You might also like
- Jpis 42 105Document5 pagesJpis 42 105Jean Pierre Alcántara VigoNo ratings yet
- SwithcingDocument6 pagesSwithcingKyoko CPNo ratings yet
- Immediate One-Stage Postextraction Implant: A Human Clinical and Histologic Case ReportDocument6 pagesImmediate One-Stage Postextraction Implant: A Human Clinical and Histologic Case ReportBagis Emre GulNo ratings yet
- The Modified Papilla Preservation-1Document6 pagesThe Modified Papilla Preservation-1Razvan SalageanNo ratings yet
- 23 03 09 07 03 11 - ExpansionDocument5 pages23 03 09 07 03 11 - ExpansionRaed Abu HamadNo ratings yet
- Aumento de Reborde Con Tejido BlandoDocument8 pagesAumento de Reborde Con Tejido BlandoSilvia SolisNo ratings yet
- Ideas and Innovations: George L. Murrell, M.D., Ricardo Requena, D.O., and Daniel W. Karakla, M.DDocument5 pagesIdeas and Innovations: George L. Murrell, M.D., Ricardo Requena, D.O., and Daniel W. Karakla, M.DVijay Prabu GNo ratings yet
- Nasopalatine Duct Cyst - A Delayed Complication To Successful Dental Implant Placement - Diagnosis and Surgical Management - As Published in The JOIDocument6 pagesNasopalatine Duct Cyst - A Delayed Complication To Successful Dental Implant Placement - Diagnosis and Surgical Management - As Published in The JOIHashem Motahir Ali Al-ShamiriNo ratings yet
- Soft Obturator Prosthesis For Postoperative Soft Palate Carcinoma: A Clinical ReportDocument3 pagesSoft Obturator Prosthesis For Postoperative Soft Palate Carcinoma: A Clinical ReportManjulika TysgiNo ratings yet
- Pouch Roll Technique For Implant Soft Tissue Augmentation - A Variation of The Modified Roll TechniqueDocument6 pagesPouch Roll Technique For Implant Soft Tissue Augmentation - A Variation of The Modified Roll TechniqueAnthony LiNo ratings yet
- Bone Ring 1Document6 pagesBone Ring 1Pradusha RevuruNo ratings yet
- Cheng 2020Document5 pagesCheng 202011pjNo ratings yet
- Immediate Implants Placed Into Infected Sites: A Clinical ReportDocument12 pagesImmediate Implants Placed Into Infected Sites: A Clinical ReportMárcia ChatelieNo ratings yet
- Mandibular Fractures Associated With Endosteal Implants PDFDocument8 pagesMandibular Fractures Associated With Endosteal Implants PDFHélio AlvesNo ratings yet
- Removal Of..Document4 pagesRemoval Of..Andrea ValverdeNo ratings yet
- Fugazzotto ImmediateImplantPlacementMolarDocument7 pagesFugazzotto ImmediateImplantPlacementMolarLozovan GregoryNo ratings yet
- 2020 Article 265Document7 pages2020 Article 265Fabian BarretoNo ratings yet
- Cleft PalateDocument4 pagesCleft PalateShoaib A. KaziNo ratings yet
- Artículo Khoury2018Document10 pagesArtículo Khoury2018Basma Derdabi100% (1)
- Zhao 2020Document2 pagesZhao 2020miraraspopovic020No ratings yet
- A New Approach To The Treatment of True-Combined Endodontic-Periodontic Lesions by The Guided Tissue Regeneration TechniqueDocument4 pagesA New Approach To The Treatment of True-Combined Endodontic-Periodontic Lesions by The Guided Tissue Regeneration TechniqueKarin Noga VerhagenNo ratings yet
- Roll Man 2013Document6 pagesRoll Man 2013SergioNo ratings yet
- Oh 2010Document5 pagesOh 2010gbaez.88No ratings yet
- Augmentation of The Sinus Floor With Mandibular Bone Block and Simultaneous Implantation: A 6-Year Clinical InvestigationDocument8 pagesAugmentation of The Sinus Floor With Mandibular Bone Block and Simultaneous Implantation: A 6-Year Clinical InvestigationWesley Silva100% (1)
- Maier 2016Document8 pagesMaier 2016Luca AlbuquerqueNo ratings yet
- Injertos Aumento RebordeDocument13 pagesInjertos Aumento Rebordejose miguel perez rodriguez100% (1)
- A New Protocol For Immediate ImplantsDocument12 pagesA New Protocol For Immediate ImplantsVikas Aggarwal100% (3)
- Ejoi 12 4 Bittner p469Document12 pagesEjoi 12 4 Bittner p469Maria Gabriela ChapaNo ratings yet
- Direct Maxillary Sinus Lift For Single Tooth Implant A Clinical StudyDocument4 pagesDirect Maxillary Sinus Lift For Single Tooth Implant A Clinical StudyRadita Dwihaning PutriNo ratings yet
- Per I OoooooDocument7 pagesPer I OooooorisjunNo ratings yet
- Ivan Bokan. Potential of Gingival Connective Tissne To Induce Keratinization of An Alveolar Mucosal Flap A Long Term Histologie and Clinical Assessment. Case Report. (Q PDFDocument7 pagesIvan Bokan. Potential of Gingival Connective Tissne To Induce Keratinization of An Alveolar Mucosal Flap A Long Term Histologie and Clinical Assessment. Case Report. (Q PDFJulio César PlataNo ratings yet
- Jurnal AccDocument6 pagesJurnal AcchelmysiswantoNo ratings yet
- Article 009Document9 pagesArticle 009MedstudNo ratings yet
- Bone Ring 3Document4 pagesBone Ring 3Pradusha RevuruNo ratings yet
- Biologically Oriented Preparation Technique (BOPT) For Implant-Supported Fixed ProsthesesDocument5 pagesBiologically Oriented Preparation Technique (BOPT) For Implant-Supported Fixed ProsthesesazazelNo ratings yet
- Positioning Magnets On A Multiple/Sectional Maxillofacial ProsthesisDocument7 pagesPositioning Magnets On A Multiple/Sectional Maxillofacial Prosthesisڣـڕٱټـي آڵـھـۈئNo ratings yet
- Papilla Preservation Between Two Implants: A Modified Socket-Shield Technique To Maintain The Scalloped Anatomy? A Case ReportDocument8 pagesPapilla Preservation Between Two Implants: A Modified Socket-Shield Technique To Maintain The Scalloped Anatomy? A Case ReportsnkidNo ratings yet
- Cheng2006 PDFDocument4 pagesCheng2006 PDFPremshith CpNo ratings yet
- Riparticol-Onofrei Cosmin Gr13Document8 pagesRiparticol-Onofrei Cosmin Gr13Cosmin OnofreiNo ratings yet
- Bone and Tissue LevelDocument3 pagesBone and Tissue LevelSaleh AlsadiNo ratings yet
- Ijomi 15 193 PDFDocument4 pagesIjomi 15 193 PDFBagis Emre GulNo ratings yet
- Jurnal Periapikal 2Document6 pagesJurnal Periapikal 2Rahmania AlikhlasNo ratings yet
- Tor Torelli 1968Document7 pagesTor Torelli 1968Viviana CanteroNo ratings yet
- Use of Pedicled Buccal Fat Pad ForDocument5 pagesUse of Pedicled Buccal Fat Pad ForTATIANA BARRIOS ESCORCIANo ratings yet
- Easy Graft: "Bioabsorbable Root Analogue For Closure of Oroantral Communications After Tooth Extraction: A Prospective Case-Cohort Study"Document7 pagesEasy Graft: "Bioabsorbable Root Analogue For Closure of Oroantral Communications After Tooth Extraction: A Prospective Case-Cohort Study"Dentapex ThailandNo ratings yet
- Distalization of Impacted Mandibular SecondDocument6 pagesDistalization of Impacted Mandibular SecondPatricia BurbanoNo ratings yet
- Management of d-PTFE Membrane Exposure For Having Final Clinical SuccessDocument3 pagesManagement of d-PTFE Membrane Exposure For Having Final Clinical SuccessNidia TorreaNo ratings yet
- Crim - Dentistry2013 260707Document5 pagesCrim - Dentistry2013 260707gamhaelNo ratings yet
- +distraction Osteogenesis For The Cleftlip and PalateDocument12 pages+distraction Osteogenesis For The Cleftlip and PalategrisguzlNo ratings yet
- Isaksson 1992Document6 pagesIsaksson 1992Rohan BhagatNo ratings yet
- CR2 CocktailManagement KhusbooMishraDocument6 pagesCR2 CocktailManagement KhusbooMishradella sainNo ratings yet
- CCR3 4 831 PDFDocument7 pagesCCR3 4 831 PDFArmareality ArmarealityNo ratings yet
- Botticelli 2004Document9 pagesBotticelli 2004medNo ratings yet
- 10 1016@j Prosdent 2005 10 014Document5 pages10 1016@j Prosdent 2005 10 014everaldocruzNo ratings yet
- 1 Three Years Follow Up of Combined Perio EndoDocument3 pages1 Three Years Follow Up of Combined Perio EndohanNo ratings yet
- Crid2014 658790Document6 pagesCrid2014 658790paula catanaNo ratings yet
- Articulo ProtodonciaDocument5 pagesArticulo ProtodonciaMilton David Rios SerratoNo ratings yet
- Rosa 2014Document6 pagesRosa 2014Michal PerkowskiNo ratings yet
- 11 - Zygomatic ImplantDocument13 pages11 - Zygomatic ImplantMohammed AL-SabahiNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- Jurnal 1Document7 pagesJurnal 1Nur WahyuniNo ratings yet
- Oroantral Communication, Its Causes, Complications, Treatments and Radiographic Features: A Pictorial ReviewDocument5 pagesOroantral Communication, Its Causes, Complications, Treatments and Radiographic Features: A Pictorial ReviewNur WahyuniNo ratings yet
- Medi 100 E24311Document5 pagesMedi 100 E24311Nur WahyuniNo ratings yet
- Alternative Method To Treat Oroantral Communication and Fistula With Autogenous Bone Graft and Platelet Rich FirbinDocument6 pagesAlternative Method To Treat Oroantral Communication and Fistula With Autogenous Bone Graft and Platelet Rich FirbinNur WahyuniNo ratings yet
- Liu 2019Document17 pagesLiu 2019Nur WahyuniNo ratings yet
- Kirankumarkrishanappa 2018Document28 pagesKirankumarkrishanappa 2018Nur WahyuniNo ratings yet
- Ethiopian Chicken (Doro Wat Stew) Recipe - FoodDocument2 pagesEthiopian Chicken (Doro Wat Stew) Recipe - FoodPalomequeNo ratings yet
- Basics of Therapeutic DietsDocument12 pagesBasics of Therapeutic DietstiruchanurNo ratings yet
- Aliza Updated ResumeDocument2 pagesAliza Updated Resumeapi-359939852No ratings yet
- Konsolidasi WelmiDocument72 pagesKonsolidasi WelmiWelmi Sulfatri IshakNo ratings yet
- Approach To The Patient in Shock: by James Holencik, DODocument52 pagesApproach To The Patient in Shock: by James Holencik, DOLydia MamurNo ratings yet
- EMP Procedure in MalaysiaDocument24 pagesEMP Procedure in Malaysialamkinpark3373No ratings yet
- Hemodynamic MonitoringDocument35 pagesHemodynamic MonitoringWiz SamNo ratings yet
- Muhanga District Development Plan 2013-2018-1 01Document116 pagesMuhanga District Development Plan 2013-2018-1 01Joseph Tuseku Officiel100% (1)
- Eritro Papulo Skuamosa 2021Document47 pagesEritro Papulo Skuamosa 2021Yolanda Agnesia Purba0% (1)
- Department of Education: Catherine B. Operaña, EddDocument5 pagesDepartment of Education: Catherine B. Operaña, EddMarica PangilinanNo ratings yet
- ODMP Sustainable Livestock Management - Watering Points Appendix 1 - Borehole DataDocument35 pagesODMP Sustainable Livestock Management - Watering Points Appendix 1 - Borehole DataAse JohannessenNo ratings yet
- 28 CryptorchidismDocument23 pages28 CryptorchidismFaisal Ibn MushtaqNo ratings yet
- Dheeraj DumirDocument11 pagesDheeraj DumirAnonymous CR8v7xb0No ratings yet
- Flux Cored Arc Welding NC IIDocument73 pagesFlux Cored Arc Welding NC IIAJ AcuñaNo ratings yet
- Hematology EMQDocument7 pagesHematology EMQfrabzi100% (1)
- Foundation of Professional Nursing PracticeDocument5 pagesFoundation of Professional Nursing PracticeIvan LouiseNo ratings yet
- Cleft Lip and PalateDocument18 pagesCleft Lip and Palateicywitch100% (1)
- Individuals Trained To The Awareness Level Are Personnel Who Are Likely To Witness An Incident and Have Been Trained To Initiate Emergency Response byDocument21 pagesIndividuals Trained To The Awareness Level Are Personnel Who Are Likely To Witness An Incident and Have Been Trained To Initiate Emergency Response byacastillojose100% (1)
- Complete Holistic Guide To Working Out in The GymDocument218 pagesComplete Holistic Guide To Working Out in The Gympsichi21No ratings yet
- Norma Ashrae 62 1989Document3 pagesNorma Ashrae 62 1989Mittzi CallejasNo ratings yet
- Hizon Interview Group 2Document3 pagesHizon Interview Group 2Dan HizonNo ratings yet
- Curriculum Vitae: Personal InformationDocument4 pagesCurriculum Vitae: Personal InformationajmanNo ratings yet
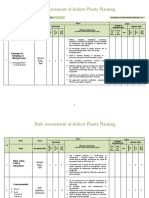
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- AIA IHS Clinics With TCM - Generic (120613)Document43 pagesAIA IHS Clinics With TCM - Generic (120613)junkaiiiNo ratings yet
- OB 2.5 Intrapartum AssessmentDocument9 pagesOB 2.5 Intrapartum AssessmentisahNo ratings yet
- Chapter 2 Fire Fighter SafetyDocument2 pagesChapter 2 Fire Fighter SafetyMuhammad Alshikh100% (1)
- SITHKOP005 - Written AssessmentDocument7 pagesSITHKOP005 - Written AssessmentTephieNo ratings yet
- Wa0011Document12 pagesWa0011Frengky AndikaNo ratings yet
- JUVENILE Justice ProjectDocument24 pagesJUVENILE Justice ProjectyashaNo ratings yet
- Grade 9 Solid Waste Management Teachers - GuideDocument32 pagesGrade 9 Solid Waste Management Teachers - GuideNicole Angela NavarroNo ratings yet