You might also like
- Lung Cancer (Nursing Care)Document5 pagesLung Cancer (Nursing Care)heiyuNo ratings yet
- Neck DissectionDocument24 pagesNeck Dissectionhayat al akoumNo ratings yet
- Online LectureDocument9 pagesOnline LectureJobelle AcenaNo ratings yet
- An Overview of PTBDocument5 pagesAn Overview of PTBJb_Abarado_7467No ratings yet
- Learning Material RLE NCM 112Document5 pagesLearning Material RLE NCM 112shiro the catNo ratings yet
- Lung CancerDocument41 pagesLung CancerchrstiannNo ratings yet
- Chest Physiotherapy With Sputum CollectionDocument41 pagesChest Physiotherapy With Sputum CollectionEduardNo ratings yet
- Scribd 020922 Case Study-Oncology A&kDocument2 pagesScribd 020922 Case Study-Oncology A&kKellie DNo ratings yet
- Infectious and Inflammatory DisordersDocument84 pagesInfectious and Inflammatory DisordersMariel OracoyNo ratings yet
- Common Abdominal Surgeries: Prof. (DR.) Md. Jawed AktherDocument21 pagesCommon Abdominal Surgeries: Prof. (DR.) Md. Jawed AkthervarunNo ratings yet
- Care of Patients With Cancer of The LiverDocument20 pagesCare of Patients With Cancer of The LiverJumar Vallo ValdezNo ratings yet
- DiagnosisDocument12 pagesDiagnosisHCX dghhqNo ratings yet
- Fundamentals of Nursing BulletsDocument14 pagesFundamentals of Nursing BulletsFRIA DEMAISIPNo ratings yet
- Answers To Activity 4: Collaborative ManagementDocument3 pagesAnswers To Activity 4: Collaborative ManagementEsmareldah Henry SirueNo ratings yet
- OLA HA LecDocument4 pagesOLA HA LecBetina De JesusNo ratings yet
- Postoperative Care ConceptsDocument44 pagesPostoperative Care ConceptsMelisa ClaireNo ratings yet
- Stomach CancerDocument11 pagesStomach CancerJumar Vallo ValdezNo ratings yet
- 77case StudyDocument3 pages77case StudyTiffany AdriasNo ratings yet
- Lung Cancer Nursing Care Plan & ManagementDocument5 pagesLung Cancer Nursing Care Plan & ManagementsajisajeenanaseerNo ratings yet
- Pre-Operative Nursing CareDocument79 pagesPre-Operative Nursing CarePeter FrimpongNo ratings yet
- 4 - Post Operative Nursing ManagementDocument38 pages4 - Post Operative Nursing ManagementraghadNo ratings yet
- ChemotherapyDocument35 pagesChemotherapynikhl saulNo ratings yet
- Fundamentals of Nursing BULLETSDocument7 pagesFundamentals of Nursing BULLETSNiña Marie Lim QuitanNo ratings yet
- Nursing Diagnosis Impaired Gas ExchangeDocument7 pagesNursing Diagnosis Impaired Gas ExchangeZycon Rodney Ae'zecquel Gachallan50% (2)
- Women's Pneumonia ReportDocument9 pagesWomen's Pneumonia ReportNohaira SADANGNo ratings yet
- Bronchogenic CarcinomaDocument13 pagesBronchogenic Carcinomaloresita_rebongNo ratings yet
- HYSTERECTOMY Tuazon SapanDocument58 pagesHYSTERECTOMY Tuazon SapanMonette Abalos MendovaNo ratings yet
- Nursing The Icu PatientsDocument31 pagesNursing The Icu PatientsInnocentNo ratings yet
- Patient Care Lectures on Vital Signs, Oxygen TherapyDocument9 pagesPatient Care Lectures on Vital Signs, Oxygen TherapyRodel AgapitoNo ratings yet
- Care of critically ill patients in intensive careDocument40 pagesCare of critically ill patients in intensive careNancy SinghNo ratings yet
- Nursing Care for Patients with Restrictive Lung DisordersDocument17 pagesNursing Care for Patients with Restrictive Lung DisordersGeorgia De OcampoNo ratings yet
- Appendicitis 191217094731Document37 pagesAppendicitis 191217094731OloanNo ratings yet
- Patient Case Study on AppendicitisDocument19 pagesPatient Case Study on Appendicitisfarzaneh yeganehNo ratings yet
- Cancer of The EsophagusDocument12 pagesCancer of The EsophagusHayat AL AKOUMNo ratings yet
- Oncology NursingDocument89 pagesOncology NursingRennard Christian J. De PerioNo ratings yet
- Surgery Imp QuestionsDocument29 pagesSurgery Imp Questionsakshit bhambriNo ratings yet
- Urinary Tract TumorsDocument13 pagesUrinary Tract Tumors4D RAGUINI, Meeka EllaNo ratings yet
- Nursing and End-of-Life CareDocument26 pagesNursing and End-of-Life CareShafiq Ur RahmanNo ratings yet
- Esophageal Cancer InserviceDocument18 pagesEsophageal Cancer Inserviceapi-371785797No ratings yet
- Pneumonia Types and TreatmentDocument34 pagesPneumonia Types and TreatmentCathy ZapantaNo ratings yet
- Critical Care Nursing For ARDSDocument13 pagesCritical Care Nursing For ARDSanchemeysNo ratings yet
- Prophylactic Measures: Sneha Ganesh 2 Yr MbbsDocument25 pagesProphylactic Measures: Sneha Ganesh 2 Yr MbbsSneha GaneshNo ratings yet
- Fundamentals of Nursing Bullets (Nle & Nclex)Document32 pagesFundamentals of Nursing Bullets (Nle & Nclex)ulcNo ratings yet
- Fundamentals of Nursing BulletsDocument32 pagesFundamentals of Nursing BulletsCatherine G. BorrasNo ratings yet
- Pneumonia: Acute Lung Infection GuideDocument4 pagesPneumonia: Acute Lung Infection GuideMarie Kelsey Acena MacaraigNo ratings yet
- Cancer of The UterusDocument14 pagesCancer of The UterusDipti PunjalNo ratings yet
- Hesi Presentation: Medical Surgical Cases-Patient X Lung CancerDocument47 pagesHesi Presentation: Medical Surgical Cases-Patient X Lung CancerKen TokkNo ratings yet
- Nursing Care for Patients with Renal StonesDocument8 pagesNursing Care for Patients with Renal StonesAnonymous dquW2YmO7No ratings yet
- Lower Respiratory Study SheetDocument13 pagesLower Respiratory Study SheetJune Rhoades100% (2)
- Kedarsing Care PlanDocument9 pagesKedarsing Care PlanAmit BarveNo ratings yet
- Chest PhysiotherapyDocument13 pagesChest PhysiotherapyAlma Susan100% (1)
- Nursing Care Plan For Pleural EffusionDocument9 pagesNursing Care Plan For Pleural EffusionJoseph Angelo Fortuna Carmona100% (1)
- For Lung CancerDocument6 pagesFor Lung CancerMichael Jerome Parallag100% (3)
- Nursing Care Plan For Appendicitis Post OperativeDocument17 pagesNursing Care Plan For Appendicitis Post OperativeOkaRizukiramanNo ratings yet
- 4 - Post Operative Phase 1Document39 pages4 - Post Operative Phase 1ننن نننن100% (4)
- Lab 4 LRTI Part OneDocument27 pagesLab 4 LRTI Part OnenohaNo ratings yet
- Discharge Plan Patient Teaching Pleural Effusion CastleDocument6 pagesDischarge Plan Patient Teaching Pleural Effusion Castleapi-341263362100% (2)
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- 3BSN7 CHNRLE ACTIVITY7 SCORING AND IDENTIFYING HEALTH PROBLEM and PRIORITY SETTING OF COMMUNITY HEALTH NURSING PROBLEMDocument6 pages3BSN7 CHNRLE ACTIVITY7 SCORING AND IDENTIFYING HEALTH PROBLEM and PRIORITY SETTING OF COMMUNITY HEALTH NURSING PROBLEMJumar Vallo ValdezNo ratings yet
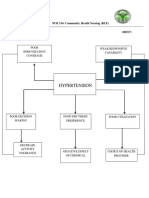
- Hypertension: NUR 154-Community Health Nursing (RLE)Document2 pagesHypertension: NUR 154-Community Health Nursing (RLE)Jumar Vallo ValdezNo ratings yet
- 3BSN7 Chnrle Activity9 2community Program Based Health Plan and EvaluationDocument3 pages3BSN7 Chnrle Activity9 2community Program Based Health Plan and EvaluationJumar Vallo ValdezNo ratings yet
- Care of Patients With Cancer of The LiverDocument20 pagesCare of Patients With Cancer of The LiverJumar Vallo ValdezNo ratings yet
- Care of Patients With CancerDocument21 pagesCare of Patients With CancerJumar Vallo ValdezNo ratings yet
- Care of Patients With Cancer of The ThyroidDocument17 pagesCare of Patients With Cancer of The ThyroidJumar Vallo ValdezNo ratings yet
- Stomach CancerDocument11 pagesStomach CancerJumar Vallo ValdezNo ratings yet
- Chronic Pain SAQ'sDocument52 pagesChronic Pain SAQ'sNaser AhmedNo ratings yet
- AComprehensive Algorithm For Management of Neuropathic Pain PDFDocument15 pagesAComprehensive Algorithm For Management of Neuropathic Pain PDFSussan AguedoNo ratings yet
- Removing Painful Stimuli to Promote ComfortDocument13 pagesRemoving Painful Stimuli to Promote ComfortCzarina Mae Quinones TadeoNo ratings yet
- Tramadol and Related ProductsDocument63 pagesTramadol and Related ProductsWrhaeyna MarieNo ratings yet
- Nursing-Practice IIIDocument17 pagesNursing-Practice IIIJean AustenNo ratings yet
- Operant Learning Theory in Pain and Chronic Pain RDocument11 pagesOperant Learning Theory in Pain and Chronic Pain RRhea AquinoNo ratings yet
- First-Trimester Pregnancy Termination - Uterine Aspiration - UpToDate PDFDocument30 pagesFirst-Trimester Pregnancy Termination - Uterine Aspiration - UpToDate PDFGLORIA ANDREA ORJUELA FLOREZNo ratings yet
- Auricular Acupuncture For Pain PDFDocument14 pagesAuricular Acupuncture For Pain PDFDerek Doran100% (1)
- Jay Spina: Presentencing DocumentDocument31 pagesJay Spina: Presentencing DocumentTony OrtegaNo ratings yet
- Intr Oduction: Classification of PainDocument4 pagesIntr Oduction: Classification of Painanimesh panda100% (1)
- Student Test of PainDocument7 pagesStudent Test of PainhumaNo ratings yet
- ThesisDocument140 pagesThesisPrem LathaNo ratings yet
- Acute Care Final Reflective JournalDocument3 pagesAcute Care Final Reflective Journalapi-328315559No ratings yet
- Test Bank For Pharmacotherapeutics For Advanced Practice 3rd Edition Virginia Poole ArcangeloDocument7 pagesTest Bank For Pharmacotherapeutics For Advanced Practice 3rd Edition Virginia Poole Arcangelosilasham3h8fNo ratings yet
- QC Kinetix (Aurora)Document1 pageQC Kinetix (Aurora)ScottHootsNo ratings yet
- Oral Oxycodone For Acute Postoperative PainDocument20 pagesOral Oxycodone For Acute Postoperative PainArmi ZakaNo ratings yet
- A Cochrane Review of Superficial Heat or ColdDocument9 pagesA Cochrane Review of Superficial Heat or ColdIvanFierroNo ratings yet
- Mixed Pain DR Novi Irawan SPSDocument25 pagesMixed Pain DR Novi Irawan SPSnovi irawanNo ratings yet
- Analgesic Efficacy of Erector Spinae Plane BlocksDocument7 pagesAnalgesic Efficacy of Erector Spinae Plane BlocksAlejandra SanchezNo ratings yet
- Analgesic ClassificationDocument4 pagesAnalgesic Classificationvie_apt6299No ratings yet
- Post Operative Pain Management in Elderly Patients: Alketa Dervishi, Kiri ZallariDocument3 pagesPost Operative Pain Management in Elderly Patients: Alketa Dervishi, Kiri ZallarianuradhaNo ratings yet
- A Systematic Review With Procedural Assessments and Meta-Analysis of Low Level Laser Therapy in Lateral Elbow Tendinopathy (Tennis Elbow)Document15 pagesA Systematic Review With Procedural Assessments and Meta-Analysis of Low Level Laser Therapy in Lateral Elbow Tendinopathy (Tennis Elbow)vitorpindaNo ratings yet
- Oncology Nursing CareDocument18 pagesOncology Nursing CareMichael Urrutia100% (1)
- RSIA MUTIARA BUNDA HIGH ALERT MEDICATION LISTDocument1 pageRSIA MUTIARA BUNDA HIGH ALERT MEDICATION LISTsuherti100% (1)
- Physiotherapy Belfast - Apex Clinic BrochureDocument2 pagesPhysiotherapy Belfast - Apex Clinic BrochureApexclinicNo ratings yet
- NCP Acute Abdominal PainDocument5 pagesNCP Acute Abdominal Painrachel_depalog82% (34)
- WHO Analgesic LadderDocument2 pagesWHO Analgesic LadderAndi PakdheeNo ratings yet
- The World Health Organization Three-Step Analgesic LadderDocument2 pagesThe World Health Organization Three-Step Analgesic LadderRisti FishyNo ratings yet
- PASSMEDICINE MCQs-PALLIATIVE CAREDocument22 pagesPASSMEDICINE MCQs-PALLIATIVE CAREImran Chaudhry100% (3)
- Willy Halim, MD, PHD, Fipp Anesthesiologist-Pain PractitionerDocument93 pagesWilly Halim, MD, PHD, Fipp Anesthesiologist-Pain PractitionerDManestesi cokicokiNo ratings yet