You might also like
- APC Pharmacy Intern Written Exam SampleDocument62 pagesAPC Pharmacy Intern Written Exam SampleDaisy Lu81% (16)
- Ashhad's Step 2 CK UW Notes PDFDocument166 pagesAshhad's Step 2 CK UW Notes PDFabNo ratings yet
- Respiratory MedicationsDocument18 pagesRespiratory Medicationsapi-338095748No ratings yet
- Arsuri Burns ENGDocument82 pagesArsuri Burns ENGRomanescu RalucaNo ratings yet
- SNAKE BITE MEDICAL MANAGEMENT CrebonDocument33 pagesSNAKE BITE MEDICAL MANAGEMENT Crebonbayu riko100% (1)
- Intro To HematologyDocument9 pagesIntro To HematologyDayledaniel SorvetoNo ratings yet
- Care of The Older Adult Handouts PrelimsDocument7 pagesCare of The Older Adult Handouts PrelimsAmanda Joy TuizaNo ratings yet
- Danger Signs of PregnancyDocument3 pagesDanger Signs of PregnancyNesly Khyrozz LorenzoNo ratings yet
- Medical Data Base Bahrain 2018Document122 pagesMedical Data Base Bahrain 2018Shibu KavullathilNo ratings yet
- Nutritional Management of Burn Injury PDFDocument11 pagesNutritional Management of Burn Injury PDFMuhammad Arief BudimanNo ratings yet
- Asthma: Prepared by Fatima Hirzallah RN, MSN, CNS, PHDDocument21 pagesAsthma: Prepared by Fatima Hirzallah RN, MSN, CNS, PHDناصر دويكاتNo ratings yet
- Burns CH 25 n-7Document7 pagesBurns CH 25 n-7Jessica VargasNo ratings yet
- Neuro Vital Signs: Special RotationDocument6 pagesNeuro Vital Signs: Special RotationJamaica LimejuiceNo ratings yet
- Approach To Patient With Burn (S) : No Blisters Swollen and Blistered Whitish or Charred (Black)Document6 pagesApproach To Patient With Burn (S) : No Blisters Swollen and Blistered Whitish or Charred (Black)Suthar Keval CNo ratings yet
- Case Presentation DengueDocument3 pagesCase Presentation DengueLindel Assley Turqueza100% (1)
- Rapid assessment vital for major burnsDocument8 pagesRapid assessment vital for major burnsHelena Meurial Hilkiah100% (1)
- Oxygenation QuizDocument3 pagesOxygenation QuizPOTENCIANA MAROMANo ratings yet
- First Aide 2023Document97 pagesFirst Aide 2023jrfdcafprescomNo ratings yet
- WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues PDFDocument423 pagesWHO Classification of Tumours of Haematopoietic and Lymphoid Tissues PDFAlejandra Arely López NegreteNo ratings yet
- SJT Practice Paper Large Print PDFDocument83 pagesSJT Practice Paper Large Print PDFRumaisha Nuha ZNo ratings yet
- Adrenal Crisis FinalDocument10 pagesAdrenal Crisis FinalAmanda Scarlet100% (1)
- 1 Anaphylaxis Anaphylaxis Is A Life-Threatening TypeDocument9 pages1 Anaphylaxis Anaphylaxis Is A Life-Threatening TypeCraigNo ratings yet
- Hypertension: Mayur BV BPH 3 Semester PSPHDocument29 pagesHypertension: Mayur BV BPH 3 Semester PSPHBijay Kumar MahatoNo ratings yet
- BurnsDocument9 pagesBurnsVincentus BinNo ratings yet
- BURNDocument35 pagesBURNSri Muliani IdrisNo ratings yet
- Management of Asthma ExacerbationDocument13 pagesManagement of Asthma ExacerbationAini Shofa HaniahNo ratings yet
- Classification of Burns Based On Depth CharacteristicsDocument2 pagesClassification of Burns Based On Depth CharacteristicsmexelleNo ratings yet
- Nursing Manag BURNDocument34 pagesNursing Manag BURNumi margi rahayuNo ratings yet
- Anti-Cholinergic Drugs and Cholinesterase InhibitorsDocument24 pagesAnti-Cholinergic Drugs and Cholinesterase InhibitorsKhalid I. Abdullah100% (1)
- NCP DIarrheaDocument8 pagesNCP DIarrheakamini ChoudharyNo ratings yet
- Humeral Fracture TreatmentDocument49 pagesHumeral Fracture TreatmentIcha Marissa SofyanNo ratings yet
- Pathophysiology of ObesityDocument1 pagePathophysiology of ObesityPoldo Josef AngeloNo ratings yet
- Types of Insulin PDFDocument3 pagesTypes of Insulin PDFRetno WulanNo ratings yet
- Cardiac ArrestDocument50 pagesCardiac ArrestAnju Radhika100% (1)
- Case StudyDocument23 pagesCase StudyFarah Jelimae BagniNo ratings yet
- Case Study Burn Injury - 11Document15 pagesCase Study Burn Injury - 11Evelyn MedinaNo ratings yet
- Brain TumorDocument50 pagesBrain TumorbudiNo ratings yet
- Transurethral Resection of the Prostate (TURP) ExplainedDocument23 pagesTransurethral Resection of the Prostate (TURP) ExplainedColeen Comelle HuertoNo ratings yet
- Au Di Minor Case Study Myasthenia GravisDocument17 pagesAu Di Minor Case Study Myasthenia Gravisapi-301816885No ratings yet
- Reteplase (MIRel)Document23 pagesReteplase (MIRel)Jhoann JamanilaNo ratings yet
- Stump CareDocument7 pagesStump CareirtazakazmiNo ratings yet
- Quiz For Burn ManagementDocument3 pagesQuiz For Burn Managementfarmasi_hmNo ratings yet
- A Drug Study On: EpinephrineDocument16 pagesA Drug Study On: EpinephrineJay Jay JayyiNo ratings yet
- CATARACTSDocument2 pagesCATARACTSHanee Kaye TagubaNo ratings yet
- Tibial FractureDocument6 pagesTibial FractureKristene June Ilagan CoyamNo ratings yet
- Chest Injuries GuideDocument19 pagesChest Injuries GuideAbdi Kumala100% (1)
- Case Stydy Angina PectorisDocument46 pagesCase Stydy Angina PectorissharenNo ratings yet
- (Generic Name) ® Drotaverine 40mgDocument2 pages(Generic Name) ® Drotaverine 40mgSangar Sardar100% (1)
- SuturesDocument62 pagesSuturesShanmuga PriyaNo ratings yet
- Acute Myocardial InfarctionDocument20 pagesAcute Myocardial InfarctionDavid Christian CalmaNo ratings yet
- Running Head: A Patient Who Has Glaucoma 1Document10 pagesRunning Head: A Patient Who Has Glaucoma 1Alonso LugoNo ratings yet
- Drugs Study For PneumoniaDocument5 pagesDrugs Study For PneumoniaLucelle ArellanoNo ratings yet
- History and Assessment & Anatomy and Physiology of BurnsDocument10 pagesHistory and Assessment & Anatomy and Physiology of BurnsRina MaeNo ratings yet
- Initial Burn Assessment and CareDocument39 pagesInitial Burn Assessment and CareMudassir Mahboob KhattakNo ratings yet
- Pediatric Bronchitis Case PresentationDocument28 pagesPediatric Bronchitis Case PresentationJoshua DulayNo ratings yet
- Septic ArthritisDocument8 pagesSeptic ArthritisLorebell100% (2)
- 02 Bronchial Asthma Circ 2018-2019Document15 pages02 Bronchial Asthma Circ 2018-2019Mooha Alanzy100% (1)
- Bronchial Asthma (1) SKDocument24 pagesBronchial Asthma (1) SKSafoora RafeeqNo ratings yet
- Type and Indication of IV Therapy 2Document33 pagesType and Indication of IV Therapy 2Ruth Jazelle MendozaNo ratings yet
- CAP Pneumonia CaseDocument46 pagesCAP Pneumonia CaseMatty FelNo ratings yet
- EMERGENCY DRUGS: A Drug StudyDocument8 pagesEMERGENCY DRUGS: A Drug StudyShaine WolfeNo ratings yet
- Drug StudyDocument8 pagesDrug StudyJay-ar Batara SorianoNo ratings yet
- PT Case: Copd Exacerbation: DedicationDocument10 pagesPT Case: Copd Exacerbation: DedicationDianaLopezBorjaNo ratings yet
- Study Questions: Burn InjuriesDocument2 pagesStudy Questions: Burn InjuriesBELTRAN, JEANNE MAURICENo ratings yet
- Fracture at Right Femur Orif Case StudyDocument16 pagesFracture at Right Femur Orif Case StudyLouie ParillaNo ratings yet
- burnsDocument26 pagesburnsgemergencycareNo ratings yet
- Introduction To Burns: Bacteria VirusesDocument6 pagesIntroduction To Burns: Bacteria Virusesanon-50728No ratings yet
- Burns 2Document4 pagesBurns 2Charmae NaveaNo ratings yet
- Introduction To BurnsDocument47 pagesIntroduction To BurnsanushavergheseNo ratings yet
- Burns Are Most Common Household InjuriesDocument28 pagesBurns Are Most Common Household InjuriesSonu MishraNo ratings yet
- Project For Pre CalDocument1 pageProject For Pre CalPOTENCIANA MAROMANo ratings yet
- Nursing Care Plan for Open I Tibia Fibula (R) Lacerated LegDocument21 pagesNursing Care Plan for Open I Tibia Fibula (R) Lacerated LegPOTENCIANA MAROMANo ratings yet
- Earth Science Module Week 2 Assessment ToolDocument1 pageEarth Science Module Week 2 Assessment ToolPOTENCIANA MAROMANo ratings yet
- Our Lady of Fatima University: Level Year and Section FacultyDocument2 pagesOur Lady of Fatima University: Level Year and Section FacultyPOTENCIANA MAROMANo ratings yet
- Anemia: Our Lady of Fatima University College of NursingDocument21 pagesAnemia: Our Lady of Fatima University College of NursingPOTENCIANA MAROMANo ratings yet
- Eapp Module Activities Week 2Document5 pagesEapp Module Activities Week 2POTENCIANA MAROMANo ratings yet
- Lesson 1 What I Know: ActivityDocument3 pagesLesson 1 What I Know: ActivityPOTENCIANA MAROMANo ratings yet
- SSS Updates 2021 Webinar CertificateDocument1 pageSSS Updates 2021 Webinar CertificatePOTENCIANA MAROMANo ratings yet
- 6TH WELLNESS WEBINARS MaromaDocument1 page6TH WELLNESS WEBINARS MaromaPOTENCIANA MAROMANo ratings yet
- Concept Map of Reading StrategiesDocument2 pagesConcept Map of Reading StrategiesPOTENCIANA MAROMANo ratings yet
- Abing, LN Cu 1 Lab L1Document8 pagesAbing, LN Cu 1 Lab L1POTENCIANA MAROMANo ratings yet
- Functions of The Digestive SystemDocument8 pagesFunctions of The Digestive SystemPOTENCIANA MAROMANo ratings yet
- Pending in Floor Pending in Wall Pictures: SizeDocument2 pagesPending in Floor Pending in Wall Pictures: SizeAshley Nicole CeloricoNo ratings yet
- Dialysis Disequilibrium Syndrome (DDS): Causes, Diagnosis and TreatmentDocument2 pagesDialysis Disequilibrium Syndrome (DDS): Causes, Diagnosis and TreatmentNathaniel SanchezNo ratings yet
- CV DrmuneerDocument5 pagesCV DrmuneeridrisgaroodNo ratings yet
- Neonatal Hypoglycemia 2Document6 pagesNeonatal Hypoglycemia 2Lalo LanNo ratings yet
- Headache Diagnosis and Treatment of 2609Document77 pagesHeadache Diagnosis and Treatment of 2609Reza Badruun Syahrul HakimNo ratings yet
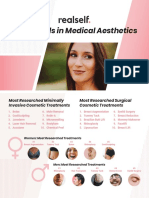
- RealSelf YearInReview OneSheetDocument2 pagesRealSelf YearInReview OneSheetDominico Adityo RaharjoNo ratings yet
- Cellular Regulation-BreastDocument41 pagesCellular Regulation-BreastMegan TurnerNo ratings yet
- Case Study On Acute Gastroenteritis and Acid Peptic-2Document15 pagesCase Study On Acute Gastroenteritis and Acid Peptic-2FHAMITHANo ratings yet
- PCOS PathophysiologyDocument2 pagesPCOS PathophysiologyMegaNo ratings yet
- Unas Agustus 2017Document18 pagesUnas Agustus 2017Dewi Arianti BudiantoNo ratings yet
- Caso Clinico 5Document5 pagesCaso Clinico 5Manuel IbarraNo ratings yet
- Pilonidal SinusDocument3 pagesPilonidal SinusHaddani FozaNo ratings yet
- Immunization Verification Form 2018Document2 pagesImmunization Verification Form 2018Jawad JamilNo ratings yet
- Micp211-1st WeekDocument3 pagesMicp211-1st WeekAlyanna TiglaoNo ratings yet
- Hip DislocationDocument39 pagesHip DislocationJordan Garcia Aguilar0% (1)
- Index BurgerDocument8 pagesIndex BurgerWasim ChaudhryNo ratings yet
- MAPEH VI Lesson on ImmunizationDocument3 pagesMAPEH VI Lesson on ImmunizationEsteban JuanNo ratings yet
- PSN Endometriosis Nov 15 SD Feb 19Document56 pagesPSN Endometriosis Nov 15 SD Feb 19lili mursidaNo ratings yet
- Odds Ratio Calculations for Disease ExposureDocument4 pagesOdds Ratio Calculations for Disease ExposureJoshMatthewsNo ratings yet
- Vital Sign RubricDocument2 pagesVital Sign RubricFrank CuvinNo ratings yet
- Potassium Chloride - Uses, Dosage & Side EffectsDocument4 pagesPotassium Chloride - Uses, Dosage & Side EffectsKenneth Mark B. TevesNo ratings yet