You might also like
- Occupational Stress, Job Satisfaction, Mental Health, Adolescents, Depression and the Professionalisation of Social WorkFrom EverandOccupational Stress, Job Satisfaction, Mental Health, Adolescents, Depression and the Professionalisation of Social WorkNo ratings yet
- Healthcare 11 01792 v2Document19 pagesHealthcare 11 01792 v2Adiyanto DidietNo ratings yet
- The Impact of Workplace Environment That Affect Employee's Performance in Private Hospitals of Hyderabad, PakistanDocument6 pagesThe Impact of Workplace Environment That Affect Employee's Performance in Private Hospitals of Hyderabad, PakistanNasir BashirNo ratings yet
- Conceptualizing The Dynamics of Workplace Stress ADocument11 pagesConceptualizing The Dynamics of Workplace Stress ACassia MontiNo ratings yet
- Jsju 2 - Workload Stress ExhaustionDocument15 pagesJsju 2 - Workload Stress ExhaustionBasilius Redan WerangNo ratings yet
- Causes and Prevention of Occupational Stress: ArticleDocument76 pagesCauses and Prevention of Occupational Stress: ArticleDumitrița IachimovschiNo ratings yet
- Ijerph 19 05792Document15 pagesIjerph 19 05792zharifderisNo ratings yet
- 2009 ImprovingworkenvironmentsDocument11 pages2009 ImprovingworkenvironmentsMarta GonçalvesNo ratings yet
- Stress Berdasarkan Masa KerjaDocument7 pagesStress Berdasarkan Masa Kerjasiti halimahNo ratings yet
- JobsatisfactionDocument10 pagesJobsatisfactionJudeNo ratings yet
- Effect of Workplace Stress Management Strategies On Employees' EfficiencyDocument7 pagesEffect of Workplace Stress Management Strategies On Employees' EfficiencyMohammad Al-arrabi AldhidiNo ratings yet
- 10 5923 J Ijap 20221201 03Document7 pages10 5923 J Ijap 20221201 03ayachairi5No ratings yet
- Correlation Between Employee Performance Well-BeinDocument14 pagesCorrelation Between Employee Performance Well-BeinLawal CafeNo ratings yet
- ARTICULO - How Job Stress Influences Job Performance - 2019Document11 pagesARTICULO - How Job Stress Influences Job Performance - 2019Farmaceutico RaulNo ratings yet
- MRK - Spring 2022 - PAD619 - 8 - MC190400105Document20 pagesMRK - Spring 2022 - PAD619 - 8 - MC190400105Rehman KhanNo ratings yet
- Impact of Job Stress On EmployeesDocument11 pagesImpact of Job Stress On EmployeesTimmie Issa Bae100% (1)
- Work-Related Stress and Health-Risks, Mechanisms and CountermeasuresDocument9 pagesWork-Related Stress and Health-Risks, Mechanisms and CountermeasuresMetiku DigieNo ratings yet
- Occupational Stress in Physical Therapist Working As Clinician and Academician in Lahore (A Comparative Cross Sectional Study)Document5 pagesOccupational Stress in Physical Therapist Working As Clinician and Academician in Lahore (A Comparative Cross Sectional Study)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Workplace-Based Organizational Interventions Promoting Mental Health and Happiness Among Healthcare Workers: A Realist ReviewDocument22 pagesWorkplace-Based Organizational Interventions Promoting Mental Health and Happiness Among Healthcare Workers: A Realist ReviewOnes Salvo TirtoNo ratings yet
- Kqy 111Document2 pagesKqy 111rygsstNo ratings yet
- Welfare and SafetyDocument8 pagesWelfare and Safetyரவிக்குமார் பகுத்தறிவாளன்No ratings yet
- Exploring The Impact of Resilience, Self-Efficacy, Optimism and Organizational Resources On Work Engagement.Document11 pagesExploring The Impact of Resilience, Self-Efficacy, Optimism and Organizational Resources On Work Engagement.Charmaine ShaninaNo ratings yet
- 1 s2.0 S2772501421000014 MainDocument6 pages1 s2.0 S2772501421000014 Mainfosimmik.undipNo ratings yet
- Health Behaviors of University Office Workers and Ergonomic SolutionsDocument7 pagesHealth Behaviors of University Office Workers and Ergonomic SolutionsAlin MartinNo ratings yet
- s40359 019 0349 1Document16 pagess40359 019 0349 1viviemoetNo ratings yet
- Oamjms 9e 7270 20211115 v0 CorrectedDocument9 pagesOamjms 9e 7270 20211115 v0 CorrectedClaudia MoksidyNo ratings yet
- Article On Stress ManagementDocument10 pagesArticle On Stress ManagementSharmila AshrafNo ratings yet
- Stress Management With Special Reference To Public Sector Bank Employees in ChennaiDocument6 pagesStress Management With Special Reference To Public Sector Bank Employees in ChennaiPriya KuttyNo ratings yet
- KQW 155Document6 pagesKQW 155Al FatihNo ratings yet
- Sorensen 2018Document36 pagesSorensen 2018munira althukairNo ratings yet
- Bazarko 2013Document28 pagesBazarko 2013pspamNo ratings yet
- Impact of Stress On Employee Productivit PDFDocument10 pagesImpact of Stress On Employee Productivit PDFdiahNo ratings yet
- JurnalDocument14 pagesJurnalmairina yulistianiNo ratings yet
- Impact of Stress On Employee Productivity, Performance and Turnover An Important Managerial IssueDocument9 pagesImpact of Stress On Employee Productivity, Performance and Turnover An Important Managerial Issueimamashraf123100% (1)
- Eportfolio Solutions PaperDocument4 pagesEportfolio Solutions Paperapi-724088039No ratings yet
- Chapter One 1.1 Background To The StudyDocument61 pagesChapter One 1.1 Background To The StudyTAOHEEDNo ratings yet
- Safety and Health at Work: Matteo Ronchetti, Simone Russo, Cristina Di Tecco, Sergio IavicoliDocument7 pagesSafety and Health at Work: Matteo Ronchetti, Simone Russo, Cristina Di Tecco, Sergio IavicoliGean Pablo MendozaNo ratings yet
- Study On Stress Management Among Co-Operative Bank Employees in Malappuram DistrictDocument10 pagesStudy On Stress Management Among Co-Operative Bank Employees in Malappuram DistrictKMA JALEELNo ratings yet
- Stress Management With Special Reference To Public Sector Bank Employees in ChennaiDocument6 pagesStress Management With Special Reference To Public Sector Bank Employees in ChennairockingprashantNo ratings yet
- Organisational Commitment in Healthcare Systems: A Bibliometric AnalysisDocument21 pagesOrganisational Commitment in Healthcare Systems: A Bibliometric AnalysisDr. POONAM KAUSHALNo ratings yet
- PDFDocument15 pagesPDFKarine SchmidtNo ratings yet
- 38.subha With Cover Page v2Document11 pages38.subha With Cover Page v2ABDUL KARIM ASLAMINo ratings yet
- Organisational Design, Organisational Climate and Burnouts in Health Services CompaniesDocument19 pagesOrganisational Design, Organisational Climate and Burnouts in Health Services CompaniesJohnNo ratings yet
- Universitas Mataram: Jurnal Magister Manajemen VOL. 6 No. 1 MARET 2017Document18 pagesUniversitas Mataram: Jurnal Magister Manajemen VOL. 6 No. 1 MARET 2017Muh.Zulfikar KamaruddinNo ratings yet
- Paper Work Seminar Group 6Document35 pagesPaper Work Seminar Group 6api-561774894No ratings yet
- 1Document10 pages1Unaiza KhanNo ratings yet
- Wellness ProgramDocument23 pagesWellness Programasde100% (1)
- Ações Educacionais e Promoção de Saúde para Gestores - Revisão de LiteraturaDocument10 pagesAções Educacionais e Promoção de Saúde para Gestores - Revisão de LiteraturaRodrigo MartinsNo ratings yet
- What Are The Workplace Health Strategies Which Can Be Implemented To Improve Employee Job PerformanceDocument3 pagesWhat Are The Workplace Health Strategies Which Can Be Implemented To Improve Employee Job PerformanceRobert Maxwell OukoNo ratings yet
- The Influence of Job Stress On JobDocument6 pagesThe Influence of Job Stress On JobInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Work Environment Affects Patient Safety Climate in A Government HospitalDocument7 pagesWork Environment Affects Patient Safety Climate in A Government HospitalIJPHSNo ratings yet
- Research Proposal On The Effects of Motivation On Employee ProductivityDocument6 pagesResearch Proposal On The Effects of Motivation On Employee ProductivityDotto MayaulaNo ratings yet
- Coping - Strategies - Adopted - by - Nurses - and Midwives To Mitigate The Effects of Occupational StressDocument8 pagesCoping - Strategies - Adopted - by - Nurses - and Midwives To Mitigate The Effects of Occupational StressMiezah ElliasonNo ratings yet
- Organizational and Environmental Factors That Affect Worker Health and Safety and Patient OutcomesDocument14 pagesOrganizational and Environmental Factors That Affect Worker Health and Safety and Patient OutcomesBheru LalNo ratings yet
- Ijerph 20 03685Document14 pagesIjerph 20 03685Tuhin DeyNo ratings yet
- Stress Assessment and Research Toolkit (StART)Document11 pagesStress Assessment and Research Toolkit (StART)Dr-Chufo IzquierdoNo ratings yet
- JETIR1908A66Document7 pagesJETIR1908A66Harsha VarshuNo ratings yet
- Falno PDFDocument18 pagesFalno PDFmUZANo ratings yet
- The Role of Workplace Health Promotion in Addressing Job StressDocument8 pagesThe Role of Workplace Health Promotion in Addressing Job StressSvetlana AndjelkovićNo ratings yet
- Elo 1998Document8 pagesElo 1998Bejan ElenaNo ratings yet
- Controllable vs. Uncontrollable Factors of Employee Turnover Intentions: An EmpiricalDocument21 pagesControllable vs. Uncontrollable Factors of Employee Turnover Intentions: An Empiricalimifty75% (4)
- ReportDocument59 pagesReportAnkit KhokharNo ratings yet
- Work Stress Issues in Malaysia: January 2009Document15 pagesWork Stress Issues in Malaysia: January 2009Fakhrul IslamNo ratings yet
- Chapter 2Document7 pagesChapter 2Christine Mae Viñas RemoNo ratings yet
- Assignment 1 - Introduction To Counselling & Guidance (Group 5)Document25 pagesAssignment 1 - Introduction To Counselling & Guidance (Group 5)fiqah fiqahNo ratings yet
- Work-Related Stress in NursingDocument49 pagesWork-Related Stress in Nursinga_l_y_nNo ratings yet
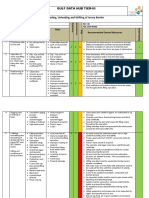
- RAMS-Loading, Unloading and Shifting of MaterialDocument5 pagesRAMS-Loading, Unloading and Shifting of MaterialEm Niax50% (2)
- Managing Individual Differences and BehaviorDocument40 pagesManaging Individual Differences and BehaviorDyg Norjuliani100% (1)
- Chap 1 Organizational Change and Stress ManagementDocument22 pagesChap 1 Organizational Change and Stress ManagementMuhammad Hashim Memon75% (4)
- Sheila Menon - London College of Clinical Hypnosis AsiaDocument16 pagesSheila Menon - London College of Clinical Hypnosis AsiaakubestlahNo ratings yet
- Dr. Shazia PaperDocument4 pagesDr. Shazia PaperMominah MayamNo ratings yet
- Burnout Among PsychoterapistsDocument26 pagesBurnout Among PsychoterapistsGsus Calle FernandezNo ratings yet
- Topic 5Document41 pagesTopic 5Nurul FarhanahNo ratings yet
- Mental Health in The WorkplaceDocument54 pagesMental Health in The Workplacearlene pagar100% (2)
- Running Head: Amazon Case Analysis 1Document30 pagesRunning Head: Amazon Case Analysis 1Ahmed HadadNo ratings yet
- Aguiar-Quintana Et Al., 2021Document10 pagesAguiar-Quintana Et Al., 2021Singa MerahNo ratings yet
- Coping Behaviours and Teacher BurnoutDocument13 pagesCoping Behaviours and Teacher BurnoutNotafake NameatallNo ratings yet
- Employers Guide - InteractiveDocument24 pagesEmployers Guide - Interactiveapi-285398586No ratings yet
- HSC PlanDocument12 pagesHSC PlanSanjay SahooNo ratings yet
- Foreign Studies and Foreign Literature About Stress and Sources of StressDocument11 pagesForeign Studies and Foreign Literature About Stress and Sources of StressBrien Naco50% (12)
- Building More Effective Organizations - HR Management and Performance in Practice (2008)Document413 pagesBuilding More Effective Organizations - HR Management and Performance in Practice (2008)Sara KožićNo ratings yet
- Causes and Effects of Work Stress in Organization (Vikrant Baghi)Document16 pagesCauses and Effects of Work Stress in Organization (Vikrant Baghi)Vikrant Baghi71% (7)
- Work. (7: BooksDocument9 pagesWork. (7: Bookssilentassassin_23No ratings yet
- ILO (Prevention of Occupational Disease)Document14 pagesILO (Prevention of Occupational Disease)Yopa Riyanda PuteriNo ratings yet
- Ulrich Borgren Gardiner Lundin 2018Document15 pagesUlrich Borgren Gardiner Lundin 2018Amy VegaNo ratings yet
- Mere WaliDocument7 pagesMere WaliMaliCk TaimoorNo ratings yet
- Effects of Job Stress On Employees PerformanceDocument9 pagesEffects of Job Stress On Employees PerformanceMOHD. SHADABNo ratings yet
- A Study On Employee Absenteeism at Transport CorporationDocument6 pagesA Study On Employee Absenteeism at Transport Corporationvenkates007100% (1)
- Relax From Job, Don't Feel Stress! The Detrimental Effects of Job Stress andDocument10 pagesRelax From Job, Don't Feel Stress! The Detrimental Effects of Job Stress andKKN-T REGULER PERIODE II KELOMPOK 109 SEI KAYU 1No ratings yet
- Stress 2Document98 pagesStress 2MadMaxNo ratings yet
- Summary of Zero to One: Notes on Startups, or How to Build the FutureFrom EverandSummary of Zero to One: Notes on Startups, or How to Build the FutureRating: 4.5 out of 5 stars4.5/5 (100)
- ChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveFrom EverandChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveNo ratings yet
- 24 Assets: Create a digital, scalable, valuable and fun business that will thrive in a fast changing worldFrom Everand24 Assets: Create a digital, scalable, valuable and fun business that will thrive in a fast changing worldRating: 5 out of 5 stars5/5 (20)
- The Millionaire Fastlane: Crack the Code to Wealth and Live Rich for a LifetimeFrom EverandThe Millionaire Fastlane: Crack the Code to Wealth and Live Rich for a LifetimeRating: 4.5 out of 5 stars4.5/5 (58)
- 12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure EntrepreneurFrom Everand12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure EntrepreneurRating: 4 out of 5 stars4/5 (2)
- The Millionaire Fastlane, 10th Anniversary Edition: Crack the Code to Wealth and Live Rich for a LifetimeFrom EverandThe Millionaire Fastlane, 10th Anniversary Edition: Crack the Code to Wealth and Live Rich for a LifetimeRating: 4.5 out of 5 stars4.5/5 (88)
- To Pixar and Beyond: My Unlikely Journey with Steve Jobs to Make Entertainment HistoryFrom EverandTo Pixar and Beyond: My Unlikely Journey with Steve Jobs to Make Entertainment HistoryRating: 4 out of 5 stars4/5 (26)
- The Master Key System: 28 Parts, Questions and AnswersFrom EverandThe Master Key System: 28 Parts, Questions and AnswersRating: 5 out of 5 stars5/5 (62)
- Brand Identity Breakthrough: How to Craft Your Company's Unique Story to Make Your Products IrresistibleFrom EverandBrand Identity Breakthrough: How to Craft Your Company's Unique Story to Make Your Products IrresistibleRating: 4.5 out of 5 stars4.5/5 (48)
- Take Your Shot: How to Grow Your Business, Attract More Clients, and Make More MoneyFrom EverandTake Your Shot: How to Grow Your Business, Attract More Clients, and Make More MoneyRating: 5 out of 5 stars5/5 (22)
- Secrets of the Millionaire Mind: Mastering the Inner Game of WealthFrom EverandSecrets of the Millionaire Mind: Mastering the Inner Game of WealthRating: 4.5 out of 5 stars4.5/5 (1026)
- Rich Dad's Before You Quit Your Job: 10 Real-Life Lessons Every Entrepreneur Should Know About Building a Multimillion-Dollar BusinessFrom EverandRich Dad's Before You Quit Your Job: 10 Real-Life Lessons Every Entrepreneur Should Know About Building a Multimillion-Dollar BusinessRating: 4.5 out of 5 stars4.5/5 (407)
- Summary of The Four Agreements: A Practical Guide to Personal Freedom (A Toltec Wisdom Book) by Don Miguel RuizFrom EverandSummary of The Four Agreements: A Practical Guide to Personal Freedom (A Toltec Wisdom Book) by Don Miguel RuizRating: 4.5 out of 5 stars4.5/5 (112)
- Enough: The Simple Path to Everything You Want -- A Field Guide for Perpetually Exhausted EntrepreneursFrom EverandEnough: The Simple Path to Everything You Want -- A Field Guide for Perpetually Exhausted EntrepreneursRating: 5 out of 5 stars5/5 (24)
- Your Next Five Moves: Master the Art of Business StrategyFrom EverandYour Next Five Moves: Master the Art of Business StrategyRating: 5 out of 5 stars5/5 (799)
- Level Up: How to Get Focused, Stop Procrastinating, and Upgrade Your LifeFrom EverandLevel Up: How to Get Focused, Stop Procrastinating, and Upgrade Your LifeRating: 5 out of 5 stars5/5 (22)
- Summary: Who Not How: The Formula to Achieve Bigger Goals Through Accelerating Teamwork by Dan Sullivan & Dr. Benjamin Hardy:From EverandSummary: Who Not How: The Formula to Achieve Bigger Goals Through Accelerating Teamwork by Dan Sullivan & Dr. Benjamin Hardy:Rating: 5 out of 5 stars5/5 (2)
- SYSTEMology: Create time, reduce errors and scale your profits with proven business systemsFrom EverandSYSTEMology: Create time, reduce errors and scale your profits with proven business systemsRating: 5 out of 5 stars5/5 (48)
- Transformed: Moving to the Product Operating ModelFrom EverandTransformed: Moving to the Product Operating ModelRating: 4 out of 5 stars4/5 (1)
- Creating Competitive Advantage: How to be Strategically Ahead in Changing MarketsFrom EverandCreating Competitive Advantage: How to be Strategically Ahead in Changing MarketsRating: 5 out of 5 stars5/5 (2)
- The Science of Positive Focus: Live Seminar: Master Keys for Reaching Your Next LevelFrom EverandThe Science of Positive Focus: Live Seminar: Master Keys for Reaching Your Next LevelRating: 5 out of 5 stars5/5 (51)
- Cryptocurrency for Beginners: A Complete Guide to Understanding the Crypto Market from Bitcoin, Ethereum and Altcoins to ICO and Blockchain TechnologyFrom EverandCryptocurrency for Beginners: A Complete Guide to Understanding the Crypto Market from Bitcoin, Ethereum and Altcoins to ICO and Blockchain TechnologyRating: 4.5 out of 5 stars4.5/5 (300)
- What Self-Made Millionaires Do That Most People Don't: 52 Ways to Create Your Own SuccessFrom EverandWhat Self-Made Millionaires Do That Most People Don't: 52 Ways to Create Your Own SuccessRating: 4.5 out of 5 stars4.5/5 (24)
- The E-Myth Revisited: Why Most Small Businesses Don't Work andFrom EverandThe E-Myth Revisited: Why Most Small Businesses Don't Work andRating: 4.5 out of 5 stars4.5/5 (709)
- 7 Secrets to Investing Like Warren BuffettFrom Everand7 Secrets to Investing Like Warren BuffettRating: 4.5 out of 5 stars4.5/5 (121)
- Summary of The Subtle Art of Not Giving A F*ck: A Counterintuitive Approach to Living a Good Life by Mark Manson: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary of The Subtle Art of Not Giving A F*ck: A Counterintuitive Approach to Living a Good Life by Mark Manson: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (38)
- Startup: How To Create A Successful, Scalable, High-Growth Business From ScratchFrom EverandStartup: How To Create A Successful, Scalable, High-Growth Business From ScratchRating: 4 out of 5 stars4/5 (114)
- 100M Offers Made Easy: Create Your Own Irresistible Offers by Turning ChatGPT into Alex HormoziFrom Everand100M Offers Made Easy: Create Your Own Irresistible Offers by Turning ChatGPT into Alex HormoziNo ratings yet