You might also like
- Deprogramming Victims of Brainwashing and Cult-like Mind Control: Methods you can ApplyFrom EverandDeprogramming Victims of Brainwashing and Cult-like Mind Control: Methods you can ApplyNo ratings yet
- Assessment Nursing Diagnosis Planning Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Nursing Diagnosis Planning Nursing Interventions Rationale EvaluationJan Lianne BernalesNo ratings yet
- Rising from the Ashes: Reclaiming Your Life after Narcissistic AbuseFrom EverandRising from the Ashes: Reclaiming Your Life after Narcissistic AbuseNo ratings yet
- NCP Inffective Individual CopingDocument1 pageNCP Inffective Individual CopingNatalie DulawanNo ratings yet
- Toxic Relationship: Practical Steps to Quit an Abusive Relationship (Become Self-Aware Quit Manipulative and Narcissistic Behaviors to Boost Confidence)From EverandToxic Relationship: Practical Steps to Quit an Abusive Relationship (Become Self-Aware Quit Manipulative and Narcissistic Behaviors to Boost Confidence)No ratings yet
- 016 NCPDocument2 pages016 NCPCzarina Santok GasparNo ratings yet
- Summary of The Rogue Hypnotist's Powerful Hypnosis - Revealing Confessions of a Rogue HypnotistFrom EverandSummary of The Rogue Hypnotist's Powerful Hypnosis - Revealing Confessions of a Rogue HypnotistNo ratings yet
- NCP - Suicidal TendencyDocument2 pagesNCP - Suicidal Tendencyяoxel яayмoи eитяeиa100% (5)
- NCPDocument6 pagesNCPKristine SuguitanNo ratings yet
- Nursing Care Plan For Schizophrenic PatientsDocument6 pagesNursing Care Plan For Schizophrenic PatientsHARVEY SELIMNo ratings yet
- Group 2 NCP For Bipolar DisorderDocument8 pagesGroup 2 NCP For Bipolar DisorderFatima Medriza Duran100% (1)
- NCPDocument1 pageNCPTalTal Balcera Beniten100% (1)
- Objectives: Short Term Goals: IndependentDocument3 pagesObjectives: Short Term Goals: IndependentSHARMAINE ANNE POLICIOSNo ratings yet
- Assessment Diagnosis Outcome Interventions Rationanle EvaluationDocument3 pagesAssessment Diagnosis Outcome Interventions Rationanle EvaluationSheng Timbasal AbduraupNo ratings yet
- NSG Care Plan - BipolarDocument17 pagesNSG Care Plan - BipolaraijelethdaldeavilaNo ratings yet
- Cues Diagnosis Planning Implementation Rationale Evaluation: Nursing Care PlanDocument2 pagesCues Diagnosis Planning Implementation Rationale Evaluation: Nursing Care PlanRenz VillalobosNo ratings yet
- Everyone Would Be Better Off Without Me" As Verbalized by The PatientDocument4 pagesEveryone Would Be Better Off Without Me" As Verbalized by The PatientDanica Kate GalleonNo ratings yet
- NCP Low Self Esteem DreiDocument5 pagesNCP Low Self Esteem DreiEllenare RacionNo ratings yet
- NCP No. 5 Risk For SuicideDocument3 pagesNCP No. 5 Risk For SuicideSMJ DRDNo ratings yet
- NCP Group 1Document3 pagesNCP Group 1Basema HashhashNo ratings yet
- Schiz NCPDocument5 pagesSchiz NCPCharisse LuteroNo ratings yet
- NCPDocument3 pagesNCPCharles Mallari Valdez100% (1)
- Ban - Final Evidence Case Analysis PortfolioDocument2 pagesBan - Final Evidence Case Analysis PortfolioDanielle Audrey BanNo ratings yet
- NSG Plan DepressionDocument12 pagesNSG Plan DepressionKavita kumariNo ratings yet
- Major Depression NCPDocument2 pagesMajor Depression NCPSeann LorescoNo ratings yet
- Case Study (Mrs. Greene)Document9 pagesCase Study (Mrs. Greene)Trina Joy DomantayNo ratings yet
- Nursing Care PlanDocument6 pagesNursing Care PlanNeza AgdalesNo ratings yet
- Situational Low Self-Esteem - NCPDocument3 pagesSituational Low Self-Esteem - NCPLizzey YuNo ratings yet
- BPD NCP 1Document4 pagesBPD NCP 1Jordz PlaciNo ratings yet
- NCPDocument2 pagesNCPJoshua DecenaNo ratings yet
- Disturbed Thought Process NCP Gallano May 22 2018Document3 pagesDisturbed Thought Process NCP Gallano May 22 2018Charles Mallari ValdezNo ratings yet
- Nursing Care Plan IIDocument4 pagesNursing Care Plan IIHarlene Joyce ReyNo ratings yet
- NCP, 3 Case StudyDocument9 pagesNCP, 3 Case StudyKrishelle Kate PannigNo ratings yet
- SElf Directed RT Manic Excitement NCP BM DISORDERDocument2 pagesSElf Directed RT Manic Excitement NCP BM DISORDEREden Marie FranciscoNo ratings yet
- ANGEL-NCP - CaseloadDocument7 pagesANGEL-NCP - CaseloadNik Rose ElNo ratings yet
- Chapter-5 - Therapeutic ApproachesDocument12 pagesChapter-5 - Therapeutic ApproachestanavtaruNo ratings yet
- Hopelessness: Assessment Diagnosis Planning Interventions Rationale EvaluationDocument6 pagesHopelessness: Assessment Diagnosis Planning Interventions Rationale EvaluationJasmineNo ratings yet
- ND - Risk For SuicideDocument3 pagesND - Risk For SuicideHu Dawi100% (2)
- Complicated Grief NCPDocument2 pagesComplicated Grief NCPChristine LebicoNo ratings yet
- NCP For CSDocument2 pagesNCP For CSIris Coronel AdamosNo ratings yet
- NCP (Gonzales) Mar 29 - Ventura PDFDocument3 pagesNCP (Gonzales) Mar 29 - Ventura PDFJian VenturaNo ratings yet
- IndependentDocument4 pagesIndependentTel EscorialNo ratings yet
- NCP - Major Depressive DisorderDocument7 pagesNCP - Major Depressive DisorderJaylord Verazon100% (1)
- Case 2 NCPDocument2 pagesCase 2 NCPJohn Carlo BesinNo ratings yet
- Date Cues NSG Dx. Scientific Basis Goal of Care NSG Intervention Rationale Outcome Criteria EvaluationDocument3 pagesDate Cues NSG Dx. Scientific Basis Goal of Care NSG Intervention Rationale Outcome Criteria EvaluationWenalyn Grace Abella LlavanNo ratings yet
- NCP-and-Drug-study For MENDocument8 pagesNCP-and-Drug-study For MENVillie SumandeNo ratings yet
- PTSD NCPDocument2 pagesPTSD NCPDanielle Quemuel Viray0% (1)
- PP Case Study PsyDocument23 pagesPP Case Study PsySriMathi Kasi Malini ArmugamNo ratings yet
- Schizophrenia NCPDocument2 pagesSchizophrenia NCPNicole cuencos100% (2)
- Dayda NursingcareplanDocument23 pagesDayda NursingcareplanMachelle lang sapat naNo ratings yet
- Schizo NCPDocument18 pagesSchizo NCPRoscheen Berg TutorNo ratings yet
- 3 Floor, DPT Building Matina Campus, Davao City Telefax: (082) Phone No.: (082) 300-5456/300-0647 Local 117Document2 pages3 Floor, DPT Building Matina Campus, Davao City Telefax: (082) Phone No.: (082) 300-5456/300-0647 Local 117Rheynel NietesNo ratings yet
- Compromised Family Coping NCPDocument2 pagesCompromised Family Coping NCPJamaeka Gotis100% (1)
- Nursing Care Plan Borderline PD (Client A) NCP #1: Pia Mae D. Buaya N-31Document9 pagesNursing Care Plan Borderline PD (Client A) NCP #1: Pia Mae D. Buaya N-31Pia Mae BuayaNo ratings yet
- NCP Alzheimers DiseaseDocument2 pagesNCP Alzheimers DiseaseShawn TejanoNo ratings yet
- Defensive Coping Related To Perceived Lack of Self-Efficacy As Evidenced by Denial of Obvious ProblemsDocument2 pagesDefensive Coping Related To Perceived Lack of Self-Efficacy As Evidenced by Denial of Obvious ProblemsJeyser T. GamutiaNo ratings yet
- Assessment Diagnosis Planning Goal Implementation Rationale EvaluationDocument5 pagesAssessment Diagnosis Planning Goal Implementation Rationale EvaluationFatima C. Malik3181323No ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanCarl Andre ReyesNo ratings yet
- Graduate School Nursing Care Plan Assessment Nursing Diagnosis Planning Intervention Rationale Expected OutcomeDocument3 pagesGraduate School Nursing Care Plan Assessment Nursing Diagnosis Planning Intervention Rationale Expected OutcomeMary Rose F. MalaluanNo ratings yet
- NCP - Situational Low Self-EsteemDocument1 pageNCP - Situational Low Self-EsteemJamal Agontong0% (1)
- CU Drafts - CovidDocument7 pagesCU Drafts - Covidganda akoNo ratings yet
- CHFDocument12 pagesCHFganda akoNo ratings yet
- Acute Glomerulonephritis LABS&DXDocument4 pagesAcute Glomerulonephritis LABS&DXganda akoNo ratings yet
- Assessmen T Diagnosi S Goal of Care Backgroun D Knowledge Intervention Rationale Evaluatio N Subjective Cues: "Sobrang Independen T: Independen TDocument3 pagesAssessmen T Diagnosi S Goal of Care Backgroun D Knowledge Intervention Rationale Evaluatio N Subjective Cues: "Sobrang Independen T: Independen Tganda akoNo ratings yet
- Hypoglycemia Case StudyDocument4 pagesHypoglycemia Case Studyganda akoNo ratings yet
- 2 Days Meat Processing Training Program (Kalayaan Laguna)Document2 pages2 Days Meat Processing Training Program (Kalayaan Laguna)Jals SaripadaNo ratings yet
- RMU With Eco-Efficient Gas Mixture-Evaluation After Three Years of Field ExperienceDocument5 pagesRMU With Eco-Efficient Gas Mixture-Evaluation After Three Years of Field ExperienceZineddine BENOUADAHNo ratings yet
- The Lafayette Driller: President's Message By: Lindsay LongmanDocument7 pagesThe Lafayette Driller: President's Message By: Lindsay LongmanLoganBohannonNo ratings yet
- Arti ResearchDocument10 pagesArti Researcharti nongbetNo ratings yet
- A Branding Effort of Walt DisneyDocument17 pagesA Branding Effort of Walt DisneyKanishk GuptaNo ratings yet
- Modern Theory of Interest: IS-LM CurveDocument36 pagesModern Theory of Interest: IS-LM CurveSouvik DeNo ratings yet
- EIV Operation ManualDocument339 pagesEIV Operation ManualJJSNo ratings yet
- BF2207 Exercise 6 - Dorchester LimitedDocument2 pagesBF2207 Exercise 6 - Dorchester LimitedEvelyn TeoNo ratings yet
- Taxicab Operators V BOTDocument2 pagesTaxicab Operators V BOTHazel P.No ratings yet
- National School Building Inventory (NSBI) Encoding For SY 2021-2022Document31 pagesNational School Building Inventory (NSBI) Encoding For SY 2021-2022Renato Rivera100% (1)
- Daftar Kalibrasi Peralatan MedisDocument34 pagesDaftar Kalibrasi Peralatan Medisdiklat rssnNo ratings yet
- Teit Cbgs Dmbi Lab Manual FH 2015Document60 pagesTeit Cbgs Dmbi Lab Manual FH 2015Soumya PandeyNo ratings yet
- IBM Tivoli Monitoring Implementation and Performance Optimization For Large Scale Environments Sg247443Document526 pagesIBM Tivoli Monitoring Implementation and Performance Optimization For Large Scale Environments Sg247443bupbechanhNo ratings yet
- HCL Corporate-PresentationDocument14 pagesHCL Corporate-Presentationtony_reddyNo ratings yet
- MCMCHistoryDocument18 pagesMCMCHistoryAli S.No ratings yet
- The Influence of The Transformational LeaderDocument9 pagesThe Influence of The Transformational Leaderkenmuira100% (1)
- BioEdit Version 7.0.0 PDFDocument192 pagesBioEdit Version 7.0.0 PDFJovanderson JacksonNo ratings yet
- Lynette Hawkins, BMG Awesome InsightDocument2 pagesLynette Hawkins, BMG Awesome Insightawesomei100% (1)
- Bonus 6 - Mastering ASP - NET Core SecurityDocument147 pagesBonus 6 - Mastering ASP - NET Core SecurityDark Shadow100% (1)
- 2.how To Boost Your Coating SalesDocument23 pages2.how To Boost Your Coating SalesAjaz Noor KhattakNo ratings yet
- Sony Ericsson Secret MenuDocument2 pagesSony Ericsson Secret MenuZeljana MaksicNo ratings yet
- ColgateDocument32 pagesColgategargatworkNo ratings yet
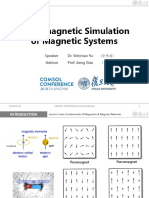
- Micromagnetic Simulation of Magnetic SystemsDocument12 pagesMicromagnetic Simulation of Magnetic SystemsImri SsNo ratings yet
- SamanthavasquezresumeDocument1 pageSamanthavasquezresumeapi-278808369No ratings yet
- Uniarch Network Video Recorders User Manual-V1.00Document99 pagesUniarch Network Video Recorders User Manual-V1.00amurjiantoNo ratings yet
- ECON 202 Optional Problem SetDocument3 pagesECON 202 Optional Problem SetAnthony SabarilloNo ratings yet
- IEC947-5-1 Contactor Relay Utilization CategoryDocument1 pageIEC947-5-1 Contactor Relay Utilization CategoryipitwowoNo ratings yet
- CIVPRO - Case Compilation No. 2Document95 pagesCIVPRO - Case Compilation No. 2Darla GreyNo ratings yet
- Dahua Video Conferencing SolutionDocument16 pagesDahua Video Conferencing SolutionDennis DubeNo ratings yet
- Lower Gasket Kit (S/N E/ 9Fz999 & Below) : Model Number: 335 Serial Number: A9KA11001 & Above, AAD111001 & AboveDocument2 pagesLower Gasket Kit (S/N E/ 9Fz999 & Below) : Model Number: 335 Serial Number: A9KA11001 & Above, AAD111001 & Abovezeeshan tanveerNo ratings yet