You might also like
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Sinovac - April 15 2021 (Health Assessment Algorithm)Document1 pageSinovac - April 15 2021 (Health Assessment Algorithm)Karen BalanayNo ratings yet
- Health Assessment Algorithm For Sinovac: YES NODocument1 pageHealth Assessment Algorithm For Sinovac: YES NOKim GomezNo ratings yet
- ASSESS THE VACCINE RECIPIENT: Is The Patient Any of The Following?Document1 pageASSESS THE VACCINE RECIPIENT: Is The Patient Any of The Following?saraNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormSusan MatayonNo ratings yet
- Boosters Health Assessment Form ENGDocument1 pageBoosters Health Assessment Form ENGKim GomezNo ratings yet
- Health-Declaration AstraZeneca EngDocument2 pagesHealth-Declaration AstraZeneca EngSheilou MarieNo ratings yet
- Health Assessment FormDocument2 pagesHealth Assessment FormJessa MaeNo ratings yet
- Vaccinees Profile ASTRA SetDocument5 pagesVaccinees Profile ASTRA SetMark Anthony RosasNo ratings yet
- ASTRAZENECA - March 10 2021 (HEALTH DECLARATION SCREENING FORM)Document1 pageASTRAZENECA - March 10 2021 (HEALTH DECLARATION SCREENING FORM)Karen BalanayNo ratings yet
- Congvax Booster HDF Consent FormDocument2 pagesCongvax Booster HDF Consent FormMichael Mangay-atNo ratings yet
- Gamaleya Health Declaration Screening Form Eng - June 9 2021Document1 pageGamaleya Health Declaration Screening Form Eng - June 9 2021LC1 NLCNo ratings yet
- Sinovac - April 15 2021 (Health Declaration Screening Form)Document1 pageSinovac - April 15 2021 (Health Declaration Screening Form)Karen BalanayNo ratings yet
- Health Declaration Screening FormDocument1 pageHealth Declaration Screening FormfitchNo ratings yet
- Moderna (Health Declaration Screening Form) Eng - June 18 2021Document1 pageModerna (Health Declaration Screening Form) Eng - June 18 2021Paulo Justin Tabangcora OropillaNo ratings yet
- Covid Illness Decision Tree 8-31-20 FINALDocument1 pageCovid Illness Decision Tree 8-31-20 FINALSamiNo ratings yet
- Health Declaration and Screening Form For Pedia VaxDocument1 pageHealth Declaration and Screening Form For Pedia VaxMark Lawrence Bael0% (1)
- Imci NotesDocument76 pagesImci Notesjekeri bekeriNo ratings yet
- Isolation and Quarantine For Healthcare WorkersDocument2 pagesIsolation and Quarantine For Healthcare WorkersDan Ver GawaranNo ratings yet
- Drug Study East AveDocument15 pagesDrug Study East AveSean Philippe CabralNo ratings yet
- Paracetamol : Indication: ClassificationDocument1 pageParacetamol : Indication: ClassificationKyla Barrera TabungarNo ratings yet
- Health Assessment Form For Pedia VaxDocument1 pageHealth Assessment Form For Pedia VaxRURAL HEALTH CENTER TAMBLER BAWINGNo ratings yet
- If A Person Has One or More of These Symptoms:: Isolate at HomeDocument3 pagesIf A Person Has One or More of These Symptoms:: Isolate at HomeAl Patrick ChavitNo ratings yet
- Sinovac - March 5 2021 (Health Declaration Screening Form)Document1 pageSinovac - March 5 2021 (Health Declaration Screening Form)IT DepartmentNo ratings yet
- Screenshot 2022-06-28 at 9.33.56 AM PDFDocument1 pageScreenshot 2022-06-28 at 9.33.56 AM PDFhelen S. DeeNo ratings yet
- Latest Quarantine and IsolationDocument6 pagesLatest Quarantine and IsolationDan Ver GawaranNo ratings yet
- KARTU KENDALI ANAK PELAYANAN VAKSINASI COVID DES 2021 6-11thun Kuta 1Document1 pageKARTU KENDALI ANAK PELAYANAN VAKSINASI COVID DES 2021 6-11thun Kuta 1anomnurcahyadiNo ratings yet
- Pfizer Health Declaration Screening Form Eng June 9 2021Document1 pagePfizer Health Declaration Screening Form Eng June 9 2021Kim GomezNo ratings yet
- COVID - Screening - Student - Child Care - Jan6 - AODA - 0Document5 pagesCOVID - Screening - Student - Child Care - Jan6 - AODA - 0KimDoll BNo ratings yet
- DohformDocument1 pageDohformKelvin ChinNo ratings yet
- 2009-2010 Influenza Season Triage Algorithm For Children ( 18 Years) WithDocument1 page2009-2010 Influenza Season Triage Algorithm For Children ( 18 Years) Withapi-25916350No ratings yet
- Nursing Care 2Document1 pageNursing Care 2Moh. H.AlObaidyNo ratings yet
- COVID 19 Screening For Students-2Document2 pagesCOVID 19 Screening For Students-2olashileidowutaylor10No ratings yet
- Recommended Immunization For Filipino Healthcare Workers 2012Document1 pageRecommended Immunization For Filipino Healthcare Workers 2012SMRNo ratings yet
- TDH Return To School Algorithm Updated 1-5-2021Document1 pageTDH Return To School Algorithm Updated 1-5-2021WVLT NewsNo ratings yet
- Midland County Schools Students/Staff COVID-19 Guide 2021-2022 School YearDocument1 pageMidland County Schools Students/Staff COVID-19 Guide 2021-2022 School YearCourtney BennettNo ratings yet
- Drug Study Drug Mechanism of Action Indications Contraindications Side Effects & Adverse Effects Nursing Responsibilities Generic NameDocument4 pagesDrug Study Drug Mechanism of Action Indications Contraindications Side Effects & Adverse Effects Nursing Responsibilities Generic NameNicholas TagleNo ratings yet
- Covid-19 Guideline FlowchartDocument1 pageCovid-19 Guideline FlowchartDavid PanianNo ratings yet
- Integrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsDocument78 pagesIntegrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsWendy EscalanteNo ratings yet
- IMCI Chart 2014 EditionDocument80 pagesIMCI Chart 2014 EditionHarold DiasanaNo ratings yet
- School Decision Tree Exclusion Guidance 20211104Document2 pagesSchool Decision Tree Exclusion Guidance 20211104AnteNo ratings yet
- Integrated Management of Chilhood IllnessesDocument12 pagesIntegrated Management of Chilhood Illnessescorpuzdarryl3No ratings yet
- Recommendations For Oral Surgery During COVID-19 Pandemic: WWW - Rcseng.ac - Uk/dental-Faculties/fds/coronavirusDocument7 pagesRecommendations For Oral Surgery During COVID-19 Pandemic: WWW - Rcseng.ac - Uk/dental-Faculties/fds/coronavirusFaiqotul KumalaNo ratings yet
- Vero RabDocument3 pagesVero RabSeanmarie CabralesNo ratings yet
- COVID-19 Screening Tool For Public Health and Health Links-Info SantéDocument27 pagesCOVID-19 Screening Tool For Public Health and Health Links-Info SantéTsania KusumawardaniNo ratings yet
- Sinovac (Health Declaration Screening Form)Document1 pageSinovac (Health Declaration Screening Form)NUR-FADZILAH ANYAMANNo ratings yet
- CHART BOOKLET Integrated Management of Childhood IllnessDocument79 pagesCHART BOOKLET Integrated Management of Childhood Illnessbonjh0eNo ratings yet
- Cough or ColdDocument3 pagesCough or Coldislafab25No ratings yet
- The Integrated Management of Childhood IllnessDocument83 pagesThe Integrated Management of Childhood Illnesssay04yaocincoNo ratings yet
- Misoprostol: (Mye Soe Prost' Ole) Diarrhea, Abdominal Pain, Flatulence, VomitingDocument4 pagesMisoprostol: (Mye Soe Prost' Ole) Diarrhea, Abdominal Pain, Flatulence, VomitingThrecia RotaNo ratings yet
- C - 19 Protocol Gladwin Public SchoolsDocument8 pagesC - 19 Protocol Gladwin Public SchoolsCourtney BennettNo ratings yet
- Pediatric Community-Acquired Pneumonia Clinical Guideline PDFDocument1 pagePediatric Community-Acquired Pneumonia Clinical Guideline PDFJohn Vincent Dy OcampoNo ratings yet
- Cap PDFDocument1 pageCap PDFroshmaeNo ratings yet
- Pediatric Community-Acquired Pneumonia Clinical GuidelineDocument1 pagePediatric Community-Acquired Pneumonia Clinical GuidelineLowrence Precious Callera DichosoNo ratings yet
- Com Dev 1Document2 pagesCom Dev 1idema2090No ratings yet
- Doh Programs Related To Family Health - Expanded Programs On ImmunizationDocument3 pagesDoh Programs Related To Family Health - Expanded Programs On ImmunizationPatrisha Bianca Paige BadillesNo ratings yet
- Covid 19 (9 Questions)Document1 pageCovid 19 (9 Questions)kushalNo ratings yet
- QC Protektodo Forms Sinopharm 1st Dose AranetaDocument3 pagesQC Protektodo Forms Sinopharm 1st Dose AranetaRalph Clinton PalomenoNo ratings yet
- Medication: Expected Pharmacological Action Therapeutic UseDocument1 pageMedication: Expected Pharmacological Action Therapeutic UseNatalia SpencerNo ratings yet
- Icu Guideline: Management of Diarrhea: StartDocument1 pageIcu Guideline: Management of Diarrhea: StartGracia VionaNo ratings yet
- ITF IPC COVID19 Overview - UPDATED - 7.27.21Document27 pagesITF IPC COVID19 Overview - UPDATED - 7.27.21Beugh RiveraNo ratings yet
- Sonoma County Superintendents Joint LetterDocument5 pagesSonoma County Superintendents Joint LetterKayleeNo ratings yet
- Anosh Ahmed Resignation LetterDocument1 pageAnosh Ahmed Resignation LetterKelly BauerNo ratings yet
- Vaccine FormDocument56 pagesVaccine FormPamela PatawaranNo ratings yet
- Spoon Fed - Why Almost Everything We've Been Told About Food Is Wrong - Tim SpectorDocument30 pagesSpoon Fed - Why Almost Everything We've Been Told About Food Is Wrong - Tim SpectorFanny0% (1)
- SRM Trichy Arts and Science College Vaccinated Detail As On 31.08.2021 Iii BbaDocument6 pagesSRM Trichy Arts and Science College Vaccinated Detail As On 31.08.2021 Iii BbaVignesh SNo ratings yet
- Covid 19Document31 pagesCovid 19Lee BuelaNo ratings yet
- Displacement StrategyDocument2 pagesDisplacement StrategyHary PowlyNo ratings yet
- CAPIZ - COVID-19 List of SDO Personnel VaccinatedDocument59 pagesCAPIZ - COVID-19 List of SDO Personnel VaccinatedJL D. BusiaNo ratings yet
- Lesson 5 - Designing SlidesDocument57 pagesLesson 5 - Designing SlidesTrương Quang TườngNo ratings yet
- C Ovid Case 19 ManagementDocument94 pagesC Ovid Case 19 ManagementMaria Allen Ann CasilihanNo ratings yet
- 10 Tips Healthy LifestyleDocument2 pages10 Tips Healthy LifestyleManwa LoverNo ratings yet
- SSC English Test Papers 2023Document114 pagesSSC English Test Papers 2023mushfik arafat100% (1)
- Sema4 COVID 19 FAQDocument2 pagesSema4 COVID 19 FAQEduardo MongeNo ratings yet
- Traveller GreeceDocument2 pagesTraveller GreeceElefteriosNo ratings yet
- Originating Application: The Administrative and Constitutional Law and Human Rights National Practice AreaDocument27 pagesOriginating Application: The Administrative and Constitutional Law and Human Rights National Practice AreaEdvin GarcíaNo ratings yet
- Impact On Indian Economy Due To Covid 191Document95 pagesImpact On Indian Economy Due To Covid 191kajal100% (3)
- 2021-09-25 - Masks Optional 3 CountiesDocument2 pages2021-09-25 - Masks Optional 3 CountiesActionNewsJaxNo ratings yet
- CV MMiller FinalDocument3 pagesCV MMiller Finalmiller1755No ratings yet
- Rws q3 Module 1 Shs Reading and Writing SkillsDocument25 pagesRws q3 Module 1 Shs Reading and Writing SkillsRose Ann Baste Bali-osNo ratings yet
- A Group of Homoeopathic Medicines For COVID 19: A Systematic Review of Clinical FeaturesDocument18 pagesA Group of Homoeopathic Medicines For COVID 19: A Systematic Review of Clinical FeaturesY.rajuNo ratings yet
- Class Six HarmonisedDocument34 pagesClass Six Harmonisedchimène olleNo ratings yet
- Eng-RWS-Q1 - Module-1 - Patterns of Written Text Across DisciplinesDocument26 pagesEng-RWS-Q1 - Module-1 - Patterns of Written Text Across Disciplinesmrp2983saonoyNo ratings yet
- EAPP Exam Q1Document6 pagesEAPP Exam Q1miniriftyNo ratings yet
- 1 s2.0 S0924857920302338 MainDocument2 pages1 s2.0 S0924857920302338 MainReginaJacobNo ratings yet
- Health FormDocument2 pagesHealth FormChristine BacordoNo ratings yet
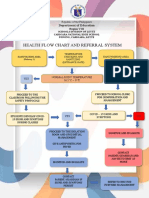
- Health Flow Chart and Referral System: Department of EducationDocument2 pagesHealth Flow Chart and Referral System: Department of EducationWendy TablaNo ratings yet
- W1-GR10 Math10 - q1 - Mod1 - PatternsSequences - V3b-FinalDocument24 pagesW1-GR10 Math10 - q1 - Mod1 - PatternsSequences - V3b-FinalRELABECARONo ratings yet
- ABOQUE, PAUL JOSHUA V. (ART APP ACT.6 Week 7)Document2 pagesABOQUE, PAUL JOSHUA V. (ART APP ACT.6 Week 7)Pj ValeNo ratings yet
- Class Viii MDP PDFDocument2 pagesClass Viii MDP PDFAnshu SahuNo ratings yet