You might also like
- Effective Treatments For PTSD, Third Edition - Practice Guidelines From The International Society For Traumatic Stress StudiesDocument579 pagesEffective Treatments For PTSD, Third Edition - Practice Guidelines From The International Society For Traumatic Stress Studieselias sohNo ratings yet
- Suicide Risk Assessment Template UpdatedDocument3 pagesSuicide Risk Assessment Template UpdatedZhillNo ratings yet
- Schiz NCPDocument5 pagesSchiz NCPCharisse LuteroNo ratings yet
- Nursing Care Plan For Schizophrenic PatientsDocument6 pagesNursing Care Plan For Schizophrenic PatientsHARVEY SELIMNo ratings yet
- Clinical Interviewing SkillsDocument27 pagesClinical Interviewing SkillsAcademic Committe100% (1)
- ND - Risk For SuicideDocument3 pagesND - Risk For SuicideHu Dawi100% (1)
- Psychiatric and Mental Health Nursing DemystifiedFrom EverandPsychiatric and Mental Health Nursing DemystifiedRating: 5 out of 5 stars5/5 (1)
- NCP Ineffective CopingDocument5 pagesNCP Ineffective CopingChiara Fajardo0% (3)
- 2 - EndometriosisDocument3 pages2 - EndometriosisJayson Olile100% (1)
- Dementia NCPDocument3 pagesDementia NCPDonnalyn MillaresNo ratings yet
- Nursing Care Plan: "Nabalaka Ko Kay First Time Nako Ma-Operahan, Basin Pud Maunsa Si Baby," AsDocument2 pagesNursing Care Plan: "Nabalaka Ko Kay First Time Nako Ma-Operahan, Basin Pud Maunsa Si Baby," Asunnamed personNo ratings yet
- Risk For InjuryDocument4 pagesRisk For InjuryJanina Patricia BuddleNo ratings yet
- NCP Inffective Individual CopingDocument1 pageNCP Inffective Individual CopingNatalie DulawanNo ratings yet
- Case Study 6Document4 pagesCase Study 6Mary Hope Bacuta0% (2)
- Nursing Care Plan: Phinma University of IloiloDocument2 pagesNursing Care Plan: Phinma University of IloiloBeatrice ManingasNo ratings yet
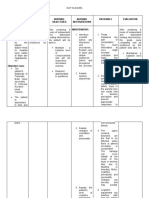
- Nursing Care Plan Assessment Diagnosis Inference Planning Interventio N Rationale EvaluationDocument3 pagesNursing Care Plan Assessment Diagnosis Inference Planning Interventio N Rationale EvaluationDianne100% (2)
- NCP For CSDocument2 pagesNCP For CSIris Coronel AdamosNo ratings yet
- Inability To Bear Down: Problems With The Psyche FactorsDocument4 pagesInability To Bear Down: Problems With The Psyche FactorsErvina Luisa Delias CampusNo ratings yet
- NCP CervicalDocument4 pagesNCP CervicalZaira Kim93% (14)
- Case Study (Mrs. Greene)Document9 pagesCase Study (Mrs. Greene)Trina Joy DomantayNo ratings yet
- Disturbed Thought Processes DescribeDocument2 pagesDisturbed Thought Processes DescribePRINCESS LARA CASILAONo ratings yet
- NCM117 NCPDocument2 pagesNCM117 NCPHANNAH MICOLE GAERLANNo ratings yet
- NCM 117 - Graded SeatworkDocument7 pagesNCM 117 - Graded SeatworkShamsa AfdalNo ratings yet
- Anxiety NCPDocument2 pagesAnxiety NCPeleinsamNo ratings yet
- ADN Care Plan - DepressionDocument3 pagesADN Care Plan - DepressionDavid PerezNo ratings yet
- NCP-and-Drug-study For MENDocument8 pagesNCP-and-Drug-study For MENVillie SumandeNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluationjay5ar5jamorabon5torNo ratings yet
- Concept Map - BipolarDocument1 pageConcept Map - BipolarbacnatjoyNo ratings yet
- GRPD SomaticNCP-1Document2 pagesGRPD SomaticNCP-1Macmac GalabacNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationSesrine BuendiaNo ratings yet
- Nursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceDocument2 pagesNursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceMelinda Cariño BallonNo ratings yet
- Revised. NCP. Jam 1Document3 pagesRevised. NCP. Jam 1ACOB, Jamil C.No ratings yet
- Psychological Adaptations in PostpartumDocument7 pagesPsychological Adaptations in PostpartumKristine JamilleNo ratings yet
- With RationaleDocument4 pagesWith RationaleKaren mae alvarroNo ratings yet
- NCP, 3 Case StudyDocument9 pagesNCP, 3 Case StudyKrishelle Kate PannigNo ratings yet
- NCP - Indi CSDocument6 pagesNCP - Indi CSFretzgine Lou ManuelNo ratings yet
- PSYCH CP DepressionDocument8 pagesPSYCH CP DepressionKendricNo ratings yet
- Nursing Care Plan 1Document5 pagesNursing Care Plan 1kuro hanabusaNo ratings yet
- NCPDocument2 pagesNCPJasmine AliamenNo ratings yet
- Top 2 PriorityDocument6 pagesTop 2 PriorityRonel ResurricionNo ratings yet
- Bipolar 1 Disorder NCPDocument3 pagesBipolar 1 Disorder NCPJoy-Rena Sabinay OchondraNo ratings yet
- ALL NCP Case StudyDocument10 pagesALL NCP Case StudyKing Aldus ConstantinoNo ratings yet
- NCP - Major Depressive DisorderDocument7 pagesNCP - Major Depressive DisorderJaylord Verazon100% (1)
- Date Cues Nsg. DX Scientific Basis Goal of Care NSG Intervention Rationale EvaluationDocument4 pagesDate Cues Nsg. DX Scientific Basis Goal of Care NSG Intervention Rationale EvaluationWenalyn Grace Abella LlavanNo ratings yet
- Bipolar Disorder ReportDocument6 pagesBipolar Disorder ReportLecah DevarasNo ratings yet
- Module 3 Case Analysis 1Document6 pagesModule 3 Case Analysis 1joyrena ochondraNo ratings yet
- NURSINGCAREPLANDocument5 pagesNURSINGCAREPLANJulius AtencioNo ratings yet
- DELIRIUMDocument7 pagesDELIRIUMSHEILA MAE SACLOTNo ratings yet
- Material, Vincent M. (NCP Seizure, Head Trauma, CVA)Document33 pagesMaterial, Vincent M. (NCP Seizure, Head Trauma, CVA)vincent materialNo ratings yet
- Final NCPs For GNDDocument3 pagesFinal NCPs For GNDTin CunetaNo ratings yet
- NCP AshraDocument4 pagesNCP AshraSherry RodriguezNo ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument1 pageSan Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesTrisha Joy T. JumonongNo ratings yet
- 3 Nursing Care PlanDocument6 pages3 Nursing Care PlanJeyser T. GamutiaNo ratings yet
- NCP For SchizoDocument6 pagesNCP For SchizoGILIANNE MARIE JIMENEANo ratings yet
- NCP Knowledge Deficit FINALDocument8 pagesNCP Knowledge Deficit FINALJOSHUA JOSE TERCEnONo ratings yet
- ANXIETYDocument2 pagesANXIETYChombe JcNo ratings yet
- Nursing Care Plan: Cues Diagnosis Planning Implementation Rationale EvaluationDocument3 pagesNursing Care Plan: Cues Diagnosis Planning Implementation Rationale EvaluationChrizley Shawn DeroniaNo ratings yet
- NURSING CARE PLAN (For Case Study)Document2 pagesNURSING CARE PLAN (For Case Study)Kathleen Martinez100% (1)
- SElf Directed RT Manic Excitement NCP BM DISORDERDocument2 pagesSElf Directed RT Manic Excitement NCP BM DISORDEREden Marie FranciscoNo ratings yet
- NCP PsychDocument2 pagesNCP PsychGeovi MitreNo ratings yet
- Nursing Care Management For A Patient With Schizophrenia and Generalized AnxietyDocument23 pagesNursing Care Management For A Patient With Schizophrenia and Generalized AnxietyKimberly Ann BoricanoNo ratings yet
- NCP (Gonzales) Mar 29 - Ventura PDFDocument3 pagesNCP (Gonzales) Mar 29 - Ventura PDFJian VenturaNo ratings yet
- Mindfulness-Based Relapse Prevention: Mindfulness Techniques for Relapse Prevention and RecoveryFrom EverandMindfulness-Based Relapse Prevention: Mindfulness Techniques for Relapse Prevention and RecoveryNo ratings yet
- L2 - Saavedra and SilvermanDocument5 pagesL2 - Saavedra and Silvermanpapá grandeNo ratings yet
- Neuroses VS PsychosisDocument23 pagesNeuroses VS PsychosisChristel Mariz SantellaNo ratings yet
- ADHD in TdcsDocument3 pagesADHD in TdcsAfnan MuntherNo ratings yet
- Cudit R Cannabis Use Disorders Identification TestDocument1 pageCudit R Cannabis Use Disorders Identification TestSanskrit education DepartmentNo ratings yet
- Im So Stressed OutDocument2 pagesIm So Stressed OutAlexandra whimsicalNo ratings yet
- Attachment in Psychotherapy by David J Wallin Guilford Press 2007 366pp Usdollar3900 PB Isbn 9781593854560Document2 pagesAttachment in Psychotherapy by David J Wallin Guilford Press 2007 366pp Usdollar3900 PB Isbn 9781593854560ŤHĚ LÊGÊNDNo ratings yet
- Psych Nursing Post Test 2 Doc F PDFDocument5 pagesPsych Nursing Post Test 2 Doc F PDFTrisha Mae MarquezNo ratings yet
- Maudsley MRW FlyerDocument2 pagesMaudsley MRW Flyerfabioviana67No ratings yet
- Raskin 2018 CH 1Document32 pagesRaskin 2018 CH 1honghagiang.forworkNo ratings yet
- Clinical Interview and PhasesDocument5 pagesClinical Interview and Phasesmomina sarwarNo ratings yet
- Schizophrenia Lecture NotesDocument7 pagesSchizophrenia Lecture NotesHerme BorladoNo ratings yet
- Robertson 1999Document8 pagesRobertson 1999Wanessa AndradeNo ratings yet
- BpadDocument27 pagesBpadnikitabhattarai20No ratings yet
- Marshman Counseling ResumeDocument1 pageMarshman Counseling Resumeapi-598396829No ratings yet
- Positive Affect Treatment For Depression and Anxiety Workbook Alicia E Meuret All ChapterDocument67 pagesPositive Affect Treatment For Depression and Anxiety Workbook Alicia E Meuret All Chapterkaren.dixon505100% (7)
- Roussis & Wells, 2008Document14 pagesRoussis & Wells, 2008Arckantos26No ratings yet
- Mental Health Services in CubaDocument4 pagesMental Health Services in CubaKevin HancockNo ratings yet
- A Rare Case of Obsessive-Compulsive Disorder WithDocument5 pagesA Rare Case of Obsessive-Compulsive Disorder WithAnand JhaNo ratings yet
- Social Anxiety Disorder - EssayDocument1 pageSocial Anxiety Disorder - EssayJesimie OriasNo ratings yet
- Major Depressive Disorder in Adults 2016 (Philippines)Document29 pagesMajor Depressive Disorder in Adults 2016 (Philippines)Doroteo Jose StationNo ratings yet
- Understanding Acupuncture For DepressionDocument9 pagesUnderstanding Acupuncture For DepressionbazediNo ratings yet
- NCDJ Style Guide Edit 2021 SilvermanDocument44 pagesNCDJ Style Guide Edit 2021 SilvermanQuỳnh AnhNo ratings yet
- Toolkit For Counseling Spanish-Speaking ClientsDocument30 pagesToolkit For Counseling Spanish-Speaking ClientsDavid StraussNo ratings yet
- A NiklovaDocument5 pagesA NiklovaJay Mark PornelaNo ratings yet
- Single-Session Manualized Ego State Therapy (EST) For Combat Stress Injury, PTSD, and ASD, Part 1: The TheoryDocument16 pagesSingle-Session Manualized Ego State Therapy (EST) For Combat Stress Injury, PTSD, and ASD, Part 1: The TheorydrkmlNo ratings yet
- Adult Mental Health Reference Guide r70000v2Document72 pagesAdult Mental Health Reference Guide r70000v2Luisa CamposNo ratings yet
- EaTing Disorders BrochureDocument2 pagesEaTing Disorders BrochureMAT Santo Nino FO2No ratings yet