You might also like
- Employees' State Insurance Corporation: Addition/ Deletion in Family Declaration FormDocument1 pageEmployees' State Insurance Corporation: Addition/ Deletion in Family Declaration Formnasir ahmedNo ratings yet
- Form 1A-Family-Declaration-FormDocument1 pageForm 1A-Family-Declaration-FormyouremailingaparnaNo ratings yet
- The Claims Game: The Tricks and Deceptive Tactics Insurance Companies Use to Underpay or Deny Your ClaimFrom EverandThe Claims Game: The Tricks and Deceptive Tactics Insurance Companies Use to Underpay or Deny Your ClaimNo ratings yet
- Form 2Document1 pageForm 2hdpanchal86No ratings yet
- ESIC1Document2 pagesESIC1hr ShrimannhospitalsNo ratings yet
- PDF Six Sails .Document9 pagesPDF Six Sails .kartik.chahal.ug21No ratings yet
- ESI Form 72ADocument1 pageESI Form 72ASaritha ManishNo ratings yet
- Update Family Details FormDocument1 pageUpdate Family Details FormNoushad IIANo ratings yet
- 15 - FORM 1B - Changes in Family Declaration FormDocument1 page15 - FORM 1B - Changes in Family Declaration FormNoushad IIANo ratings yet
- Form - CCF - Death Form-2Document1 pageForm - CCF - Death Form-2DEEPAK RAGNo ratings yet
- Employees' State Insurance Corporation: Strike Out If Not ApplicableDocument1 pageEmployees' State Insurance Corporation: Strike Out If Not Applicablenasir ahmedNo ratings yet
- Employees' State Insurance Corporation: Strike Out If Not ApplicableDocument1 pageEmployees' State Insurance Corporation: Strike Out If Not Applicablenasir ahmedNo ratings yet
- Ompal Singh AIJPC9375PDocument8 pagesOmpal Singh AIJPC9375PSonia GargNo ratings yet
- Form 15Document1 pageForm 15hdpanchal86No ratings yet
- ESI Declaration FormDocument3 pagesESI Declaration FormSourav SarkarNo ratings yet
- Esic Claim Sickness Form9Document1 pageEsic Claim Sickness Form9trupti_naik08725No ratings yet
- A. I/We The Undersigned: FemaleDocument3 pagesA. I/We The Undersigned: FemaleRishabh ChorariaNo ratings yet
- Application For Reinstatement or Policy ChangeDocument2 pagesApplication For Reinstatement or Policy ChangeCristhelDelaTorreNo ratings yet
- Form 2Document2 pagesForm 2madhubaddapuriNo ratings yet
- Form 24Document1 pageForm 24hdpanchal86No ratings yet
- Wa1104.Document8 pagesWa1104.Anuj KumarNo ratings yet
- Agent RequirementsDocument5 pagesAgent RequirementsamericaategaNo ratings yet
- CA APP Blank FormDocument4 pagesCA APP Blank FormChristine Irish GoyenaNo ratings yet
- 14 - ForM 1A - Family Declaration FormDocument1 page14 - ForM 1A - Family Declaration FormNoushad IIANo ratings yet
- Employees' State Insurance Corporation: AttestationDocument1 pageEmployees' State Insurance Corporation: Attestationnasir ahmedNo ratings yet
- Employees' State Insurance Corporation: AttestationDocument1 pageEmployees' State Insurance Corporation: Attestationnasir ahmedNo ratings yet
- Aap 2021Document1 pageAap 2021Jana NaNo ratings yet
- Workforce JF ISR (1)Document10 pagesWorkforce JF ISR (1)santoshkushwah2No ratings yet
- PF Nomination FormDocument2 pagesPF Nomination FormHR SPEEVO INDUSTRIES LLPNo ratings yet
- PF Form 2Document2 pagesPF Form 2Babu kNo ratings yet
- PF Nomination Form - Form 2Document2 pagesPF Nomination Form - Form 2Jitendra BhatewaraNo ratings yet
- The National Health Insurance Management Authority: Application For Registration As A MemberDocument3 pagesThe National Health Insurance Management Authority: Application For Registration As A MemberRichard シNo ratings yet
- FORM 2 (Revised) : Nomination and Declaration FormDocument2 pagesFORM 2 (Revised) : Nomination and Declaration FormHarshit Suri100% (1)
- ESI FormDocument2 pagesESI Formdaskuntal2285No ratings yet
- Form 1 for ESIC Insurance DetailsDocument3 pagesForm 1 for ESIC Insurance DetailsSiddhant UtekarNo ratings yet
- ESI Form 1 DeclarationDocument2 pagesESI Form 1 Declarationlucky0807No ratings yet
- (A) Insuredperson'S Particulars (B) Employer'S ParticularsDocument2 pages(A) Insuredperson'S Particulars (B) Employer'S Particularsraziqkhan0078129No ratings yet
- DECLARATION FORMDocument2 pagesDECLARATION FORMDilli Rani0% (1)
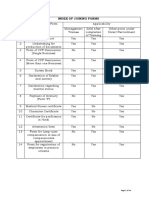
- Index of Joining FormsDocument19 pagesIndex of Joining Formsashwaniv_6No ratings yet
- Employees' insurance formDocument2 pagesEmployees' insurance formaqueeleng100% (1)
- ESI Form2Document2 pagesESI Form2Jay NayakNo ratings yet
- Affidavit For Change of NameDocument2 pagesAffidavit For Change of NameNasiru029100% (3)
- Apply for funding with ID numberDocument2 pagesApply for funding with ID numberThubelihle HadebeNo ratings yet
- DownloadDocument2 pagesDownloadniharxerox180No ratings yet
- PF Nomination Form (Form 2) - SAMPLEDocument2 pagesPF Nomination Form (Form 2) - SAMPLEManas75% (4)
- Beneficiary Nomination-Provident FundDocument2 pagesBeneficiary Nomination-Provident FundBharatSubramonyNo ratings yet
- Notice of Change of Nomination (Form No. 3750) PDFDocument3 pagesNotice of Change of Nomination (Form No. 3750) PDFDesikan100% (1)
- Form - 2 (Editable)Document2 pagesForm - 2 (Editable)Avinash AgrawalNo ratings yet
- Form 2 Nomination and DeclarationDocument2 pagesForm 2 Nomination and DeclarationRenu AmbaniNo ratings yet
- Citibanamex Trust Account ApplicationDocument2 pagesCitibanamex Trust Account Applicationchistopher freundNo ratings yet
- Employees Reg-FormFinal NewDocument3 pagesEmployees Reg-FormFinal NewTimoara NatanNo ratings yet
- Form 2 and EPFODocument4 pagesForm 2 and EPFOSabarish T ENo ratings yet
- Form For Making Nomination in GratuityDocument1 pageForm For Making Nomination in GratuityarushicapricornNo ratings yet
- Apply for funding with IDDocument2 pagesApply for funding with IDAmanda MalingaNo ratings yet
- FORM P300F1 OAB R0 Claim For Old Age Benefit PDFDocument2 pagesFORM P300F1 OAB R0 Claim For Old Age Benefit PDFDhanraj SinghNo ratings yet
- Death Claim FormDocument4 pagesDeath Claim FormudufkhkfysfkgoNo ratings yet
- Alam & Brothers Afidabit 111Document4 pagesAlam & Brothers Afidabit 111gawsia computerNo ratings yet
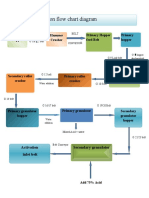
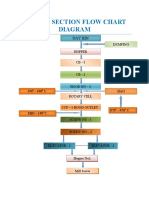
- Granulation Section Flow Chart Diagram: Hammer Crusher Feeding Hopper Primary Hopper Feed Belt Primary HopperDocument1 pageGranulation Section Flow Chart Diagram: Hammer Crusher Feeding Hopper Primary Hopper Feed Belt Primary Hoppernasir ahmedNo ratings yet
- Acid ActivationDocument1 pageAcid Activationnasir ahmedNo ratings yet
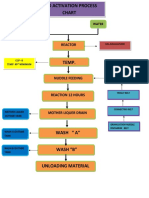
- Acid Activation Process ChartDocument2 pagesAcid Activation Process Chartnasir ahmedNo ratings yet
- Daily Stock Record (Mar)Document35 pagesDaily Stock Record (Mar)nasir ahmedNo ratings yet
- Drier Section Flow Chart Diagram: Day BinDocument1 pageDrier Section Flow Chart Diagram: Day Binnasir ahmedNo ratings yet
- Monthy Production & Dispatch DetailsDocument6 pagesMonthy Production & Dispatch Detailsnasir ahmedNo ratings yet
- Laboratory Organisational Chart: General ManagerDocument1 pageLaboratory Organisational Chart: General Managernasir ahmedNo ratings yet
- Milll 41Document2 pagesMilll 41nasir ahmedNo ratings yet
- Production Report for August - Bags, ETP, and Activation BatchesDocument4 pagesProduction Report for August - Bags, ETP, and Activation Batchesnasir ahmedNo ratings yet
- Vegetables Bill March 2022Document2 pagesVegetables Bill March 2022nasir ahmedNo ratings yet
- Production & Dispatch Graph SheetDocument4 pagesProduction & Dispatch Graph Sheetnasir ahmedNo ratings yet
- Bajaj Earths Stock (Sep)Document31 pagesBajaj Earths Stock (Sep)nasir ahmedNo ratings yet
- Dispatch From Goods ListDocument4 pagesDispatch From Goods Listnasir ahmedNo ratings yet
- Production & Dispatch Graph SheetDocument2 pagesProduction & Dispatch Graph Sheetnasir ahmedNo ratings yet
- GRN Report Wash Plant 21-22....Document384 pagesGRN Report Wash Plant 21-22....nasir ahmedNo ratings yet
- Gypsum Dispatch Details (JAN 2022)Document4 pagesGypsum Dispatch Details (JAN 2022)nasir ahmedNo ratings yet
- Bajaj Earths StockDocument38 pagesBajaj Earths Stocknasir ahmedNo ratings yet
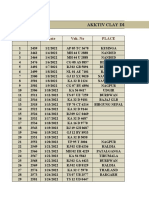
- Akktiv Clay Dispatch Details Jan 2022Document9 pagesAkktiv Clay Dispatch Details Jan 2022nasir ahmedNo ratings yet
- Daily Acid and Lime RecordsDocument33 pagesDaily Acid and Lime Recordsnasir ahmedNo ratings yet
- Granulation Report Jan 2022Document6 pagesGranulation Report Jan 2022nasir ahmedNo ratings yet
- Daily Stock Record (Dec)Document47 pagesDaily Stock Record (Dec)nasir ahmedNo ratings yet
- Gypsum Dispatch Details (Dec)Document4 pagesGypsum Dispatch Details (Dec)nasir ahmedNo ratings yet
- Bajaj Earth's Wash Plant GRN Report (2022)Document44 pagesBajaj Earth's Wash Plant GRN Report (2022)nasir ahmedNo ratings yet
- Incharge's Production ReportDocument10 pagesIncharge's Production Reportnasir ahmedNo ratings yet
- GRN Report Wash Plant 21-22....Document419 pagesGRN Report Wash Plant 21-22....nasir ahmedNo ratings yet
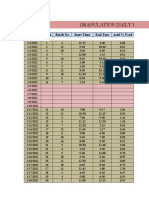
- Granulation Daily Batches Report: Date Sl. No Batch No Start Time End TmeDocument9 pagesGranulation Daily Batches Report: Date Sl. No Batch No Start Time End Tmenasir ahmedNo ratings yet
- Akktiv Clay Dispatch Details DecemberDocument6 pagesAkktiv Clay Dispatch Details Decembernasir ahmedNo ratings yet
- Production Report November 2021Document9 pagesProduction Report November 2021nasir ahmedNo ratings yet
- Monthly Dispatch Graph SheetDocument2 pagesMonthly Dispatch Graph Sheetnasir ahmedNo ratings yet
- Bajaj Earth's Stock (Dec)Document57 pagesBajaj Earth's Stock (Dec)nasir ahmedNo ratings yet
- Ge 2 - Purposive Communication: 1st Exam Mechanics & GuidelinesDocument8 pagesGe 2 - Purposive Communication: 1st Exam Mechanics & GuidelinesCarl Monte de RamosNo ratings yet
- Review-Bias and PrejudiceDocument28 pagesReview-Bias and PrejudiceMaria Cecilia LoristoNo ratings yet
- Translation of Key Passages from the Lotus SutraDocument12 pagesTranslation of Key Passages from the Lotus SutraCharly de TaïNo ratings yet
- Intra-corporate Controversy DismissalDocument125 pagesIntra-corporate Controversy DismissalPearl Angeli Quisido CanadaNo ratings yet
- Bible's View on Gambling and Its DangersDocument2 pagesBible's View on Gambling and Its DangersMarcus JacksonNo ratings yet
- Can I Legally Drop Out of School in Switzerland If I Am 16 - Google SucheDocument1 pageCan I Legally Drop Out of School in Switzerland If I Am 16 - Google SucheWilhelm AgenciesNo ratings yet
- 4 Revisi OK CS 6 Katalog Lautan DalamDocument2 pages4 Revisi OK CS 6 Katalog Lautan DalamDedi SetiawanNo ratings yet
- Efficiency of WebsiteDocument9 pagesEfficiency of WebsiteDzul FazwanNo ratings yet
- Chapter 1 Problem 5 To 7Document2 pagesChapter 1 Problem 5 To 7XienaNo ratings yet
- Ginzberg, The Legends of The Jews, Vol. 5 OCR PDFDocument470 pagesGinzberg, The Legends of The Jews, Vol. 5 OCR PDFd-fbuser-59671747No ratings yet
- I Have Studied Under Many Efficient Teachers and I Have Learnt A Lot From ThemDocument1 pageI Have Studied Under Many Efficient Teachers and I Have Learnt A Lot From ThemSHENNIE WONG PUI CHI MoeNo ratings yet
- Module 3Document6 pagesModule 3Sheera MangcoNo ratings yet
- Churchil SpeechDocument5 pagesChurchil Speechchinuuu85br5484No ratings yet
- Hitlist Rank - 2 (96909)Document13 pagesHitlist Rank - 2 (96909)AlokSinghNo ratings yet
- Government of Punjab: Walk in InterviewDocument7 pagesGovernment of Punjab: Walk in InterviewJeshiNo ratings yet
- Velasquez Business Ethics - Short VersionDocument69 pagesVelasquez Business Ethics - Short VersionIndraNo ratings yet
- The Merchant of Venice (Bullough)Document2 pagesThe Merchant of Venice (Bullough)Ana Stc100% (1)
- Thanksgiving MinibookDocument1 pageThanksgiving MinibookIrina FisticanNo ratings yet
- Vandana SP - MacroeconomicsDocument3 pagesVandana SP - Macroeconomicssrikanth_balasubra_1No ratings yet
- Philippine Constitution Association vs Salvador Enriquez ruling on veto power, pork barrelDocument1 pagePhilippine Constitution Association vs Salvador Enriquez ruling on veto power, pork barrellckdscl100% (1)
- What Is Customer Relationship Management (CRM) ?Document4 pagesWhat Is Customer Relationship Management (CRM) ?MALAY KUMARNo ratings yet
- Topic: Arts of East Asia Learning Competencies & CodeDocument4 pagesTopic: Arts of East Asia Learning Competencies & CodeJaimeCrispinoNo ratings yet
- BSP All AboutDocument9 pagesBSP All AboutRomnick VictoriaNo ratings yet
- Marketing Planning & Application: Submitted To Sir Bilal KothariDocument20 pagesMarketing Planning & Application: Submitted To Sir Bilal KothariSAIF ULLAHNo ratings yet
- Scoring Rubric For Automated FS Fabm2Document2 pagesScoring Rubric For Automated FS Fabm2Erica NapigkitNo ratings yet
- Viva Presentation: Ruchi Vinay ChavanDocument54 pagesViva Presentation: Ruchi Vinay ChavanPravin SarafNo ratings yet
- North Baturaja Block PT Terra Global VestalDocument2 pagesNorth Baturaja Block PT Terra Global VestalYoga RiKumoroNo ratings yet
- Merrill & Hemming 2017 IASPM Abstracts PDFDocument211 pagesMerrill & Hemming 2017 IASPM Abstracts PDFDébora GomesNo ratings yet
- The 2015 IMD World Competitiveness ScoreboardDocument1 pageThe 2015 IMD World Competitiveness ScoreboardCarlos G.No ratings yet
- FB Secondary DataDocument8 pagesFB Secondary DataraheelismNo ratings yet