You might also like
- CardiologyDocument62 pagesCardiologysee yinNo ratings yet
- Lippincott 39 S Anesthesia Review 1001 Questions A PDFDocument429 pagesLippincott 39 S Anesthesia Review 1001 Questions A PDFPeter Kazarin50% (2)
- Chan, Johnson - TreatmentGuidelines PDFDocument0 pagesChan, Johnson - TreatmentGuidelines PDFBogdan CarabasNo ratings yet
- Approach To The Adult Patient With Syncope in The Emergency DepartmentDocument26 pagesApproach To The Adult Patient With Syncope in The Emergency DepartmentVinicius DumontNo ratings yet
- Hepatic Encephalopathy and ComaDocument19 pagesHepatic Encephalopathy and ComaJas Castro JoveroNo ratings yet
- Vitamin E - Dr. Wilfrid E. Shute's Complete Updated Vi - Shute, Wilfrid E., 1907Document236 pagesVitamin E - Dr. Wilfrid E. Shute's Complete Updated Vi - Shute, Wilfrid E., 1907Anonymous gwFqQcnaX100% (2)
- Pacing Week PresentationsDocument54 pagesPacing Week PresentationsjoejenningsNo ratings yet
- Feb 09 Harvey Diamond Fit 4 Life)Document4 pagesFeb 09 Harvey Diamond Fit 4 Life)bethany50% (2)
- American Heart Association Guidelines For CPR 2015: Christopher RyalinoDocument50 pagesAmerican Heart Association Guidelines For CPR 2015: Christopher RyalinoLightNo ratings yet
- Swan Ganz CathetersDocument27 pagesSwan Ganz CatheterschadchimaNo ratings yet
- Q: Characterize The Different Types of Pacemaker. Explain The Various Steps of PacingDocument4 pagesQ: Characterize The Different Types of Pacemaker. Explain The Various Steps of PacingKRUPALITHAKKAR100% (1)
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- MVR CabgDocument57 pagesMVR CabgRoshani sharmaNo ratings yet
- Capnography and Its ApplicationsDocument37 pagesCapnography and Its ApplicationsTraceNo ratings yet
- Necrotizing Otitis 2022Document20 pagesNecrotizing Otitis 2022asmashNo ratings yet
- CABGDocument3 pagesCABGprofarmahNo ratings yet
- DR Lila - Patient Preparation For Emergencies Surgeries - New 11012017Document37 pagesDR Lila - Patient Preparation For Emergencies Surgeries - New 11012017bloadyroar100% (1)
- Management of Shock: Role of Inotropic & Vasoactive DrugsDocument50 pagesManagement of Shock: Role of Inotropic & Vasoactive DrugsbajaocNo ratings yet
- Major Haemorrhage ProtocolsDocument3 pagesMajor Haemorrhage ProtocolsleicesterbugNo ratings yet
- Management of The EVDDocument7 pagesManagement of The EVDplethoraldork100% (1)
- Global MigrationDocument31 pagesGlobal MigrationAlthea AlcalaNo ratings yet
- Wide QRS Complex TachyarrhythmiaDocument36 pagesWide QRS Complex TachyarrhythmiaMaruliNo ratings yet
- Seminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingDocument52 pagesSeminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingAyen AlingNo ratings yet
- 29744226: Cerebral Pathophysiology in Extracorporeal Membrane Oxygenation Pitfalls in Daily Clinical ManagementDocument11 pages29744226: Cerebral Pathophysiology in Extracorporeal Membrane Oxygenation Pitfalls in Daily Clinical ManagementEward Rod SalNo ratings yet
- How-to Manual for Pacemaker and ICD Devices: Procedures and ProgrammingFrom EverandHow-to Manual for Pacemaker and ICD Devices: Procedures and ProgrammingNo ratings yet
- Gap Co2 Cocc 2018Document9 pagesGap Co2 Cocc 2018Cesar Rivas CamposNo ratings yet
- FinaDocument6 pagesFinaPablo Sure20% (5)
- Perioperative Cardiovascular Evaluation For Noncardiac SurgeryDocument46 pagesPerioperative Cardiovascular Evaluation For Noncardiac SurgeryErinne DefrianiNo ratings yet
- This Study Resource Was: Cardiogenic ShockDocument5 pagesThis Study Resource Was: Cardiogenic ShockShyla Manguiat100% (1)
- ARDSnet Protocols PDFDocument2 pagesARDSnet Protocols PDFvbfisioNo ratings yet
- Initial Assessment and ManagementDocument8 pagesInitial Assessment and ManagementAlvin De LunaNo ratings yet
- Cardiac ArrestDocument49 pagesCardiac Arrestpraveenkumar biradarNo ratings yet
- 2 EsiDocument23 pages2 EsizianaNo ratings yet
- Post-Cardiac Arrest Management in Adults - UpToDateDocument34 pagesPost-Cardiac Arrest Management in Adults - UpToDatehatsune100% (1)
- Conducting A: Literature SearchDocument32 pagesConducting A: Literature SearchSolehah OmarNo ratings yet
- FAQs Catheter-Associated Urinary Tract InfectionDocument1 pageFAQs Catheter-Associated Urinary Tract InfectioncateterdoblejotaNo ratings yet
- Ivc FilterDocument15 pagesIvc FilterashishNo ratings yet
- Care of Patient With TPM Slide PresentationDocument16 pagesCare of Patient With TPM Slide PresentationirzehronNo ratings yet
- Selected Nursing Diagnoses and Interventions For Patients With DysrhythmiasDocument19 pagesSelected Nursing Diagnoses and Interventions For Patients With Dysrhythmiaslanie_jecielNo ratings yet
- Cardiopulmonary Bypass: Dr. Ravi Gadani MS, FmasDocument24 pagesCardiopulmonary Bypass: Dr. Ravi Gadani MS, FmasRaviNo ratings yet
- Nursing Management of Mechanically Ventilated PatientsDocument179 pagesNursing Management of Mechanically Ventilated PatientsSourabh AlawaNo ratings yet
- Cardiopulmonary BypassDocument62 pagesCardiopulmonary BypassNidya Putri100% (1)
- Isbi Practice Guidelines For Burn Care Part 2 2018 PDFDocument90 pagesIsbi Practice Guidelines For Burn Care Part 2 2018 PDFAstri SuyataNo ratings yet
- Supraventricular TachycardiaDocument9 pagesSupraventricular TachycardiaclubsanatateNo ratings yet
- CPRDocument4 pagesCPRjeetNo ratings yet
- Baska MaskDocument8 pagesBaska MaskAnish H DaveNo ratings yet
- Emergency Drug (Finale)Document49 pagesEmergency Drug (Finale)SN. CaR67% (3)
- Blood Gas Analysis For Bedside DiagnosisDocument6 pagesBlood Gas Analysis For Bedside DiagnosisMuhamad Wirawan AdityoNo ratings yet
- Cardiac SurgeryDocument27 pagesCardiac SurgeryReeti Singh100% (1)
- Coronary Artery Bypass Graft Report NCM 118Document23 pagesCoronary Artery Bypass Graft Report NCM 118Vhince Norben PiscoNo ratings yet
- Hepatic EncephalopathyDocument21 pagesHepatic EncephalopathyAnonymous n3qy0JdCgNo ratings yet
- Contrast EchocardiographyDocument54 pagesContrast EchocardiographySruthiNo ratings yet
- A Guide To ECG Reporting For Year 3 Medical StudentsDocument2 pagesA Guide To ECG Reporting For Year 3 Medical StudentscsngiuNo ratings yet
- 8.the Atls ProtocolDocument57 pages8.the Atls ProtocolReuben DutiNo ratings yet
- Pleural Fluid AnalysisDocument15 pagesPleural Fluid AnalysisNatalie Sarah MoonNo ratings yet
- Holter MonitoringDocument19 pagesHolter Monitoringomotola Ayobundle-oyewo MA206100% (1)
- Acute Treatment of Hypocalcaemia (Adults)Document2 pagesAcute Treatment of Hypocalcaemia (Adults)Ahed WarwarNo ratings yet
- HBP C315HIS Implant Procedure-eLearnDocument35 pagesHBP C315HIS Implant Procedure-eLearnRichiNo ratings yet
- Arterial LinesDocument9 pagesArterial LinesRei IrincoNo ratings yet
- Nervous System AlterationsDocument45 pagesNervous System AlterationsMajesty ParkerNo ratings yet
- Coronary Artery Bypass SurgeryDocument12 pagesCoronary Artery Bypass SurgeryCarlos Eduardo Quisse SánchezNo ratings yet
- AclsDocument4 pagesAclsAnusha Verghese100% (1)
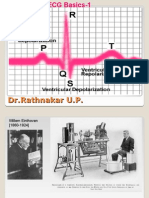
- ECG Basics 1Document24 pagesECG Basics 1Dr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Anaphylaxis CEACCP 2004Document3 pagesAnaphylaxis CEACCP 2004kuruppukarlNo ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
- Practice Essentials: Signs and SymptomsDocument17 pagesPractice Essentials: Signs and Symptomsdwi rizky kurniatiNo ratings yet
- Updated Lists of Controlled Substances As of October 2019Document14 pagesUpdated Lists of Controlled Substances As of October 2019Marlon RondainNo ratings yet
- The Global MigrationDocument3 pagesThe Global MigrationAlthea AlcalaNo ratings yet
- Organ Donation What Is Organ Donation?Document10 pagesOrgan Donation What Is Organ Donation?Althea AlcalaNo ratings yet
- WEEK 16 Filipino Culture Practices and Beliefs 118 LecDocument6 pagesWEEK 16 Filipino Culture Practices and Beliefs 118 LecAlthea AlcalaNo ratings yet
- Professional Negligence and The Doctrine of Res Ipsa LoquiturDocument7 pagesProfessional Negligence and The Doctrine of Res Ipsa LoquiturAlthea AlcalaNo ratings yet
- IVT ComplicationsDocument4 pagesIVT ComplicationsAlthea AlcalaNo ratings yet
- Sexual HarassmentDocument5 pagesSexual HarassmentAlthea AlcalaNo ratings yet
- Blood TransfusionDocument8 pagesBlood TransfusionAlthea AlcalaNo ratings yet
- MnemonicsDocument20 pagesMnemonicsKhassmeen Delos Santos AradaniNo ratings yet
- MinnaH SaunaReviewDocument9 pagesMinnaH SaunaReviewRobbyNo ratings yet
- Hemodynamically Stable Left Ventricular Pseudoaneurysm: Who Should Manage - Surgeon or Cardiologist?Document4 pagesHemodynamically Stable Left Ventricular Pseudoaneurysm: Who Should Manage - Surgeon or Cardiologist?asclepiuspdfsNo ratings yet
- Amlodipine Side EffectsDocument6 pagesAmlodipine Side Effects1976gt500No ratings yet
- Jeena Jayan - CV Orig-2Document5 pagesJeena Jayan - CV Orig-2Raghavendran RamachandranNo ratings yet
- Coronary Artery Revascularization in Stable Patients With Diabetes Mellitus - UpToDateDocument22 pagesCoronary Artery Revascularization in Stable Patients With Diabetes Mellitus - UpToDateAnca StanNo ratings yet
- Clinical: MCQ TestDocument47 pagesClinical: MCQ TestAhmed AlrkabeNo ratings yet
- Pharmacological Management of Acute Coronary Syndromes (ACS) and Acute Limb Ischemia (ALI)Document44 pagesPharmacological Management of Acute Coronary Syndromes (ACS) and Acute Limb Ischemia (ALI)hendratj90No ratings yet
- Physiological Changes in Older AdultsDocument30 pagesPhysiological Changes in Older AdultsElla Neiza AngelesNo ratings yet
- New England Journal Medicine: The ofDocument13 pagesNew England Journal Medicine: The ofStefania CristinaNo ratings yet
- Tif30Document49 pagesTif30HCX dghhqNo ratings yet
- Aortoiliac Occlusive DiseaseDocument37 pagesAortoiliac Occlusive Diseasewolff_512No ratings yet
- 100 Important Terminologies in Medical Surgical NursingDocument4 pages100 Important Terminologies in Medical Surgical Nursingyuuki konnoNo ratings yet
- Kertas Kerja PinjamanDocument18 pagesKertas Kerja PinjamanWan AzmanNo ratings yet
- Mfine CardiologistsDocument7 pagesMfine Cardiologistsmfine healthNo ratings yet
- Copd and Cardiovascular Disease: Original ArticleDocument9 pagesCopd and Cardiovascular Disease: Original Articlemgoez077No ratings yet
- Course in The Ward Date & Time Doctor's Order Rationale June 29, 2007 9:50pmDocument3 pagesCourse in The Ward Date & Time Doctor's Order Rationale June 29, 2007 9:50pmSean DadulaNo ratings yet
- Vitamin CDocument3 pagesVitamin Cnichitacristina66No ratings yet
- Lecture 3 PDFDocument24 pagesLecture 3 PDFAya MuhannadNo ratings yet
- Science: Jeanelyn Mae B. Pesimo Grade 11 - Abm St. Gregory The GreatDocument14 pagesScience: Jeanelyn Mae B. Pesimo Grade 11 - Abm St. Gregory The GreatJeanelyn Mae PesimoNo ratings yet
- The Heart III - Chapter 19 Case StudyDocument5 pagesThe Heart III - Chapter 19 Case StudyBrad ConnersNo ratings yet
- ECG in Acute MI The - Unknown OcrDocument366 pagesECG in Acute MI The - Unknown OcrER BearNo ratings yet
- Pathophysiology ErDocument3 pagesPathophysiology ErAlexa A. AldayNo ratings yet
- Cardiomems HF System: Product HighlightsDocument2 pagesCardiomems HF System: Product HighlightsanishNo ratings yet