You might also like
- American Landlord Law: Everything U Need to Know About Landlord-Tenant LawsFrom EverandAmerican Landlord Law: Everything U Need to Know About Landlord-Tenant LawsNo ratings yet
- Form DB-450 Claim For Disability BenefitsDocument2 pagesForm DB-450 Claim For Disability BenefitsWilliam Mattar100% (3)
- Personal Bond of IndemnityDocument4 pagesPersonal Bond of Indemnitysajeer n FORWARDNo ratings yet
- Real Estate Services Marketing Proposal: Presented byDocument31 pagesReal Estate Services Marketing Proposal: Presented bybethlehem100% (1)
- Medical Services Management Business PlanDocument31 pagesMedical Services Management Business Plansilvia67% (3)
- Memorandum of Agreement MapeconDocument7 pagesMemorandum of Agreement MapeconHoward Untalan100% (1)
- INS 21 Chapter9-Insurance PoliciesDocument27 pagesINS 21 Chapter9-Insurance Policiesvenki_hinfotechNo ratings yet
- Maternity Leave Application Form Performa PDFDocument4 pagesMaternity Leave Application Form Performa PDFAnonymous epg6ult78% (9)
- Bajaj Allianz General Insurance CompanyDocument2 pagesBajaj Allianz General Insurance Companysarath potnuriNo ratings yet
- ReillyBrown IAPM 11e PPT Ch02Document72 pagesReillyBrown IAPM 11e PPT Ch02rocky wongNo ratings yet
- Employees' State Insurance Corporation: Strike Out If Not ApplicableDocument1 pageEmployees' State Insurance Corporation: Strike Out If Not Applicablenasir ahmedNo ratings yet
- Esic Claim Sickness Form9Document1 pageEsic Claim Sickness Form9trupti_naik08725No ratings yet
- Employees' State Insurance Corporation: AttestationDocument1 pageEmployees' State Insurance Corporation: Attestationnasir ahmedNo ratings yet
- Employees' State Insurance Corporation: AttestationDocument1 pageEmployees' State Insurance Corporation: Attestationnasir ahmedNo ratings yet
- Employees' State Insurance Corporation: Date................................Document1 pageEmployees' State Insurance Corporation: Date................................nasir ahmedNo ratings yet
- Form 14Document1 pageForm 14hdpanchal86100% (1)
- Form 19Document1 pageForm 19hdpanchal86No ratings yet
- Form 23Document1 pageForm 23hdpanchal86100% (1)
- Notice and Proof of Claim For Disability BenefitsDocument4 pagesNotice and Proof of Claim For Disability BenefitsabramovrNo ratings yet
- Self DeclarationDocument1 pageSelf Declarationnaveenofficial25No ratings yet
- Maternity New Form 19Document2 pagesMaternity New Form 19Mujibur RehmanNo ratings yet
- Form 15Document1 pageForm 15hdpanchal86No ratings yet
- Revised PF Withdrawal Form-19Document3 pagesRevised PF Withdrawal Form-19Sukhveer SinghNo ratings yet
- Employment Untertaking 1027Document1 pageEmployment Untertaking 1027Ashwin JayagurunathanNo ratings yet
- Employees' State Insurance Corporation: Addition/ Deletion in Family Declaration FormDocument1 pageEmployees' State Insurance Corporation: Addition/ Deletion in Family Declaration Formnasir ahmedNo ratings yet
- Employees' State Insurance Corporation: Addition/ Deletion in Family Declaration FormDocument1 pageEmployees' State Insurance Corporation: Addition/ Deletion in Family Declaration Formnasir ahmedNo ratings yet
- Form 24Document1 pageForm 24hdpanchal86No ratings yet
- Form 7Document3 pagesForm 7hdpanchal86No ratings yet
- Personal Accident-1Document3 pagesPersonal Accident-1satish KumarNo ratings yet
- Form 5Document2 pagesForm 5hdpanchal86No ratings yet
- NPS Form 1Document1 pageNPS Form 1DJNo ratings yet
- I Care Staff Reference Data Form 2022 NEWDocument4 pagesI Care Staff Reference Data Form 2022 NEWjaiyesimibukunNo ratings yet
- PPF FormsDocument9 pagesPPF FormsVivek Godgift JNo ratings yet
- Form of Application For LeaveDocument2 pagesForm of Application For LeaveAlvinNo ratings yet
- Panvel Indiabulls Greens Mega Mall Application FormDocument24 pagesPanvel Indiabulls Greens Mega Mall Application FormsharmaabhayNo ratings yet
- Application For Student Registration: Institute of Certified Management Accountants of Sri LankaDocument4 pagesApplication For Student Registration: Institute of Certified Management Accountants of Sri LankaKinGsly Warshamana100% (1)
- 4 - ForM 12A - Claim For Maternity Benefit For SicknessDocument1 page4 - ForM 12A - Claim For Maternity Benefit For SicknessNoushad IIANo ratings yet
- Form-Si-Bond Surety Bond - Sample FormDocument5 pagesForm-Si-Bond Surety Bond - Sample FormMikeDouglasNo ratings yet
- Vantage Loan Application Form: Section A: Particulars of BorrowerDocument9 pagesVantage Loan Application Form: Section A: Particulars of BorrowerOluwaloseyi SekoniNo ratings yet
- Application For LeaveDocument5 pagesApplication For LeavebixoniNo ratings yet
- Ric Jaminzaidad Pvt. LTD.: Application For BookingDocument2 pagesRic Jaminzaidad Pvt. LTD.: Application For BookingANUNo ratings yet
- Bul CMR en PdfiDocument2 pagesBul CMR en PdfiThierry Gnasiri Godwe HinsouNo ratings yet
- Employment Agreement EMPLOYMENT AGREEMENDocument6 pagesEmployment Agreement EMPLOYMENT AGREEMENNSWADI WILLIAMNo ratings yet
- Policy RectDocument17 pagesPolicy Rectप्रेम हेNo ratings yet
- (For All Officers Other Than Group D) : (Through The Head of Office)Document4 pages(For All Officers Other Than Group D) : (Through The Head of Office)Amit GangulyNo ratings yet
- 2022 Surety Form 003Document2 pages2022 Surety Form 003Wandile TembeNo ratings yet
- ObcDocument7 pagesObcRahul SharmaNo ratings yet
- Application FOR Unemployment Benefits Under RA 8291: DateDocument2 pagesApplication FOR Unemployment Benefits Under RA 8291: DateGianJyrellAlbertoCorletNo ratings yet
- Signature of Pensioner.: Here State Name of Agent. Specimen of Agent's Signature Received Payment Signature of AgentDocument1 pageSignature of Pensioner.: Here State Name of Agent. Specimen of Agent's Signature Received Payment Signature of AgentMuhammad Umair ChNo ratings yet
- Habib Bank AG Zurich: Account Opening Requirements - Personal AccountDocument6 pagesHabib Bank AG Zurich: Account Opening Requirements - Personal Accountfaisal_ahsan7919No ratings yet
- Akidul Islam Contact FormDocument3 pagesAkidul Islam Contact FormAnonymous OThBFHuNo ratings yet
- Account Opening Form For Non Resident IndiansDocument3 pagesAccount Opening Form For Non Resident IndiansNobleNo ratings yet
- Life CertificateDocument1 pageLife CertificateDollar KhokharNo ratings yet
- 1 - Renewal Application - Application For Continuance of Federal Kisan Credit Card Scheme - Modified V 2Document6 pages1 - Renewal Application - Application For Continuance of Federal Kisan Credit Card Scheme - Modified V 2AsifayiroorNo ratings yet
- 15 G Form (Blank)Document2 pages15 G Form (Blank)nst27No ratings yet
- Form - CCF - Death Form-2Document1 pageForm - CCF - Death Form-2DEEPAK RAGNo ratings yet
- SB Form 01Document2 pagesSB Form 01Tony M.TomyNo ratings yet
- Form 16Document1 pageForm 16hdpanchal86No ratings yet
- Aia Form 1 PDFDocument3 pagesAia Form 1 PDFVicky PascuaNo ratings yet
- Vul ApplicationDocument4 pagesVul ApplicationJoseph ZafraNo ratings yet
- Vul ApplicationDocument4 pagesVul ApplicationJoseph ZafraNo ratings yet
- Medical Claim FormDocument5 pagesMedical Claim FormRg RrgNo ratings yet
- Maturity Claim (Form No.3825)Document3 pagesMaturity Claim (Form No.3825)Ranjith KandimallaNo ratings yet
- Stinks EdpmDocument1 pageStinks EdpmJakeem SamsonNo ratings yet
- Indemnity - Bond DraftDocument3 pagesIndemnity - Bond Draftnidhi sharmaNo ratings yet
- Government of Pakistan-Esta Code-Chapter-8aDocument84 pagesGovernment of Pakistan-Esta Code-Chapter-8aTahir Khan100% (2)
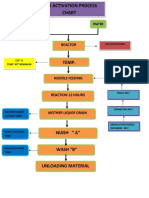
- Acid Activation Process ChartDocument2 pagesAcid Activation Process Chartnasir ahmedNo ratings yet
- Milll 41Document2 pagesMilll 41nasir ahmedNo ratings yet
- Production & Dispatch Graph SheetDocument2 pagesProduction & Dispatch Graph Sheetnasir ahmedNo ratings yet
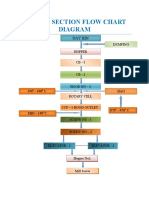
- Drier Section Flow Chart Diagram: Day BinDocument1 pageDrier Section Flow Chart Diagram: Day Binnasir ahmedNo ratings yet
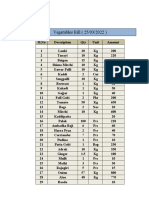
- Vegetable BillDocument2 pagesVegetable Billnasir ahmedNo ratings yet
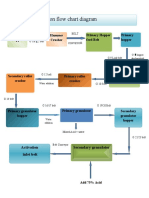
- Granulation Section Flow Chart Diagram: Hammer Crusher Feeding Hopper Primary Hopper Feed Belt Primary HopperDocument1 pageGranulation Section Flow Chart Diagram: Hammer Crusher Feeding Hopper Primary Hopper Feed Belt Primary Hoppernasir ahmedNo ratings yet
- Acid ActivationDocument1 pageAcid Activationnasir ahmedNo ratings yet
- Laboratory Organisational Chart: General ManagerDocument1 pageLaboratory Organisational Chart: General Managernasir ahmedNo ratings yet
- Monthy Production & Dispatch DetailsDocument6 pagesMonthy Production & Dispatch Detailsnasir ahmedNo ratings yet
- Dispatch From Goods ListDocument4 pagesDispatch From Goods Listnasir ahmedNo ratings yet
- Daily Stock Record (Mar)Document35 pagesDaily Stock Record (Mar)nasir ahmedNo ratings yet
- Incharge's Production Report (August) .Document4 pagesIncharge's Production Report (August) .nasir ahmedNo ratings yet
- Production & Dispatch Graph SheetDocument4 pagesProduction & Dispatch Graph Sheetnasir ahmedNo ratings yet
- GRN Report Wash Plant 21-22....Document384 pagesGRN Report Wash Plant 21-22....nasir ahmedNo ratings yet
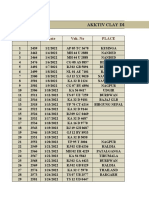
- Akktiv Clay Dispatch Details Jan 2022Document9 pagesAkktiv Clay Dispatch Details Jan 2022nasir ahmedNo ratings yet
- Bajaj Earths StockDocument38 pagesBajaj Earths Stocknasir ahmedNo ratings yet
- Incharge's Production ReportDocument10 pagesIncharge's Production Reportnasir ahmedNo ratings yet
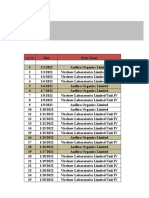
- Granulation Report Jan 2022Document6 pagesGranulation Report Jan 2022nasir ahmedNo ratings yet
- Gypsum Dispatch Details (Dec)Document4 pagesGypsum Dispatch Details (Dec)nasir ahmedNo ratings yet
- Gypsum Dispatch Details (JAN 2022)Document4 pagesGypsum Dispatch Details (JAN 2022)nasir ahmedNo ratings yet
- Daily Stock Record Jan 2022Document33 pagesDaily Stock Record Jan 2022nasir ahmedNo ratings yet
- Bajaj Earths Stock (Sep)Document31 pagesBajaj Earths Stock (Sep)nasir ahmedNo ratings yet
- Bajaj Earth's Wash Plant GRN Report (2022)Document44 pagesBajaj Earth's Wash Plant GRN Report (2022)nasir ahmedNo ratings yet
- GRN Report Wash Plant 21-22....Document419 pagesGRN Report Wash Plant 21-22....nasir ahmedNo ratings yet
- Daily Stock Record (Dec)Document47 pagesDaily Stock Record (Dec)nasir ahmedNo ratings yet
- Akktiv Clay Dispatch Details DecemberDocument6 pagesAkktiv Clay Dispatch Details Decembernasir ahmedNo ratings yet
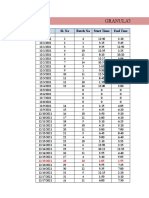
- Granulation Daily Batches Report: Date Sl. No Batch No Start Time End TmeDocument9 pagesGranulation Daily Batches Report: Date Sl. No Batch No Start Time End Tmenasir ahmedNo ratings yet
- Monthly Dispatch Graph SheetDocument2 pagesMonthly Dispatch Graph Sheetnasir ahmedNo ratings yet
- Bajaj Earth's Stock (Dec)Document57 pagesBajaj Earth's Stock (Dec)nasir ahmedNo ratings yet
- Production Report For The NovDocument9 pagesProduction Report For The Novnasir ahmedNo ratings yet
- OTB Notice 2020 08 20 19 15 50 186683Document3 pagesOTB Notice 2020 08 20 19 15 50 18668369j8mpp2sc0% (1)
- Account Statement 191120 191120Document2 pagesAccount Statement 191120 191120Ashutosh KumarNo ratings yet
- 2006 RFP For Epc (Final) 17-03-2006Document257 pages2006 RFP For Epc (Final) 17-03-2006MuyiwacribdNo ratings yet
- Dwnload Full Employment Law For Human Resource Practice 4th Edition Walsh Test Bank PDFDocument7 pagesDwnload Full Employment Law For Human Resource Practice 4th Edition Walsh Test Bank PDFmaihemoynounkq3b100% (9)
- Currency Report - Daily - 14 June 2022 - 14-06-2022 - 09Document4 pagesCurrency Report - Daily - 14 June 2022 - 14-06-2022 - 09Porus Saranjit SinghNo ratings yet
- Tarea para El Lunes 15Document6 pagesTarea para El Lunes 15laura bermudezNo ratings yet
- NR12A - ICC Build Target Cost V4.2Document98 pagesNR12A - ICC Build Target Cost V4.2David WoodhouseNo ratings yet
- Recall 17V-676: Blower Motor Wiring: ModelDocument19 pagesRecall 17V-676: Blower Motor Wiring: Modelsebiru1No ratings yet
- Risk and Its TreatmentDocument3 pagesRisk and Its TreatmentRhealyn RagosNo ratings yet
- Bank of Baroda: (Head Office, Mandvi, Baroda) Particulats To Be Supplied by The Applicant/Guarantor For AdvanceDocument3 pagesBank of Baroda: (Head Office, Mandvi, Baroda) Particulats To Be Supplied by The Applicant/Guarantor For AdvanceShiv DwivediNo ratings yet
- Insurance PPDocument12 pagesInsurance PPSanchit ArtNo ratings yet
- Office of Inspector General Report: Sunrise HospitalDocument53 pagesOffice of Inspector General Report: Sunrise HospitalFOX5 VegasNo ratings yet
- 2011 US GuideDocument28 pages2011 US GuideLoganBohannonNo ratings yet
- Brief Exercises Adjusting The AccountsDocument5 pagesBrief Exercises Adjusting The AccountsYoussef Khaled Mahmoud ShawkyNo ratings yet
- Job Offer-CEC-Relationship Manager-VRM-BRANCH BANKING-VRMDocument3 pagesJob Offer-CEC-Relationship Manager-VRM-BRANCH BANKING-VRMDnyanada NarvekarNo ratings yet
- Cash Surrender ValueDocument14 pagesCash Surrender ValueZonith ValleNo ratings yet
- 76321bos61648 cp4Document172 pages76321bos61648 cp4pikachupiki181No ratings yet
- Mansions of Australia Home and Contents Insurance: Online Quote Request Form Temporary RemovalDocument1 pageMansions of Australia Home and Contents Insurance: Online Quote Request Form Temporary RemovalFilipNo ratings yet
- If1 Insurance Legal and Regulatory Examination SyllabusDocument5 pagesIf1 Insurance Legal and Regulatory Examination Syllabusalexkosenko89No ratings yet
- Ijm 10 06 055Document9 pagesIjm 10 06 055Phạm Phương ThùyNo ratings yet
- Business Studies Final Set2Document3 pagesBusiness Studies Final Set2JOHN JOSHYNo ratings yet
- Payment Terms: Dr. A.K. Sengupta Principal Advisor CED Former Dean, Indian Institute of Foreign TradeDocument14 pagesPayment Terms: Dr. A.K. Sengupta Principal Advisor CED Former Dean, Indian Institute of Foreign TradeimadNo ratings yet
- Crop InsuranceDocument56 pagesCrop InsuranceSharayu BavkarNo ratings yet
- 2020 Registered Insurance Intermediaries As at 19th October 2020-MergedDocument202 pages2020 Registered Insurance Intermediaries As at 19th October 2020-MergedericmNo ratings yet