo Denki TapeReader Model 2702 Instruction ManualcoronaqcNo ratings yet
- Drives: AC Inverters Sensorless Vector Closed Loop Vector Servo Drives DC Drives MotorsDocument44 pagesDrives: AC Inverters Sensorless Vector Closed Loop Vector Servo Drives DC Drives Motorsjohxav10No ratings yet
- Tedtalks: Malcolm Gladwell: The Strange Tale of The Norden BombsightDocument9 pagesTedtalks: Malcolm Gladwell: The Strange Tale of The Norden BombsightalibrownNo ratings yet
- DoubleTakeAvailabilityLinuxUsersGuide 7.1.2Document302 pagesDoubleTakeAvailabilityLinuxUsersGuide 7.1.2ZainalNo ratings yet
- Work ImmersionDocument12 pagesWork ImmersionGerald TamondongNo ratings yet
- MA 103 SlidesDocument11 pagesMA 103 SlidessarisNo ratings yet
- Blood SpatterDocument13 pagesBlood SpatterGabriel Stossel (2020)No ratings yet
- Magnetic Force Analysis in A Gapped-Core Reactor Model Under Harmonic Magnetizations by Efficient Frequency-Domain DecompositionDocument2 pagesMagnetic Force Analysis in A Gapped-Core Reactor Model Under Harmonic Magnetizations by Efficient Frequency-Domain DecompositionKiran KarthikNo ratings yet
- DB2 Security: Sample QuestionsDocument3 pagesDB2 Security: Sample Questionspraveen123jNo ratings yet
- Three Moment Equation For BeamsDocument12 pagesThree Moment Equation For BeamsRico EstevaNo ratings yet
- Smith - Matthew, ResumeDocument1 pageSmith - Matthew, Resumesmithm13No ratings yet
- A Comparison of Australian and German Literary JournalismDocument262 pagesA Comparison of Australian and German Literary JournalismKatarina TešićNo ratings yet
- Research PaperDocument20 pagesResearch PaperAngel Candare76% (21)
- CPCCCM2007B Student Final Assessment Submission EvidenceDocument36 pagesCPCCCM2007B Student Final Assessment Submission Evidencemishal chNo ratings yet
- ENGL 0101 Graded Quiz Unit 6Document3 pagesENGL 0101 Graded Quiz Unit 6Mark AntonyNo ratings yet
- Fiber Cable Preparation, Splicing, and Termination InstructionsDocument8 pagesFiber Cable Preparation, Splicing, and Termination InstructionsHunaAdjaganNo ratings yet
- 11 Anh INTENSIVE LISTENING LESSON 01.12Document2 pages11 Anh INTENSIVE LISTENING LESSON 01.12Ha Huy KhanhNo ratings yet
- Almighty Military Format Revised by Welbeck (Male)Document11 pagesAlmighty Military Format Revised by Welbeck (Male)jadenroy442No ratings yet
- First Periodical Test 2022-2023Document4 pagesFirst Periodical Test 2022-2023RHYSLYN RUFIN SALINASNo ratings yet
- C Guide ExamDocument724 pagesC Guide ExamAlan MirandaNo ratings yet
- Determinants of Organizational StructureDocument57 pagesDeterminants of Organizational StructureAmit89% (9)
- Gas Dynamics and Jet PropulsionDocument315 pagesGas Dynamics and Jet PropulsionSuresh BiradarNo ratings yet
- The Six Steps of The Writing ProcessDocument4 pagesThe Six Steps of The Writing ProcessBenjamín Fernando Rodriguez Santana67% (3)
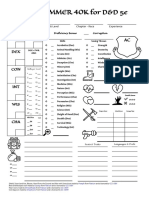
- WARHAMMER 40K For D&D 5e: Character Name Class & Level Chapter - Race ExperienceDocument1 pageWARHAMMER 40K For D&D 5e: Character Name Class & Level Chapter - Race ExperienceJacob CooperNo ratings yet
- Verification OverviewDocument123 pagesVerification OverviewSamNo ratings yet
- ECP2046 CO2 Tri 2 20122013Document6 pagesECP2046 CO2 Tri 2 20122013Engr Ayaz KhanNo ratings yet
- Jutoh PlusDocument34 pagesJutoh Plusrenio75No ratings yet
- The 14 Tablets of Lord EnkiDocument10 pagesThe 14 Tablets of Lord EnkiChirita GheorgheNo ratings yet
- Ab PLC EpksDocument82 pagesAb PLC EpksBouazzaNo ratings yet