Professional Documents
Culture Documents
FX de La Cabeza Del Radio Cirugia y Terapia
Uploaded by
Eduardo RodriguezOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
FX de La Cabeza Del Radio Cirugia y Terapia
Uploaded by
Eduardo RodriguezCopyright:
Available Formats
SCIENTIFIC/CLINICAL ARTICLES
JHT READ FOR CREDIT #022
Radial Head Fractures—Advanced Techniques
in Surgical Management and Rehabilitation
Kraig Y. Bano, MPT, CHT ABSTRACT: Radial head fractures are the most common frac-
y tures in the elbow, and the treatment of nondisplaced fractures is
Hand & Upper Extremity Center
often straightforward. However, radial head fractures with concur-
PRO Physical Therapy rent injury to the elbow stabilizers may require complex treatment
Newark, Delaware and therapy that are targeted at specifically restoring elbow stabil-
Main Line Hand Center ity. This treatment of complex radial head fractures has recently
Exton, Pennsylvania improved because of long-term follow-up studies, increased bio-
mechanical research on elbow stability, and improved surgical
techniques. With an open line of communication between the sur-
Randeep S. Kahlon, MD, FACS geon and the therapist, an appropriate therapy plan can be initi-
Orthopaedic Trauma Service ated to protect both simple and complex injuries. The therapist
should have knowledge of specific tissue healing and treatment
ChristianaCare techniques, and the patient must be educated in possible out-
Wilmington, Delaware comes, safe arcs of motions, positioning, and proper splint use.
School of Physical Therapy This article summarizes current advanced techniques in the surgi-
cal management and rehabilitation of radial head fractures. Com-
University of Delaware
prehensive protocols for decision making and treatment are
Newark, Delaware introduced for both simple and complex radial head fractures.
First State Orthopaedics J HAND THER. 2006;19:114–36.
Wilmington, Delaware
Radial head fractures are the most common fractures of radial head fractures to be that of Paul of Aegina
in the elbow.1 Treatment of nondisplaced fractures can (AD 625–690) in his description of fractures of the
often be straightforward, but the associated injuries lower arm.2 In 1897, Helserich was the first to rec-
seen in both nondisplaced and displaced radial head ommend radial head resection for late deformity.
fractures greatly influence decision making about ap- Hammond in 1910 recognized the role of radiology
propriate and reasonable intervention choiczes. in the diagnostic workup and also recommended
Major progress in the management of these fractures excision of the radial head or displaced fragments.3
has been in part attributed to information gained Watson-Jones, in 1930, noted only 50% good results
from long-term follow-up studies on radial head exci- for displaced fractures and also noted that radial
sions, new biomechanical research studies on elbow head excision leads to radial shortening and/or ulnar
stability, and improved surgical techniques. As the sur- dislocation.4 During this time, many authors advo-
gical management of radial head fractures has evolved, cated a range of treatments involving nonoperative
treatment interventions for therapy have similarly treatment, fragment excision, head excision, manipu-
been modified and improved. This article summarizes lation, and tendon reconstruction for angulation.
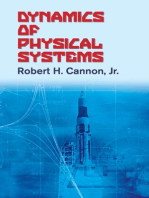
current advanced techniques in the surgical manage- In 1954, Mason put forth a classification system
ment and rehaabilitation of radial head fractures. based on his review of 100 patients5 (Figure 1). Type I
fractures were nondisplaced and did well with non-
operative treatment. Type II fractures, which he
HISTORICAL BACKGROUND called ‘‘marginal sector fractures,’’ were displaced
and had varying results. If the fragment was less
A comprehensive summary of the literature by
than 25% of the articular surface, he recommended
Schwartz and Young documented the first description
nonoperative treatment. Fragment excision was re-
y
Affiliation at the time manuscript was created. served for larger fragments, and head excision was
reserved for head tilting or fracture comminution.
Correspondence and reprint requests to Kraig Y. Bano, MPT, CHT,
Main Line Hand Center, 495 Thomas Jones Way, Suite 204, Exton, Type III fractures were comminuted and he advised
PA 19341; e-mail: <kbano25@hotmail.com>. early excision. (Note that none of his patients under-
doi:10.1197/j.jht.2006.02.011 went open reduction internal fixation [ORIF].)
114 JOURNAL OF HAND THERAPY
‘‘complex or complicated.’’8 This allowed for treat-
ment of simple fractures based on the Mason classifi-
cation and allowed for treatment of the complex
injuries based on the associated injury. As the Mayo
classification is the most current and inclusive classi-
fication, it will be used in this article.
An important distinction should be noted regard-
ing the terminology of ‘‘simple’’ or ‘‘complex.’’ This
article focuses on radial head fractures, but simple or
complex are also often used in classification of elbow
dislocations. When used in reference to radial head
fractures, the two terms denote an associated injury
with the radial head fracture. However, when used
FIGURE 1. Mason classification of radial head fractures. in reference to elbow dislocations (without radial
(Reprinted with permission from Green’s Operative Hand
Surgery, 5th ed. Philadelphia, PA: Elsevier, 2005) head fracture) the two terms denote whether the
dislocation is reducible and whether the dislocation
can be maintained without surgery.
Subsequently, as attempts at ORIF increased and
In 1941, Speed was the first to consider prosthetic
improved, many Mason II fractures were reclassified
replacement (metal) in lieu of excision for commi-
intraoperatively into Mason III because the severity
nuted fractures.9 Silicone replacement was champ-
of radial head fracture comminution is usually un-
ioned by Swanson and others at a later date. The
derappreciated on the preoperative films. Johnston
Swanson silicone radial head implant went on to be-
added a type IV fracture category in 1962, described
come the most-used implant worldwide for these
as radial head fracture with elbow dislocation, and
fractures.10 Long-term follow-up studies of patients
noted that primary radial head excision was not a be-
with silicone arthroplasty, however, have revealed
nign procedure.6 Since that time, increasing research
problems with implant wear, implant failure, and sil-
into elbow anatomy and biomechanics, in addition to
icone synovitis.11,12 Other materials used for arthro-
advances in ORIF techniques and instruments, has
plasty have included acrylic, ultra-high molecular
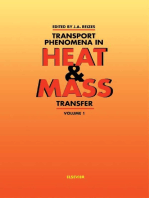
greatly advanced operative techniques. Hotchkiss,
weight polyethylene, ceramics, and various metals.
in 1997, modified the Mason classification by adding
Arthroplasty with metallic implants is the current
specific displacement guidelines and classifying type
state of the art, and recent advances have been cen-
II fractures as those that are repairable and type III
tered on bipolar designs and modular designs.13
fractures as those that are not repairable7 (Figure 2).
Morrey advocated an additional level of classification
(termed the Mayo classification) in which isolated ra- ANATOMY AND BIOMECHANICS
dial head fractures were ‘‘simple or uncomplicated,’’
whereas radial head fractures associated with an- A complete discussion of elbow biomechanics (see
other elbow fracture or ligament injury were termed the article in this issue by Lockard) is beyond the
HOTCHKISS CLASSIFICATION OF PROXIMAL RADIAL FRACTURES*
Type I
• Nondisplaced or minimally displaced fracture of head or neck
• No mechanical block to rotation
• Displacement less than 2 mm or a marginal lip fracture
Type II
• Displaced (usually > 2 mm) fracture of head or neck (angulated)
• May have mechanical block to motion or be incongruous
• Without severe comminution (technically possible to repair by open reduction and
internal fixation)
• More than a marginal lip fracture of the radial head
Type III
• Severely comminuted fracture of the radial head or neck
• Judged not reconstructable on basis of radiographic or intraoperative appearance
• Usually requires excision for movement
*All of these fractures may have associated injuries such as a coronoid fracture, elbow dislocation, or medial collateral or
interosseus ligament tears. From Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision. J Am
Acad Orthop Surg 5:1-10, 1997.
FIGURE 2. Hotchkiss classification of radial head fracture.
April–June 2006 115
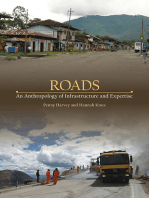
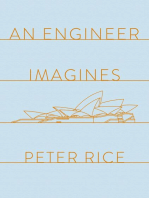
scope of this article; however, some basics are rele- anterolateral corner of the radial head articular disk
vant. The proximal radio-ulnar joint (PRUJ) is highly (Figure 4). This stress is followed in sequence by the
congruent and accounts for approximately 60–70° of lateral and then the medial elbow ligament support-
the articular surface of the radial head. The corre- ing structures, consistent with a PL rotation of the
sponding safe zone is an arc of 110° where hardware joint. With this progression, dislocations of the elbow
can be placed without impinging in the radial notch occur in approximately 5–10% of radial fractures.1,6,19
during forearm rotation14,15 (Figure 3). Because of the Dislocations can often present with coronoid frac-
elliptical nature of the radial articular disk, there is a tures of varying severity. Thus, the ‘‘terrible triad’’
slight radial/ulnar translation of the head and this is is a radial head fracture, a coronoid fracture, and dis-
accentuated in pronation. location of the elbow (with the obligatory disruption
The lateral collateral ligament (LCL) is an impor- of at least one of the collateral ligaments).20
tant stabilizer against posterolateral (PL) instability.16 A concomitant LCL injury creates PL instability
This is an important factor in assessing the soft tissue and may indicate an occult elbow subluxation.
component of the injury laterally, but it also dictates a Commonly, the anterolateral wedge fracture off the
cautious surgical approach. The traditional Kocher radial head is the result of a partial PL subluxation
approach may actually violate the LCL; thus, a more and the LCL should be addressed concurrently if the
midaxial approach is recommended to avoid iatro- radial head is being treated operatively.1
genic LCL detachment and the sequelae of late failure Amis and Miller have shown that the radial head is
and residual pain. The surgical incision (in the deep selectively fractured in increasing elbow flexion.21
musculotendinous layer) should be limited to the The coronoid process is at highest risk between 0
anterior one-half of the radiocapitellar joint (RCJ) in and 35° of elbow flexion in FOOSH, whereas the ra-
order to spare the LCL and maintain PL stability. dial head is at risk between 0 and 80° of flexion.
The radial head is an important elbow stabilizer to Depending on the size of the coronoid fracture, elbow
valgus stress.17 Lack of the lateral column support instability may be the actual major issue and the ra-
(provided by the radial head) significantly increases dial head fracture may just be a marker of this injury.
physiologic stress borne by the medial collateral liga- Additionally, in the lateral compartment, capitellum
ment (MCL). In one study, tension stress seen by the fractures occur at a rate of 24% with displaced, oper-
MCL with an absent radial head reached as high as ative radial head fractures.22
33 the body weight.18 A concurrent MCL injury Medial collateral ligament injuries have been asso-
with radial head comminution creates an instant val- ciated with radial head fracture severity. Mason type
gus instability and predisposes to significant long- I fractures have associated MCL injuries less than 5%
term sequelae. of the time, whereas type II show an incidence of
approximately 50% and type III approximately
MECHANISM AND ASSOCIATED
INJURIES
A fall on an outstretched hand (FOOSH) with the
hand/forearm in pronation accounts for the large
majority of radial head fractures. The axial load upon
the elbow (with the hand pronated) stresses the
FIGURE 3. Proximal radio-ulnar joint rotation—note the FIGURE 4. Anterolateral radial head at risk. (Illustration
high congruency of the joint and the ‘‘safe zone’’ for fixa- by Elizabeth Roselius Ó 2005. Reprinted with permission
tion. (Reprinted with permission from Green’s Operative from Green’s Operative Hand Surgery, 5th ed. Philadel-
Hand Surgery, 5th ed. Philadelphia, PA: Elsevier, 2005) phia, PA: Elsevier, 2005)
116 JOURNAL OF HAND THERAPY
87%.23 As previously mentioned, there is significant of the radial column to maintain radial length, either
increasing tensile stress for the MCL in the absence by ORIF or by radial head arthroplasty.25
of an intact radial column. MCL insufficiency can Furthermore, the distal ulna should be closely ob-
present acutely in this circumstance but also can pre- served for dorsal instability and may require supina-
sent much later secondary to chronic MCL overload- tion splinting to immobilize the DRUJ in a
ing from the prolonged absence of radial column concentrically reduced alignment. In reviewing the
support. This delayed or secondary presentation of Mayo experience, Trousdale et al. noted 80% satisfac-
valgus instability often contributes to the develop- tory results when the Essex-Lopresti injury was recog-
ment of tardy ulnar nerve palsy. nized and treated appropriately versus only 14%
The initial evaluation of any radial head fracture satisfactory results for late detection and subsequent
should also include a wrist examination, particularly attempts at reconstruction.26
the distal radio-ulnar joint (DRUJ), to rule out
an Essex-Lopresti injury. This entity occurs when
the radial head fracture has an associated tear of INTERVENTION OPTIONS
the interosseous membrane (IOM) with possible tri-
angular fibrocartilage (TFCC) injury and possible As with any fracture, management of radial head
DRUJ instability. Axial forces in the forearm are fractures should be based on both patient factors and
distributed 80% radius/20% ulna at the wrist but injury-specific factors. Patient factors include age,
change to 40% radius/60% ulna at the elbow.24 In or- bone quality, (non-elbow) associated injuries, and
der to accomplish this transfer of load from the distal activity level. Injury-specific factors include fracture
radius to the proximal ulna, three structures are essen- size, displacement, rotation block, and associated
tial: the radial head, the IOM, and the DRUJ ligaments. bony and ligament injuries (Table 1).
Thus, with radial head fractures, the IOM and DRUJ Initial management of a radial head fracture with
become the remaining forearm axial stabilizers and elbow dislocation involves a gentle reduction (under
are at risk for rupture in the more severe radial head conscious intravenous sedation) followed by repeat
injury patterns (Figure 5). In order to prevent radial radiographs to determine the success of the reduc-
shortening of 5–10 mm and ulnocarpal impaction tion. The initial radiographs, and any postreduction
syndrome, recognition of this injury requires repair radiographs, should be carefully assessed for associ-
ated fractures or displacement that may suggest a
complex injury or unstable elbow. Further evaluation
by computed tomography with three-dimensional
reconstructions can be helpful to evaluate associated
injuries, as plain radiographic studies (x-rays) do not
adequately reflect the amount of comminution
(Figure 6).
Nonoperative management with early active range
of motion is best used following type I and stable type
II fractures.7 This includes nondisplaced or mini-
mally displaced fractures without a rotation block
(Figures 7A and 7B). If a mechanical block to rotation
is noted, aspiration of the elbow hemarthrosis with
injection of local anesthetic is used to assess forearm
rotation. Morrey reports that nonsurgical treatment is
appropriate for type II fractures when 20–140° of flex-
ion and 70° of forearm rotation in each direction are
available under anesthetic block.27 Early motion pro-
tocols are successful in these cases, with careful clin-
ical follow-up to observe any subsequent or late
displacement of the fracture fragment(s). Larger frag-
ments (greater than one third of the articular surface)
require close observation for late displacement.
Open reduction internal fixation is recommended
for type II fractures with significant displacement
($2 mm), large fragment size ($33%), or mechanical
FIGURE 5. Essex-Lopresti injury—note the injury of the block to motion.28,29 Radial neck fractures with
interosseous membrane and distal radio-ulnar joint. (Illus-
tration by Elizabeth Roselius Ó 2005. Reprinted with per- greater than 20° of angulation impede forearm rota-
mission from Green’s Hand Surgery, 5th ed. Philadelphia, tion at the PRUJ, and surgery should be considered.30
PA: Elsevier, 2005) In younger patients, we recommend ORIF for even
April–June 2006 117
TABLE 1. Treatment of Radial Head Fractures
Simple (aka Mason I–III, Hotchkiss Complex (aka Johnston type IV or
I–III, or Morrey Simple) Morrey/Mayo Complex)
I Non-op Early range of motion (ROM) 1. Same radial head protocol as for simple
II Non-op Early ROM types I–III
II Operative 1. Open reduction internal fixation (ORIF) 2. Radial head excision (without
Indications: 2. Fragment excision (rare) arthroplasty) is contraindicated. Radial
1. Rotational block 3. Radial head excision (limited to older head reconstruction is essential to elbow
2. Displacement $2 mm population without complex injury) stability
3. Large fragment ($33%) All followed by early ROM 3. Fix associated injuries:
4. Neck $20% angulation a. Coronoid fracture
(Assumes repair is possible, b. Lateral collateral ligament (LCL)
otherwise reclassify as type III) rupture
III Operative 1. Metallic arthroplasty (especially if older) c. Medial collateral ligament rupture
Usually comminuted 2. ORIF (especially if younger) d. Essex-Lopresti lesion
Some are irreparable 3. Radial head excision (limited to older e. Olecranon fracture
Consider locking plate population without complex injury) f. Global instability may require
Metallic prosthesis over silicone All followed by early ROM external fixator (or use to protect
repair of an associated injury)
All followed by early ROM (protected with
safe arc, splints, or braces as needed)
comminuted fractures that are difficult to fix so as to injuries, whether articular, ligamentous, or bony.
create an anatomic spacer (both to provide valgus sta- Stabilizing the proximal radius does provide signifi-
bility and to minimize proximal radial migration) cant stability to the unstable elbow, but augmentation
(Figures 8A–8D). Fixation techniques have improved with additional fixation for the associated injury may
tremendously over the last three decades and now in- still be needed. A congruous reduction and a stable
clude small subarticular compression screws, interos- fixation are prerequisites to allow early motion tech-
seous headless screws, plates, absorbable pins, niques (within days) and achieve successful results.
cannulated screws, threaded K-wires, and fixed Failure to achieve rigid, congruous fixation leads to
angle/locked plates. These improved fixation tech- persistent postoperative stiffness, pain, and, some-
niques have extended the indications for ORIF. Any times, ongoing articular damage on the corresponding
surgical approach to the radial head must carefully surfaces. Thus, if appropriate internal rigid fixation
preserve the LCL attachment and may also involve cannot be attained, an alternative treatment should be
repair of the LCL attachment if avulsed from the lat- used. Ultimately, the decision to repair, excise, or
eral epicondyle. Internal fixation should be limited to replace the head is an intraoperative decision.
the safe zone, as described above, to minimize rota- Radial head excision following fracture has an
tion block at the PRUJ. extensive but controversial history in the literature.
Stable internal fixation of the radial head is of Currently, radial head excision has a limited role in
significant value in complex fractures with associated the acute management of these injuries. Specifically,
FIGURE 6. Radial head fracture comminution seen better on computed tomography (CT): A and B, injury films with 3-D
reconstructions. Note the radial head comminution, posterior displaced head fragment, and adjacent anterior coronoid
fracture.
118 JOURNAL OF HAND THERAPY
FIGURE 7. Type I radial head fracture (A and B, injury films).
it is reserved for the simple comminuted type III stability). For all other cases, radial head excision
fracture in the older population (Figures 9A–9F). should be performed sparingly. Specifically, for the ir-
However, in complex acute injuries, there is signi- reparable radial head fracture or complex radial head
ficant evidence to show that isolated excision fracture with ligamentous instability, we prefer metal-
leads to failure and is difficult to reconstruct.26 lic arthroplasty replacement over excision. An early
Biomechanical studies have documented significant active range of motion program is then implemented
pathologic alterations in elbow kinematics after acute with expectations of early return of motion.
excision, and long-term studies show mixed clinical Radial head arthroplasty (or replacement) is indi-
results.31 Once the decision is made to excise the ra- cated for all irreparable fractures with associated
dial head, intraoperative stress examination of the injuries (all complex type III injuries) (Figures 10A–
MCL, IOM, and DRUJ should be documented. 10D). King et al. demonstrated that radial head re-
Excision thus should be reserved for those injuries placement restores elbow kinematics and enhances
in which the above stress testing fails to document elbow stability akin to the native radial head.13 He
any instability.32 Thus, we recommend early isolated recommends radial head arthroplasty for all irrepara-
radial head excision only for the simple comminuted ble fractures regardless of other associated injuries to
fracture in the older population (with ligamentous minimize the incidence of missed associated complex
FIGURE 8. Type II displaced radial head fracture (A, B, injury films; C, D, post-op at three months).
April–June 2006 119
FIGURE 9. Type III radial head fracture in a 62-year-old female (A–C, injury films. Note the displaced posterior fragment
in C preventing extension. D–F, post-op at three months. Note that in addition to the radial head excision, the displaced
posterior fragment has been excised in F restoring extension).
injuries. Recent improvements in prosthesis design Intraoperative stress testing after radial head recon-
allow for a more customized, modular fit and allow struction and LCL repair dictates the need for further
for easier implantation. adjunctive stabilization (such as MCL repair or
The management of complex radial head fractures external hinge fixation device). Because radial head
is directed at the associated injury/instability (the reconstruction with LCL repair alone often provides
elbow dislocation) in addition to the radial head a stable enough elbow for early range of motion,
fracture injury. Stabilization of the radial column (via additional stabilization is frequently not needed.
ORIF or replacement) is completed as indicated Essex-Lopresti lesions are best treated with radial
above and then is augmented with additional repairs head reconstruction and stabilization of the DRUJ,
as dictated by any persistent elbow instability. Large either by immobilization or by temporary DRUJ
coronoid fragments (especially the anteromedial pinning. In this instance, the mild loss of DRUJ
fragment, which is often missed) require stabilization pronation (seen sometimes with supination pinning)
for early range of motion (ROM). LCL injuries are is much preferable to the risk of dorsal distal ulna
repaired through the lateral approach as part of the instability (seen with untreated DRUJ injuries).
closure for the radial head treatment. If the repaired Olecranon fractures are fixed with rigid internal
elbow is not fully stabilized, the postoperative pro- fixation (preferably using the newer anatomically
tocol is adjusted accordingly to minimize radial head contoured olecranon plates rather than with the
subluxation in the early phases of recovery. traditional tension band technique) as this allows
120 JOURNAL OF HAND THERAPY
FIGURE 10. Complex type III radial head fracture in a 51-year-old male (A, B, injury films. C, D, post-op at three months.
Note the lateral collateral ligament repair with suture anchor in the lateral epicondyle).
earlier full ROM in therapy. Occasionally, in the face of a missed Essex-Lopresti lesion, whereas late pre-
of gross instability despite the above repairs (or to sentation of this wrist pain is likely secondary to ul-
protect the above repairs), hinged elbow external nar carpal arthrosis from proximal radial migration.
fixation is necessary to maintain a concentric elbow If this late ulnar carpal arthrosis (usually ulnar im-
reduction. If so, radial column fixation can be par- paction syndrome) is allowed to progress, there will
tially ‘‘unloaded’’ by the lateral nature of the frame be a significant wrist disability in all ROM. Studies
but cautious observation of lateral column compres- vary greatly as to the incidence of wrist pain
sive forces (that are often seen later upon frame and the severity of wrist pain after radial head oper-
removal) is obligatory. ative treatment with or without head excision.33,34
However, with the recent improvements in radial
head ORIF techniques and the increasing early recog-
COMPLICATIONS nition of these associated injuries, the previous stud-
ies discussing the incidence of wrist pain may require
Complications are found in both nonoperative and re-evaluation. Silicone synovitis and other failures of
operative treatment outcomes. Nonunion can occur silicone implants (axial failure, hardware breakage,
with any radial fracture, including type I nondis- etc.) are presenting in increasing frequency in long-
placed fractures. Asymptomatic nonunion does not term follow-up studies. Thus, currently, there are no
require treatment, but symptomatic nonunion can be indications for silicone arthroplasty.
addressed with either radial head excision or arthro- Heterotopic ossification occurs variably after radial
plasty, depending on any residual associated injuries. head excision, in delayed operative interventions,
Late displacement is treated in a similar manner, but and in head-injured patients.35 A patient with HO
close clinical observation is needed to prevent late who is asymptomatic is treated conservatively, and
degenerative changes. excisional treatment is recommended for sympto-
Additional complications include residual pain, matic patients willing to undergo extensive rehabili-
stiffness, failure of fixation, wrist pain, degenerative tation. With appropriate surgical, adjunctive, and
arthritis, silicone synovitis, and heterotopic ossifica- rehabilitation protocols, successful outcome in HO
tion (HO). Residual pain is multifactorial including cases can approach 75%.11 Surgical and rehabilitation
articular malalignment or occult instability. Wrist strategies are discussed in the Casavant and Hastings
pain occurring early after injury may be the result article in this issue; adjunctive interventions include
April–June 2006 121
perioperative radiation therapy and high-dose post- the Arm, Shoulder, and Hand questionnaire or the
operative nonsteroidal anti-inflammatory drugs to Patient-rated Elbow evaluation can help with goal
minimize HO recurrence. setting and to measure change in the patient over
With open and prompt communication between time. Patients’ reports of specific ADL, work, and lei-
the surgeon and the therapist, complications can be sure limitations are recorded. (These measures are
addressed appropriately. discussed further in the article by MacDermid and
Michlovitz in this issue.)
REHABILITATION Objective physical measures are taken during the
initial examination. These include edema measure-
Initial Evaluation after Radial Head Fractures ments, wound assessment, ROM, and strength.
Edema is measured by girth at specific landmarks
When beginning therapy with the patient who has or volumetry if the wounds are healed. When mea-
sustained a radial head fracture, it is important to suring girth around the elbow, using the epicondyles
obtain as much information about the injury and or joint line as landmarks gives more consistent re-
interventions as possible. The therapist should be in sults than using skin landmarks as bone position is
contact with the surgeon to obtain the following constant versus the mobility of skin. The ulnohum-
information: date and mechanism of injury, type of eral and radiohumeral joint lines are appreciated dis-
fracture, stability of fixation, type of intervention, any tal to the epicondyles. However, pain and edema may
concomitant injuries, and any limitations in ROM prevent the palpation of these bony landmarks.
due to joint instability. Knowledge of the intervention Circumferential tape measurement at the anterior el-
and outcome rendered by the surgeon is important in bow crease using the olecranon as a guide dorsally
developing a therapeutic plan. The mechanism of may be substituted. The angle of the elbow during
injury may reveal information regarding the intensity girth measurement should also be noted to maintain
of trauma and possibility of concomitant injuries to consistency for a measuring point during subsequent
not only the elbow but also other body parts. Injuries measurements.
in other areas in the upper extremity such as the The wound should be thoroughly evaluated to
shoulder, wrist, hand, scapula, thorax, and lower ensure that the sutures are intact and that there is no
extremity alter the rehabilitation program. If there is evidence of infection. If a hinged external fixation
surgical intervention, information regarding the sta- device is used, the pins should be assessed similarly.
bility of the reduction, hardware type and location, Signs of infection include redness, edema, increased
repair or reconstruction of concomitant injuries, and skin temperature, discharge, odor, fever, and dehis-
quality of bone and ligaments involved is necessary cence of the wound. Pain with tapping of the pins
to develop an appropriate treatment plan for therapy. and loosening of the pins are possibly early indica-
Thus, the type of surgical intervention will dictate the tions of osteomyelitis. If these symptoms arise, it is
therapist’s plan of care and progression for treatment imperative to immediately contact the referring sur-
(Tables 2 and 3). geon. The skin surrounding the wound should be
Patient history includes the date and mechanism of thoroughly inspected for abnormalities such as mac-
injury, hand dominance, any previous upper extrem- eration or blistering. The size of the wound, integrity
ity injuries, and medical conditions that may affect of closure, adherence, and blanching with motion are
either healing or treatment. Activity of daily living noted. In general, there are rarely issues with the
(ADL) limitations, work requirements, and hobbies incisions.
are also identified. Details regarding the patient’s If instability of the elbow is present, the ROM limits
work status and timeline to return to work should be for the stable arc of motion should be obtained from
obtained. A job task description is obtained from the the surgeon before proceeding with the evaluation
place of employment to assist with goal setting and and treatment. Forearm rotation motion is measured
program development that may require intense work with the elbow in 90° of flexion. Passive elbow ROM
conditioning. Opportunities for light or modified measurements are deferred until appropriate to test.
duty are explored to allow the patient to transition ROM of uninvolved joints such as the shoulder and
back to the work environment earlier. Hobbies such wrist should be taken.
as crafts, musical instruments, and sports are taken Strength testing is not appropriate before the frac-
into account, and the patient’s personal goals are ture has healed; therefore, it is assessed later. When
discussed and incorporated into treatment planning. appropriate, testing is compared with the contralat-
Pain is assessed for location, type, quality, intensity, eral side, if deemed normal, via manual muscle
and behavior. A pain questionnaire, visual analog testing, dynamometer measurement, isotonic/isoki-
scale, or verbal rating scale is useful. The same scale netic testing, lift testing, or functional capacity
as that administered for the initial rating is used for evaluation.
the subsequent follow-up ratings to maintain consis- Sensory and motor function of the peripheral
tency. An outcome measure such as the Disability of nerves is also evaluated. The radial nerve is in close
122 JOURNAL OF HAND THERAPY
TABLE 2. Rehabilitation of Simple Radial Head Fractures
Weeks
Therapeutic
Intervention 0–2 2–4 4–6 6–8 8–12
Immobilization ,10 days
Splinting for Begins immediately
protection May continue until
three to six weeks
following injury or
surgery
Edema control Begins immediately
Continues
throughout
rehabilitation
Pain control Begins immediately
Continues throughout
rehabilitation
Scar management Begins three to four
weeks after
surgery, following
wound closure and
suture removal
Early active/active Begins as early as
assisted range of pain and edema
motion (ROM) allow
Usually less than
ten days
Stable ROM
Pain-free ROM
Also include
uninvolved joints
Passive range of Begins gentle,
motion avoiding soft
tissue injury
Stable range only
Joint mobs Begins three to four
weeks after injury
or surgery
Requires proper bone
healing
Needs to be stable
Splinting for motion Static, static
progressive,
or dynamic
splinting begins
Needs proper bone
healing
Strengthening Shoulder/scapular Isometric elbow PREs for all joints Strengthening Work conditioning
strengthening and exercises begin Pain-free ranges progressed as Include a total
isometric wrist at three to Needs proper bone tolerated body approach
exercises begin at four weeks healing
,2 weeks
proximity and can be damaged with radial head severe edema with pain out of proportion at the
fracture, dislocation, or surgical dissection. The ulnar forearm, compartment syndrome should be consid-
nerve in the cubital tunnel is susceptible to injury ered and the patient should be referred for immediate
with dislocation, medial epicondyle fracture, com- surgical evaluation.36
pression from immobilization devices, or tardy palsy Once a thorough evaluation is completed, an edu-
from prolonged valgus instability. In the case of cated assessment of the radial head fracture with
April–June 2006 123
TABLE 3. Rehabilitation of Complex Radial Head Fractures
Weeks
Therapeutic
Intervention 0–2 2–4 4–6 6–8 8–12
Immobilization ,10 days
after surgery
Splinting for Thermoplastic splint
protection immediately after
surgery up to six
weeks post-op
Hinged elbow splint
Locked at 90 between
exercise sessions
Blocked motion in
stable range
If unstable, forearm
held in either pron/
sup/neutral forearm
rotation to increase
stability
Pain and edema Begins immediately
control post-op
Continues throughout
rehab
Wound care Immediately post-op
Prevent infection
With external fixator,
includes pin care
Scar management Begins three to
four weeks
after surgery,
following
wound closure
and suture
removal
Early active/active Begins as early as pain
assisted ROM and edema allow
Usually less than ten
days
Stable ROM in hinged
splint with blocked
motion
Pain-free ROM
Also include
uninvolved joints
Forearm rotated for
maximum stability
Forearm motion only to
neutral for four to six
weeks if using a
rotated position to
stabilize
Avoid stressing injured
ligaments
(Continued)
124 JOURNAL OF HAND THERAPY
TABLE 3. Continued
Weeks
Therapeutic
Intervention 0–2 2–4 4–6 6–8 8–12
Passive range of Begins gentle,
motion avoiding soft
tissue injury
Stay in stable range
Avoid stretching/
stressing injured
structures or
increasing
instability
Joint mobs Begin joint mobs if
appropriate
Contraindicated
with instability,
especially with
excision,
arthroplasty,
and/or ligament
injury
Splinting for Static, static
motion progressive, and
dynamic splinting
may begin if
elbow is stable
Need proper bone
and ligament
healing
Avoid stressing
injured ligaments
Strengthening Shoulder/scapular Stable elbow Isometrics for the Wrist and elbow PREs begin if
strengthening and isometrics unstable elbow or PREs external fixator
isometric wrist begin at three to injured wrist In stable ROM involved
exercises begin at four weeks Pain-free ranges At 12–16 weeks,
,2 weeks Avoid causing begin work
damage conditioning as
appropriate
.12 weeks work
conditioning if
external fixator
involved
specific functional goals can be made. Then a treat- with normal pronation and supination at 80–90°
ment plan is developed and modified as necessary each.37,38 Contralateral ROM measurements, pre-
for the individual patient. suming that the elbow is not also injured, will define
the ideal goals, though functional and realistic goals
Goals for Rehabilitation may vary from this based on the severity of the injury.
Morrey et al. demonstrated that most ADL, demon-
Goals for therapy are based on integration of the strated by 15 tasks, could be achieved with 100° of
history of the injury, concurrent patient medical elbow motion (from 30° to 130°) and 100° of forearm
factors, and injury intervention with findings from rotation (from 50° pronation to 50° supination). They
the initial examination, assessment, and function also determined that all tasks were achieved in an arc
necessary for ADL, work, and hobbies. Returning to from 15° to 140° of elbow motion.39 Alternatively,
all functional activities, or at least maximizing func- Vasen et al., in a study of 12 tasks, demonstrated
tion, is the main goal of therapy. Maximal motion for that elbow motion from 75° to 120° could enable the
the elbow and forearm should be achieved without performance of all tested tasks and motion from 90°
compromising stability or damaging repaired struc- to 105° had minimal impairment.40 However, certain
tures. Normal ROM at the elbow is 0° of extension job duties may require more or less motion than that
(up to 10° of hyperextension) and 140–150° of flexion, identified by these authors. In these instances, the
April–June 2006 125
FIGURE 11. Examples of postinjury or postoperative splints to prevent forearm rotation. (A) A sugartong splint that limits
elbow extension and forearm rotation but allows elbow flexion. (B) A posterior long-arm splint including the elbow and
wrist that prevents both elbow and forearm motion. (C) A Muenster splint that limits elbow extension and forearm rotation
but allows elbow flexion. (A and C are courtesy of S. Blackmore MS, OTR/L, CHT).
functional goals are to gain motion for whatever tasks pressure over the injured area. Flaring of the area and
are required by the patient. use of foam can decrease discomfort and allow for
Strength is maximized to allow for return to ADL, good support. The sling or splint may be used for sup-
hobbies, and work. However, the patient may return port and protection after ROM begins, usually around
to light or modified duty with less than maximal day three following injury.
strength while continuing therapy. In simple operative type II and III fractures, stabi-
Attempting to meet the patient’s personal goals lization in a long-arm cast or splint incorporating the
and expectations for regaining motion and strength elbow, forearm, and wrist to prevent forearm rotation
are the guiding factors when developing therapeutic is recommended (Figures 11A–11C). Stable reduction
goals. If the patient’s expectations are not realistic, and rigid fixation of the radial head are necessary for
then the patient should be educated in the probable early motion. These same splints are used for protec-
outcomes based on the nature of their injuries. tion for up to three weeks with early active motion
beginning as early as day five postoperatively, but
no later than day ten, with stable fracture fixa-
Rehabilitation of Simple Fractures tion.1,8,27,41–43 Limiting forearm rotation and elbow
extension to avoid unnecessary stresses to the healing
Based on the Mayo classification, the term simple fracture is the primary goal of splinting. To accom-
or uncomplicated refers to isolated radial head frac- plish this, Muenster and sugartong splints that allow
tures.8 With this system, the Mason classification de- flexion but limit extension and forearm rotation are
notes the type of fracture involved. Generally, any used preferentially to long-arm splints, which com-
instability present is due to unstable fracture frag- pletely immobilize the elbow. Normally, there are
ments in type II and III and requires surgical inter- no limits for elbow flexion following radial head frac-
vention to stabilize. For simple type I, II, and III, tures; however, radiocapitellar contact increases as el-
early active/active assisted motion (A/AAROM) bow flexion increases, so care should be taken if pain
programs have shown better outcomes versus pro- increases with increasing flexion.
longed immobilization1,8,11,27,42,44,56 (Table 2). Rarely, total immobilization of the elbow is chosen
With simple type I and nonoperative simple type for intervention. One must critically consider the
II radial head fractures, a very short immobilization detrimental effects of prolonged immobilization if
period of up to a week is recommended. In general, this type of intervention is used. Longer immob-
edema and pain dictate the time frame for immobi- ilization causes increased joint stiffness due to adhe-
lizing the elbow. In most cases, sling immobilization sion formation involving the joint capsule and
with a compression bandage is appropriate; however, surrounding soft tissue. An immobilization period
a more rigid support, such as a half cast or splint, may of less than three to four weeks with early active
be necessary (Figure 11B). Care is taken with fabricat- motion has been reported in the literature as having
ing the protective splint to avoid rubbing or increased better outcomes.8,11,42,44,45
126 JOURNAL OF HAND THERAPY
Edema and Pain Control remodeling.44,48 We have found that compressive ap-
plications such as silicone gel sheets and elastomer
Regardless of the intervention chosen to initially molds are excellent ways to minimize hypertrophic
treat the fracture, edema and pain must be addressed scar formation. Either iontophoresis with iodine or
initially since both can limit gains in motion. In some continuous wave ultrasound has been suggested to
cases, the surgeon may elect to aspirate the elbow to help decrease scar formation and thickening.46,47
relieve both swelling and pain.1,27,43 Aspiration of the Early scar care limits the amount of scar tissue and
joint allows surgical assessment for rotational block adhesions that can hinder return of motion.
and also improves early ROM significantly. It is our
experience that this improvement (while beneficial
Early Active/Active Assisted Motion
for patient participation in initial therapy) is only
transient. Early edema control includes rest, ice, com- Early active/active assisted motion for simple
pression, and elevation. Elevation incorporates the radial head fractures has been shown to lead to
use of gravity to decrease edema at the distal extrem- improved outcomes.8,11,27,41,42–44,56 Early A/AAROM
ity, which helps minimize the progression to intersti- helps to prevent stiffness, brawny edema, and adhe-
tial fibrosis associated with chronic edema. This sion formation of the capsule and annular ligament
effect is enhanced with the addition of gentle muscle as well as promote healing and increase tensile
contractions of the upper arm, forearm, and intrinsic strength of the involved bony and soft tissue struc-
muscles of the hand to mobilize the lymphatic and tures.1 In simple type I and II radial head fractures,
venous systems. Ice and compression (in the form A/AAROM may be initiated as soon as edema and
of bandage wrapping or elastic sleeves) can also be pain will allow. For postoperative simple type II and
used between exercise sessions to minimize increases III fractures, A/AAROM usually begins as early as
in edema. Elevation coupled with retrograde mas- day five and less than day ten. Splint use may be con-
sage is another effective method of reducing edema. tinued for protection from heavy activity for up to
Pain control includes a variety of techniques and three weeks following surgery. Full-time elbow immo-
modalities. Initially, medication from the surgeon is bilization of three to four weeks may cause increased
helpful for reducing edema and pain. Cold applica- adhesion formation and stiffness, which lead to in-
tion is an easy and readily available method of creased difficulty with regaining motion.8,11,42,45
decreasing and limiting return of edema as well as Uninvolved joints in the upper extremity, such as
reducing pain symptoms. Electrical stimulation, us- the scapulothoracic joint, shoulder, and wrist, are
ing a variety of waveforms, has been shown to addressed to ensure that motion has not been lost due
decrease pain.46 High-volt pulsed stimulation and to concomitant injury or lack of use. Exercises for
modulated alternating current electrical stimulation these joints should be initiated at the beginning of
aid in pain reduction but have been noted as having therapy, and the motion is monitored regularly. Pain
limited effects in reducing or inhibiting edema.46 at the wrist, especially at the radial ulnar joint/
Ultrasound has demonstrated potential to aid in ulnocarpal area, should be evaluated for an undiag-
edema and pain control; however, its use is limited nosed Essex-Lopresti lesion. Symptoms of this in-
to smaller surface areas, which makes it a poor choice clude wrist pain with loss of motion (primarily
for larger area application.47 Once edema and pain following radial head resection), a prominent dorsal
have been reduced, an early active motion program distal ulna, or severely limited DRUJ rotation. If these
may begin with fewer delays. findings are present but not previously documented,
further evaluation by the surgeon is warranted.
Wound Care and Scar Management Elbow flexion and extension begin in a nonpainful
arc with the forearm in neutral rotation to decrease
In simple type II and III fractures, following surgi- radial head compression. However, positioning the
cal intervention, wound care and scar management forearm in pronation with elbow extension decreases
are important parts of the rehabilitation process. the compressive force at the radial head by decreas-
Rarely does wound care involve more than patient ing the valgus moment associated with end-range
education for maintaining a clean and dry incision extension.49 Positioning the patient supine with the
site to prevent infection and promote healing. Once shoulder at 90° of flexion is a practical way to use
the sutures have been removed, scar management gravity to assist elbow flexion and to increase active
begins. Initially, steri-strips may be applied to main- contraction of the triceps for extension, as well as pro-
tain wound closure and prevent dehiscence. At this vide stabilization for the scapula. The patient seated
time, it is still important to monitor the area for with the elbow and humerus supported on a table
infection. Scar massage may begin at three to four and wedge uses gravity-assisted elbow extension
weeks following surgery to desensitize, add com- and increases active contraction of the biceps for flex-
pressive forces to decrease scar hypertrophy, and ion. The patient should understand the necessity to
add tensile stresses to aid with scar tissue stabilize the scapula with elbow extension to
April–June 2006 127
eliminate protraction compensation. Generally, humerus supported on the plinth or wedge, is an ex-
greater effort is required to regain elbow extension cellent position. The forearm is positioned in either
and forearm rotation. Elbow flexion usually returns neutral or pronation to decrease the valgus forces
more readily. with elbow extension.
Active/active assisted pronation and supination Pronation and supination PROM is performed with
may be initiated. Information from the surgeon will the elbow at 90° with the humerus stabilized. This can
determine if there is a specific limited safe arc of be accomplished with the elbow at the side and using
motion or if motion may be increased as tolerated. a plinth to prevent shoulder abduction and adduction
Initially, the elbow should be positioned in 90° of or with the humerus fixed on the plinth in supine or
flexion. Stabilizing the humerus on a plinth, between sitting (Figures 12A–12B). Rotational force should be
the body and the plinth, or in a doorway for a home directed through the distal radius and ulna, and not
program, decreases compensatory shoulder abduc- the hand, to avoid stressing the ligaments in the wrist.
tion and adduction with pronation and supination. Forceful pronation is avoided initially due to the in-
With the patient completing an early motion pro- creased contact between the healing radial head and
tocol, a home exercise program is initiated in a safe capitellum with increasing pronation.
arc of motion every hour or as edema and pain Motion deficits should be differentiated among
permit. The home program should be modified as capsular joint stiffness or a ‘‘two joint muscle’’ length
necessary to safely regain maximal motion of the restriction, such as the biceps, triceps, or forearm
elbow and forearm. muscles. For instance, if passive elbow extension is
limited, the biceps is evaluated in both lengthened
Passive Range of Motion (shoulder extension and forearm pronation) and
slacked (shoulder flexion and forearm supination)
At four to six weeks from injury or surgery for positions while passively extending the elbow. If it is
simple type I, II, and III, if there is appropriate determined that muscular tightness or guarding is
fracture stability, passive range of motion (PROM) limiting motion, then specific muscle stretching and
may begin. Valgus stress with extension should be muscle energy techniques are incorporated. If, how-
minimized to limit the compressive forces through ever, the motion limitation is unchanged, then the
the radiocapitellar joint (RCJ). The goal of PROM is to limitation is due to joint tightness. The wrist flexor and
maximize motion at the joint without contributing to extensor muscles may also require testing. If the
increased fracture instability. Gentle, sustained restrictions are due to the joint capsule and surround-
stretching should be used with prolonged holds at ing ligaments, the use of hot packs or continuous wave
end ranges of flexion and extension. This follows the ultrasound to the capsule with a sustained stretch can
guide that a low-load, prolonged stress will cause be helpful with increasing motion.47 Further interven-
greater plastic changes in tissues than a high-load, tions such as joint mobilization and splinting may be
short-duration stress.50,51 Overzealous stretching incorporated as adjuncts for increasing joint motion.
may lead to increased edema, guarding, and spasm,
which will limit progression of motion. Elbow flexion Joint Mobilization
and extension PROM begins with the humerus and
scapula in a stable position to avoid compensatory At three to four weeks from injury or surgery for
movements. The patient positioned supine, with the simple type I, II, and III, if the elbow ROM is limited by
FIGURE 12. (A) Passive range of motion (PROM) for supination by a therapist with the humerus fixed on a foam wedge
and the elbow in 90° flexion. (B) An example of self-PROM into supination with the humerus fixed between the patient’s
body and a plinth. Note that the force for rotation is directed through the distal radius and not at the hand in both examples.
128 JOURNAL OF HAND THERAPY
RCJ, humero-ulnar joint (HUJ), PRUJ, or DRUJ tight- RCJ. With full radial head excision, mobilization at
ness, then joint mobilization may begin. It is important the PRUJ is contraindicated. Whereas with partial
to understand that both good fracture and joint stabil- excision of the radial head, mobilization at the PRUJ
ity must be present in order to begin mobilization. is contraindicated only if there is instability of the
Accessory joint motion of the involved and uninvolved lateral pillar.
elbows (assuming that the uninvolved joint is normal)
should be compared to assess for any limitation that is Splinting for Motion
hindering motion. Grade I and II mobilizations for the
RCJ, PRUJ, and DRUJ can be used to decrease pain and Splinting is another method used to increase ROM.
edema. Grade III and IV mobilizations for the RCJ, Splinting to improve ROM is based on the total end-
PRUJ, and DRUJ are used to increase capsule mobility range time concept as described by Flowers and
and elbow motion. For the HUJ, Grade I and II joint LaStayo.51 A low-load, prolonged stress has been
distraction can decrease pain and edema and Grade III shown to increase ROM more effectively than high-
and IV distractions can increase capsular mobility and load, short-duration stresses due to plastic changes
elbow ROM. within the tissue.50,51
Limited pronation and supination may be due to At four to six weeks after injury or surgery for
tightness at either PRUJ or the DRUJ or both. During simple type I, II, and III fractures, splinting may be
supination, the radial head rotates and translates initiated if the patient does not respond to ROM
anteriorly to stretch the anterior capsule and sur- exercises. Normally, elbow flexion does not require
rounding soft tissue at the PRUJ as the distal radius more intervention than ROM exercises. Therefore,
rotates posteriorly around the ulnar head at the most of the splinting for motion focuses on elbow
DRUJ. In pronation, the radius acts in the opposite extension and forearm rotation. Serial static, night-
manner, with the head rotating and translating time elbow extension splinting is an excellent method
posteriorly to stretch the posterior capsule and to increase motion using a low-load prolonged stress.
surrounding soft tissue as the radius rotates volarly A volar long-arm serial static splint, such as a belly
around the ulna. Therefore, if forearm supination gutter, may be used at bedtime for elbow flexion
rotation is limited by the PRUJ, anterior mobilization contractures of 30° or less (Figures 13A–13C). Care
of the radial head at the PRUJ is appropriate, whereas should be taken with serial static splinting to position
if there is limitation at the DRUJ, posterior mobiliza- the joint in a tolerable end-range position, as stretch-
tion of the radius on the ulna is appropriate. For ing beyond tolerance can increase pain and decrease
pronation, these would be reversed. splint compliance, which could potentially contribute
With simple type II and III fractures treated with to increased edema and scarring. Static progressive
surgery, the fracture stability should be verified splints such as the turnbuckle and JAS elbow and
prior to initiating mobilization to the PRUJ and pronation/supination splints (Joint Active Systems,
FIGURE 13. (A) A serial static volar long-arm belly gutter splint used for contractures of 30° or less. (B) A static-progress-
ive turnbuckle extension splint used for contractures of greater than 30°. (C) A dynamic supination/pronation splint.
(Photos courtesy of S. Blackmore, MS, OTR/L, CHT).
April–June 2006 129
Inc., Effingham, IL) are used for flexion contractures Gradual progressive resisted exercises for the el-
greater than 30° and forearm rotation. Custom ther- bow, forearm, and wrist are initiated at four to six
moplastic dynamic splinting and the Dynasplint el- weeks following injury or surgery of simple type I, II,
bow and pronation/supination splint (Dynasplint and III fractures. For elbow flexion and extension,
Systems, Inc., Severna Park, MD) may also be used strengthening should begin in pain-free arcs of
for flexion contractures greater than 30° and forearm motion with light resistance with hand or cuff
rotation. Static progressive and dynamic splinting weights or resistive bands with progression as toler-
can be used intermittently during the day. (See ated. Pronation and supination strengthening begins
Davila and Johnston-Jones article in this issue for with the elbow in 90° of flexion to minimize force at
more information on splinting used to regain motion.) the radial head and in a pain-free arc. The resistance
When fitting the patient with a splint to improve and ROM may be increased as tolerated. It is neces-
motion, it is important to avoid unnecessary valgus sary to have good wrist stability to maintain neutral
and varus stresses at the elbow. Valgus stress, espe- wrist posture with pronation/supination strengthen-
cially with extension, can cause increased compres- ing. A splint to support the wrist temporarily with
sion of the radial head. To avoid these stresses, these exercises may be used so neutral wrist position
attention is directed to proper splint fitting and can be maintained for strengthening. At this time,
patient education on proper splint use. strengthening for the rotator cuff can be added using
weights or resisted bands if needed. Internal rotation
Strengthening and Conditioning may be held, initially, if the valgus force causes dis-
comfort at the radial head.
It is important to maintain the musculature of the Once good ROM and strength of the upper ex-
upper extremity as the fracture is healing. The ability of tremity are achieved, formal work and avocational
the scapular musculature to form a stable base for the activity conditioning may begin as necessary. To
upper extremity is of utmost importance in regaining prepare patients who have been out of work for an
ROM and strength in the elbow, forearm, and wrist. For extended period for their return, specific condition-
that reason, proximal strengthening of the shoulder ing is necessary. The program should incorporate
girdle complex should be initiated if needed. Active not only the upper extremity but also total body con-
scapular exercises involving elevation/depression, ditioning to enable a safe transition to full work
protraction/retraction, and combined motions are duties. For manual laborers, activities that mimic
started with initiation of therapy. Prone exercises for the patient’s daily activities such as box lifting and
scapular strengthening may be used without adding carrying, pushing and pulling carts, and use of tools
stress to the healing radial head. However, prone such as screwdrivers and wrenches are excellent ad-
shoulder external rotation can stress the LCL and ditions to the conditioning program. Equipment with
should be avoided initially if there is pain. Exercises isotonic and isometric instrumented dynamometers
for the deltoid may be added in either seated or is available for exercise including those by
standing position. Resistance may be added via cuff Baltimore Therapeutic Equipment (Hanover, MD)
weights proximal to the elbow as the patient pro- and Biodex (Shirley, NY), which can be used to
gresses. It may be necessary to wear the elbow splint to strengthen as well as simulate work activities in var-
protect the fracture with these exercises. ious positions. In some cases, a modified or short-
The early addition of isometric exercises and fine ened workday coupled with work conditioning
motor activities may also aid with decreasing edema enables the patient to make a smooth transition
distally. The submaximal isometrics are used to back to the workplace.
maintain muscle quality and tone and avoid exces- Patients may be returning to avocational activities
sive atrophy. Thus, the submaximal wrist isometric such as hobbies or sports that require specific condi-
exercises may be initiated early. Submaximal elbow tioning. For instance, baseball and softball players
and forearm isometrics, however, should be initiated use throwing programs that are position specific to
later at three to four weeks following injury or return to their sports. It is important to know the level
surgery of simple type I, II, and III fractures when of function that is necessary for each patient to safely
there is sufficient fracture stability to tolerate forces and confidently return to his or her pre-injury level of
across the radial head. There is evidence that the activity and design a conditioning program appro-
flexor–pronator mass adds dynamic stabilization priate to reach that level.
against valgus stress, namely the flexor carpi ulnaris
and flexor digitorum superficialis.52 Strengthening Complications
and fine motor activities for the intrinsic hand mus-
cles and digits are initiated if needed. Fine motor Elbow and wrist pain, stiffness, and radiocapitellar
and dexterity activities not only aid with digital arthritis can occur. Symptomatic fracture nonunion
motion but also use combined motion of the upper can limit motion and function. Contractures limiting
extremity, which promotes motion at all joints. extension may develop due to adhesions of the
130 JOURNAL OF HAND THERAPY
anterior capsule. A residual flexion contracture of 10– Postoperative care for complex type II and III
15° is not infrequent in the more severe injuries. fractures depends on the surgeon’s intervention. As
Adhesions involving the radial neck and annular with simple type II and III fractures, stable reduction
ligament may limit rotation of the forearm. Muscle and rigid fixation of the radial head are necessary for
guarding or spasm, most notably by the biceps early motion. However, intervention regarding asso-
brachii, can limit elbow motion.53 Development of ciated injuries will modify the rehabilitation pro-
HO or myositis ossificans can also prevent elbow mo- gram. For example, when a coronoid fracture has
tion. Wrist pain and loss of motion may be indicative undergone surgical fixation, elbow extension is lim-
of an Essex-Lopresti lesion, which may not have been ited to prevent stress to the repair and redislocation.
initially diagnosed. LCL injuries are not always surgically reconstructed,
depending on elbow stability following the radial
Rehabilitation of Complex Fractures head repair. With nonsurgical and surgically treated
LCL injuries, varus stress with positioning and mo-
Complex or complicated radial head fractures also tion is avoided. The forearm is positioned in prona-
involve concomitant elbow fractures or ligament tion within a splint to increase stability (see later in
injury.8 These fractures are designated type I–III corre- this paper). MCL reconstruction is not frequently per-
sponding to the Mason classification. Complex frac- formed since repair of the radial head and LCL gen-
tures differ from simple ones because of the addition erally provides adequate stability for early motion.
of instability of the elbow due to factors beyond the ra- With both LCL and MCL injuries, a hinged elbow
dial head fracture fragment alone. Rehabilitation of splint may be necessary for increased stability.
these injuries depends on the level of involvement of Studies have shown that in cases with a compro-
concomitant factors and the intervention chosen by mised or absent MCL, the radiocapitellar complex
the surgeon (Table 3). acts to assist against cubitus valgus and thus becomes
The approach used by the surgeon and therapist an important stabilizer to valgus stress.1,8,17,54 In this
for complex type I and type II fractures involving lig- new role (as the sole remaining valgus stabilizer), the
amentous or other osseous structures with resultant radial column sees increased compressive joint
instability will be different from that used for simple forces, which may stress the radial head repair or
type I and II fractures. Complex type I fractures are the nondisplaced fracture. However, if there is an
rare and require focusing on the concomitant injuries MCL injury, splinting with the forearm in supination
since the radial head fracture is stable. Treatment in- aids in stability with motion and valgus stress is
volves splinting coupled with an early ROM pro- avoided. A hinged elbow splint will increase stability
gram. Splinting stabilizes against varus/valgus and decrease valgus stresses. An associated Essex-
stresses and limits elbow extension within a stable Lopresti lesion may require splinting in supination
range (see later in this article). Splint use may con- to reduce the dorsal ulnar head instability. Surgery
tinue for protection for three to four weeks following may be required to stabilize the DRUJ. Olecranon
injury. Complex type II can be treated nonsurgically fractures require limitation of extension and full flex-
or surgically. Nonsurgical type II treatment denotes ion. Because the triceps inserts onto the olecranon,
a stable radial head fracture fragment without dis- early active extension and full passive flexion are
placement or rotational block. Initial treatment is contraindicated. With more global instability, hinged
the same as that for complex type I. Surgical type II external fixation may be necessary to provide stabil-
requires addressing both the fracture intervention ity and allow for a limited arc of early motion.
and intervention for concomitant injury. The elbow
and forearm are immobilized in a long-arm splint Splinting
or locked hinged splint for a period of less than ten
days followed by an early motion program. A hinged Splinting for elbow stabilization with an extension
splint is then used to allow elbow motion within safe block is common with complex fracture rehabilita-
limits and prevent varus/valgus stresses (see below). tion. Splinting can be either custom thermoplastic or
The splint is worn for up to six weeks for protection. prefabricated in nature. With instability due to liga-
Muenster and sugartong splints are inappropriate mentous or concomitant fractures, a hinged elbow
due to their inability to provide the accurate limita- splint can be used to provide initial immobilization
tion of extension necessary for the unstable elbow. and later unlocked to allow for protected motion.8,42
For complex type III and Johnston type IV frac- The splint is worn for three to six weeks following
tures, both the surgical repair of the radial head and surgery and will require modification as edema
the repair of the associated injuries dictate rehabili- decreases. The patient is provided with information
tation. Initial management is the same as that for regarding proper care, use, and skin monitoring.
complex type II fractures. However, a hinged external The typical forearm position when managing el-
fixation device may be necessary to maintain elbow bow instability is pronation. In our opinion, forearm
reduction stability. rotation needs to be modified according to elbow
April–June 2006 131
stability. An unstable fracture fragment at the more For complex type I and nonsurgical type II, A/
common anterolateral aspect of the radial head AAROM begins after less than ten days of immobi-
causes posteromedial instability. Positioning the fore- lization as immobilization periods of three weeks or
arm in pronation allows the larger, stable portion of more have demonstrated less favorable results.8,42,44
the radial head to contact the capitellum, which aids Care is taken to avoid stresses to associated injuries.
with stabilizing the joint. However, an unstable frac- For instance, with MCL and LCL injuries, valgus
ture fragment at the PL aspect of the radial head leads and varus stresses should be minimized. Motion is
to anteromedial instability, which is more effectively limited to the stable arc indicated by the surgeon.
stabilized with the forearm in supination. If the MCL In complex surgical type II and III fractures with
is injured, the forearm is positioned in supination, either ligamentous or concurrent bony injuries, mo-
which tightens the lateral ligaments and flexor/pro- tion begins within ten days of surgery in protected
nator origin while providing lateral column support forearm rotation (described previously) and limited
against valgus stress. For LCL injuries, the forearm arc of motion. Knowledge of the injured ligaments and
is pronated, which tightens the medial ligaments bony structures and an understanding of the elbow
and extensor/supinator origin.11,48 For injuries to and forearm kinematics are essential for proper treat-
both the LCL and MCL, the forearm is positioned in ment. For instance, if the LCL was reflected or
neutral or, in some cases, an examination under anes- reconstructed during the procedure, then varus
thesia by the surgeon is required to determine the stresses are minimized and a pronated forearm posi-
safe arc or safe position. In a study by Pomianowski tion is maintained with elbow motion to increase
et al., varus and valgus laxity was examined under stability. The range through which motion is safe is
a variety of surgical and nonsurgical conditions and indicated by the surgeon. The use of the hinged elbow
flexion angles.55 They found that laxity was signifi- splint increases stability with early motion while
cantly affected by forearm rotation position. It was protecting against valgus and varus moments that
determined that elbow laxity for both varus and val- would normally stress the MCL and radial head and
gus loads was greatest in pronation and 20° of elbow LCL. The splint is locked in 90° flexion between
flexion. For complex fractures with joint instability, exercise sessions, with forearm rotation dictated by
the position of the forearm for both immobilization the associated injury as described above. If a hinged
and ROM must be discussed with the surgeon to external fixation device is used, early motion is started
plan for greatest stability and least stress to the in- in a similar manner as with a hinged splint.
jured structures. Active/active assisted motion should begin with
the humerus stabilized with proper forearm rotation
maintained. The specific degree for the stable arc of
Pain and Edema Control and Wound Care motion, especially into extension, is obtained from
the surgeon. The patient begins with tolerable motion
As with rehabilitation with simple fractures,
within the stable arc in flexion and extension. At
edema, pain, wound care, and scar management
home, this motion is performed by the patient in the
must be addressed early. The same methods as those
splint initially. The blocks set by the therapist or
described previously for simple fractures apply to
surgeon on the hinged splint limit the patient’s
complex fracture care. If a hinged external fixation
motion at home. In therapy, the splint may be
device is used, additional patient education regard-
removed and A/AAROM in a safe arc of motion is
ing the device is necessary. The pin sites are avenues
performed and carefully monitored. Elbow motion
from the outside environment directly to the bone so
performed with the patient in supine with the shoul-
prevention of infection is of utmost importance. Once
der in flexion provides increased stability with elbow
these factors are addressed, an early motion protocol
flexion and extension. Gradually, the arc of motion is
may begin with fewer hindrances.
increased at a rate of 5–10° of extension and 10° of
flexion per week as tolerated without compromising
Early Active/Active Assisted Motion healing structures or stability.
Pronation and supination active motion begins in
Early motion following complex fractures is simi- 90° of elbow flexion.11,36 It is important to guard
lar to that following simple fractures. The concept of against unnecessary varus or valgus stresses.
using motion early in the healing process to prevent Stabilizing the humerus, as with simple fractures,
stiffness, adhesion formation of the radial head and aids with decreasing compensatory motions that in-
neck with the annular ligament and brawny edema crease valgus and varus moments at the elbow.
formation, as well as promote healing, increase mo- Again, forearm rotation may be limited initially due
tion, and increase tensile strength of the involved to specific positioning for instability. For instance, if
tissue is the same.1,8,11,27,42,43,56 Motion of nonaffected the forearm is held in pronation to increase stability,
joints such as the scapulothoracic joint, shoulder, then forearm rotation should be limited to neutral
wrist, and hand should begin immediately. for four to six weeks, then gradually progressed
132 JOURNAL OF HAND THERAPY
into supination.36 The opposite would be used for a there is good stability of the joint and all fractures are
forearm being held in supination. healed. Splinting to regain motion has been described
earlier. Due to a history of joint instability, careful
Passive Range of Motion assessment must be made of joint stresses applied by
any splint and patient pain associated with splint use.
Passive range of motion begins at six to eight Avoiding unnecessary stresses on healing structures
weeks following surgery depending on fracture heal- is important. Low-load prolonged stress not only
ing and joint stability. Information obtained from the lengthens tight capsular structures, but also places a
surgeon regarding healing status will determine if stress on the remodeling ligaments. Understanding
PROM is appropriate. PROM guidelines were out- the effects of splinting on all tissues involved is
lined previously with simple fractures. It is also im- important to maximize elbow motion while main-
portant to be vigilant on avoiding stress to injured taining stability.
ligaments or stretching into unstable ranges.
Maintaining proper forearm rotation as described
previously is important for elbow stability. Strengthening and Conditioning
As with simple fractures, muscle tightness or Maintaining the musculature of uninvolved joints
guarding may limit motion. Testing the triceps and is important as described for simple fractures.
biceps in both lengthened and slacked positions will Exercises for shoulder musculature including those
determine if the motion deficit is due to the muscle or for scapular stabilization may be started in the first
from capsular or joint limitations. Forearm muscula- week within tolerance. External rotation of the
ture should be assessed for shortening. shoulder with the patient prone-lying is avoided
initially due to increased stress on the LCL. The
Joint Mobilization
splint should be used while performing these exer-
Joint mobilizations with healing elbow instability cises to protect the elbow from harmful stresses. If a
should be used by only therapists who are highly hinged external fixation device is being used, active
competent and well experienced with manual tech- assisted motion may be necessary early due to the
niques. Joint mobilization is never used on the unsta- added weight from the device. Fine motor/dexterity
ble elbow. Once appropriate fracture and soft tissue exercises of the digits and intrinsic hand muscle
healing has occurred and the joint is considered to be strengthening may begin as tolerated. Activities may
stable, joint mobilization is used judiciously to gain have to be modified due to protective splinting or
motion in complex type I and nonsurgical type II external fixation. Wrist submaximal isometrics may
fractures. At six to eight weeks following surgery or begin early to assist with maintaining muscle tone
injury, radiocapitellar mobilizations may be appro- and decreasing edema unless there is a concomitant
priate after sufficient healing has occurred. Grade I wrist, IOM, or muscular injury. In these cases,
and II mobilizations may be appropriate to decrease isometrics should be held until sufficient healing
pain and edema. However, Grade III and IV mobili- has occurred. Isometric wrist exercises may contrib-
zations are used judiciously and only with a stable ute to soft tissue discomfort at pin sites if a hinged
joint. As with simple fractures, accessory joint motion external fixation device is used. Generally, strength-
should be assessed initially to determine if capsular ening can begin for the above motions at four to
tightness is limiting motion. If a coronoid or olecranon eight weeks following injury or surgery depending
fracture is involved, ulnohumeral joint distraction is on the severity of the injuries. The same is true with
contraindicated until full bony stability has occurred elbow isometric exercises. In stable elbow positions
and no other instability is present. and forearm rotation, submaximal elbow isometric
For complex type II and type III fractures treated by exercises may begin at three to four weeks postsur-
excision or arthroplasty, RCJ mobilizations are con- gery. When there is significant elbow or forearm
traindicated. When the radial head is excised, there is instability, strengthening may be delayed until six to
already an inherent instability present. There is a risk eight weeks. When a hinged external fixation device
of loosening the prosthesis with mobilization that is used, strengthening is generally deferred until
would lead to complications such as pain, decreased removal of the device and healing of bone and
motion, and instability. PRUJ and DRUJ mobiliza- tissues related to the pin sites.
tions are contraindicated with IOM, DRUJ, and PRUJ For complex type II and III injuries, progression of
injuries, radial head excision or arthroplasty, and ROM activities of the elbow and forearm to strength-
radial head instability. ening may begin at six to eight weeks following sur-
gery. This time frame is based on the need for fracture
Splinting for Motion stability and adequate ligamentous stability. The sur-
geon is consulted to determine if it is appropriate to
Splinting is an option to gain motion at four to progress the program to strengthening. When a
eight weeks following surgery or injury provided hinged external fixation device is used, this timeline
April–June 2006 133
may be eight to 12 weeks following surgery after re- 2. Schwartz RP, Young F. Treatment of fractures of the head and
moval of the device. The progression for strengthen- neck of the radius and slipped radial epiphysis in children.
Surg Gynecol Obstet. 1933;22:528–37.
ing described for simple fractures can be applied to 3. Hammond R. Fracture of the head and neck of the radius. Ann
complex fractures. Surg. 1910;53:207–14.
Based on the nature of the involved structures, 4. Watson-Jones R. Discussion of minor injuries of the elbow joint.
Proc R Soc Med. 1930;23:323–7.
modification of the strengthening exercises may be
5. Mason ML. Some observations on fracture of the head of the
necessary. For the wrist, forearm, and elbow, resis- radius with a review of one hundred cases. Br J Surg. 1954;
tive exercises should begin in a stable, pain-free 42:123–32.
range. It is important to stress correct form with 6. Johnston GW. A follow-up of one hundred cases of fracture of
the head of the radius with a review of the literature. Ulster
exercises to prevent stresses to healing ligaments or Med J. 1962;31:51–6.
fractures of the elbow. For instance, in attempting to 7. Hotchkiss RN. Displaced fractures of the radial head: internal
gain more supination, a patient may compensate fixation or excision? J Am Acad Orthop Surg. 1997;5:1–10.
with shoulder adduction and external rotation, 8. Morrey BF. Radial head fracture. In: Morrey BF (ed). The Elbow
and Its Disorders. Philadelphia, PA: WB Saunders, 2000, pp
which causes a valgus stress on the elbow. 341–64.
Shoulder and scapular exercises can be progressed 9. Speed K. Ferrule caps for the head of the radius. Surg Gynecol
as long as the injured structures are protected until Obstet. 1941;73:845–50.
they are stable. 10. Swanson AB, Jaeger SH, La Rochelle D. Comminuted fractures
of the radial head: the role of silicone-implant replacement
At 12–16 weeks postsurgery, the rehabilitation pro- arthroplasty. J Bone Joint Surg Am. 1981;63:1039–49.
gram should be modified to include work condition- 11. Moro JK, Werier J, MacDermid JC, et al. Arthroplasty with a
ing or avocational needs as described previously. A metal radial head for unreconstructible fractures of the radial
total body conditioning program based on the pa- head. J Bone Joint Surg Am. 2001;83:1201–11.
12. Smets S, Govaers K, Jansen N, et al. The floating radial head
tient’s job-specific tasks begins. Modifications may prosthesis for comminuted radial head fractures: a multicen-
be made to accomplish job tasks in the case of motion tric study. Acta Orthop Belg. 2000;66:353–8.
loss as long as safety is preserved. The patient may 13. King GJ, Zarzour ZD, Patterson SD, Johnson JA. An anthropo-
metric study of the radial head: implications in the design of a
work with a supportive brace in cases of prolonged
prosthesis. J Arthroplasty. 2001;16:112–6.
instabilities. Once again, returning to work in a 14. Soyer AD, Nowotarski PJ, Kelso TB, Mighell MA. Optimal
modified duty or partial day situation along with a position for plate fixation of complex fractures of the proximal
continued conditioning program is very beneficial radius: a cadaver study. J Orthop Trauma. 1998;12:291–3.
15. Smith GR, Hotchkiss RN. Radial head and neck fractures: ana-
to the patient. tomic guidelines for proper placement of internal fixation.
J Shoulder Elbow Surg. 1996;5:113–7.
16. Dunning CE, Zarzour ZD, Patterson SD, et al. Ligamentous
CONCLUSIONS AND PRACTICE stabilizers against posterolateral rotatory instability of the
RECOMMENDATIONS elbow. J Bone Joint Surg Am. 2001;83:1823–8.
17. Morrey BF, Tanaka S, An KN. Valgus stability of the elbow: a
definition of primary and secondary constraints. Clin Orthop
Accurate and complete diagnosis and early inter-
Relat Res. 1991;Apr(265):187–95.
vention coupled with early motion protocols provide 18. Amis AA, Miller JH, Dowson D, Wright V. Biomechanical
the best outcomes for radial head fractures and aspects of the elbow: joint forces related to prosthesis design.
associated injuries.1,8,11,27,42,43,56 It is imperative that Eng Med. 1981;10:65–8.
19. O’Driscoll SW, Morrey BF, Korinek S, An KN. Elbow subluxa-
the surgeon and therapist have early and continued tion and dislocation: a spectrum of instability. Clin Orthop.
communication to effectively treat the patient. The 1992;Jul(280):186–97.
surgeon must provide information to the therapist re- 20. Regan W, Morrey B. Fractures of the coronoid process of the
garding the injured structures, specifics about surgi- ulna. J Bone Joint Surg Am. 1989;71:1348–54.
21. Amis AA, Miller JH. The mechanisms of elbow fractures: an
cal intervention, stability of fracture fixation, and investigation using impact tests in vitro. Injury. 1995;26:163–8.
joint stability. The therapist must understand tissue 22. Ward WG, Nunley JA. Concomitant fractures of the capitellum
healing, potential stresses to tissues, and treatment and radial head. J Orthop Trauma. 1988;2:110–6.
techniques to protect the simple and complex in- 23. Davidson PA, Moseley JB Jr, Tullos HS. Radial head fracture:
a potentially complex injury. Clin Orthop. 1993;Dec(297):224–30.
juries. The patient must be educated in possible out- 24. Halls AA, Travill A. Transmission of pressures across the
comes, safe arcs of motions, positioning, and proper elbow joint. Anat Rec. 1964;150:243–8.
splint use. With the patient, doctor, and therapist 25. Sowa DT, Hotchkiss RN, Weiland AJ. Symptomatic proximal
trio working together, maximal functional outcome translation of the radius following radial head resection. Clin
Orthop. 1995;Aug(317):106–13.
can be attained for simple and complex types of 26. Trousdale RT, Amadio PC, Cooney WP, Morrey BF. Radio-
radial head fractures. ulnar dissociation: a review of twenty cases. J Bone Joint
Surg Am. 1992;74:1486–97.
27. Morrey BF. Current concepts in the treatment of fractures of the
REFERENCES radial head. In: Jackson DW (ed). Instructional Course Lec-
tures, Vol. 44. Tauton, MA: Rand McNally, 1995, pp 175–85.
1. King GJW. Fracture of the head of radius. In: Green DP, et al 28. Beingessner DM, Dunning CE, Beingessner CJ, et al. The effect
(ed). Green’s Operative Hand Surgery, Vol. 1. 5th ed. Philadel- of radial head fracture size on radiocapitellar joint stability.
phia, PA: Elsevier Churchill Livingston, 2005, pp 845–87. Clin Biomech. 2003;18:677–81.
134 JOURNAL OF HAND THERAPY
29. Geel CW, Palmer AK, Ruedi T, Leutenegger AF. Internal fixa- 43. Kuntz DG, Baratz ME. Fractures of the elbow. Orthop Clin
tion of proximal radial head fractures. J Orthop Trauma. North Am. 1999;30:37–61.
1990;4:270–4. 44. Broberg MA, Morrey BF. Results of delayed excision of the radial
30. Arner O, Ekengren K, Von Schreeb T. Fractures of the head and head after fracture. J Bone Joint Surg Am. 1986;68A:669–74.
neck of the radius: a clinical and roentgenographic study of 310 45. Cyr LM, Ross RG. How controlled stress affects healing tissues.
cases. Acta Chir Scand. 1957;112:115. J Hand Ther. 1998;11:125–30.
31. Beingessner DM, Dunning CE, Gordon KD, et al. The effect of 46. Robinson AJ, Snyder-Mackler L (eds). Clinical Electrophysiolo-
radial head excision and arthroplasty on elbow kinematics and gy—Electrotherapy and Electrophysiologic Testing. 2nd ed.
stability. J Bone Joint Surg Am. 2004;86:1730–9. Philadelphia, PA: Williams and Wilkins, 1995.
32. Roberts PH. Dislocation of the elbow. Br J Surg. 1969;56:806–15. 47. Michlovitz SL. Thermal Agents in Rehabilitation. 2nd ed. Phil-
33. Lansinger O, Karlsson J, Korner L, Mare K. Dislocation of the adelphia, PA: FA Davis Company, 1990.
elbow joint. Arch Orthop Trauma Surg. 1984;102:183–6. 48. Smith KL, Dean SJ. Tissue repair of the epidermis and dermis.
34. Middleton RW, Miles NM. A report of a case of non-union J Hand Ther. 1998;11:95–104.
following fracture of the neck of the radius. Injury. 1976;8:31–4. 49. Norkin CC, Levangie PK. The elbow complex. In: Norkin CC,
35. Garland DE, Hanscom DA, Keenan MA, et al. Resection of het- Levangie PK (eds). Joint Structure and Function—A Compre-
erotopic ossification in the adult with head trauma. J Bone Joint hensive Analysis. 2nd ed. Philadelphia, PA: FA Davis Com-
Surg Am. 1985;67:1261–9. pany, 1992, pp 240–61.
36. Davila SA. Therapist’s management of fractures and disloca- 50. Hardy M, Woodal W. Therapeutic effects of heat, cold, and
tions of the elbow. In: Mackin EL, et al (ed). Rehabilitation of stretch on connective tissue. J Hand Ther. 1998;11:148–56.
the Hand and Upper Extremity, Vol. 2. 5th ed. Philadelphia, 51. Flowers K, LaStaya P. Effect of total end range time on
PA: Mosby, 2002, pp 1230–43. improving passive range of motion. J Hand Ther. 1994;7:150–7.
37. Hislop HJ, Montgomery J. Daniel’s and Worthingham’s Muscle 52. Park MC, Ahmad CS. Dynamic contributions of the flexor-
Testing—Techniques of Manual Examination. 6th ed. Philadel- pronator mass to elbow valgus stability. J Bone Joint Surg
phia, PA: WB Saunders Company, 1995, pp 108–123. Am. 2004;86A:2268–74.
38. Magee DJ. Orthopedic Physical Assessment. 4th ed. Philadel- 53. Page C, Backus SI, Lenhoff MW. Electromyographic activity in
phia, PA: Saunders, 2002. stiff and normal elbows during elbow flexion and extension.
39. Morrey BF, Askew LJ, Chao EY. A biomechanical study of nor- J Hand Ther. 2003;16:5–11.
mal functional elbow motion. J Bone Joint Surg Am. 1981;63A: 54. Werner FW. Principles of musculoskeletal biomechanics—
872–7. forearm and elbow joint. In: Peimer CA (ed). Surgery of the
40. Vasen AP, Lacey SH, Keith MW, Shaffer JW. Functional range Hand and Upper Extremity, Vol. 1. New York, NY: McGraw-
of motion of the elbow. J Hand Surg [Am]. 1995;20:288–92. Hill, 1996, pp 19–29.
41. Morrey BF. Radial head fractures. In: Morrey BF (ed). The 55. Pomianowski S, O’Driscoll SW, Neale PG, Park MJ, Morrey BF,
Elbow. 2nd ed. Philadelphia, PA: Lippincott, Williams and An KN. The effect of forearm rotation on laxity and stability of
Wilkins, 2002, pp 83–102. the elbow. Clin Biomech. 2001;16:401–7.
42. Broberg MA, Morrey BF. Results of treatment of fracture- 56. Teasdale R, Savoie FH, Hughes JL. Comminuted fractures of
dislocations of the elbow. Clin Orthop. 1987;Mar(216):109–19. the proximal radius and ulna. Clin Orthop. 1993;292:37–47.
April–June 2006 135
JHT Read for Credit
Quiz: Article #022
Record your answers on the Return Answer Form c. nondisplaced radial head fracture 1 TFCC
found on the tear-out coupon at the back of this tear
issue. There is only one best answer for each d. comminuted radial head fracture 1 MCL
question. injury
#4. The "terrible triad" is a combination of these
#1. Radial head resection following fracture may be three:
complicated by: a. radial head fracture, olecranon fracture, dislo-
a. ulnar shortening and negative ulnar variance cation of the elbow
b. radial lengthening and positive radial b. radial head fracture, coronoid fracture, olecra-
variance non fracture
c. radial shortening and positive ulnar variance c. radial head fracture, coronoid fracture, dislo-
d. ulnar lengthening and negative ulnar variance cation of the elbow
#2. The shape of the radial articular dish is: d. radial head fracture, TFCC tear, IOM tear
a. elliptical #5. The key to good management of most nondis-
b. spherical placed radial head fractures is:
c. irregular a. aggressive PROM
d. flat b. early ROM
#3. The following combination leads to instant val- c. the strict avoidance of any PROM
gus instability with long-term sequelae: d. strengthening
a. comminuted radial head fracture 1 LCL
injury When submitting to the HTCC for recertification,
b. comminuted radial head fracture 1 anterior please batch your JHT RFC certificates in groups
joint capsule injury of three or more to get full credit.
136 JOURNAL OF HAND THERAPY
You might also like
- Operative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesFrom EverandOperative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesAlexander Y. ShinNo ratings yet
- Complex Elbow InstabilityDocument9 pagesComplex Elbow InstabilityAristoteles Plato SocratesNo ratings yet
- Elbow Fractures: Distal Humerus: The American Society For Surgery of The Hand.)Document15 pagesElbow Fractures: Distal Humerus: The American Society For Surgery of The Hand.)Radu UrcanNo ratings yet
- Tratamiento Quirurgico de Triada Terrible de CodoDocument9 pagesTratamiento Quirurgico de Triada Terrible de Codotraumatologia ortopediaNo ratings yet
- Fracturas Seno FrontalDocument16 pagesFracturas Seno FrontalMarisol Gallego DuqueNo ratings yet
- 1950 Don H. O'Donoghue Surgical Treatment of Fresh Injuries To The Major Ligaments of The KneeDocument4 pages1950 Don H. O'Donoghue Surgical Treatment of Fresh Injuries To The Major Ligaments of The KneeJohannes CordeNo ratings yet
- 2015 Article 75Document9 pages2015 Article 75Finna Tryasti Fidianti1BNo ratings yet
- Misra 2019Document3 pagesMisra 2019Jawhar DhiafNo ratings yet
- Adult Traumatic Brachial PlexusDocument12 pagesAdult Traumatic Brachial PlexusMarjeane Cristina Jaques Hockmuller mhockmullerNo ratings yet
- Current Concepts in Midface Fracture ManagementDocument9 pagesCurrent Concepts in Midface Fracture ManagementMarkNo ratings yet
- Trauma C1 C2Document8 pagesTrauma C1 C2Karen OrtizNo ratings yet
- Current Concepts Tibial Plateau FXDocument14 pagesCurrent Concepts Tibial Plateau FXOrtho 20172100% (1)
- Current Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiDocument8 pagesCurrent Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiJoão Artur BonadimanNo ratings yet
- Surat KuasaDocument9 pagesSurat KuasarifkizidnyNo ratings yet
- Fracturas PatologicasDocument20 pagesFracturas PatologicasSamantha AriasNo ratings yet
- 17 - Distal Radius FracturesDocument78 pages17 - Distal Radius FracturesFlorin PanduruNo ratings yet
- Stav SoucasnyDocument14 pagesStav SoucasnyTommysNo ratings yet
- Skeletal Trauma 6th Edition-9-MinDocument81 pagesSkeletal Trauma 6th Edition-9-Minjuan ricardo carvajal alvaradoNo ratings yet
- Fractura e FalangsDocument16 pagesFractura e FalangsJulio Cesar Guillen MoralesNo ratings yet
- Fractures of The Radial Head (2013)Document9 pagesFractures of The Radial Head (2013)Say MamenNo ratings yet
- Traumatic and Trauma-Related Amputations: Current Concepts ReviewDocument17 pagesTraumatic and Trauma-Related Amputations: Current Concepts ReviewJUANNo ratings yet
- Exogenous Spinal Trauma-Surgical Therapy and AftercareDocument8 pagesExogenous Spinal Trauma-Surgical Therapy and Aftercaretaner_soysurenNo ratings yet
- Proximal Humeral FracturesDocument12 pagesProximal Humeral FracturesAlanwalk CompanyNo ratings yet
- 12 - Rehabilitation After Fractures of - 2018 - Clinical Orthopaedic Rehabilitat PDFDocument7 pages12 - Rehabilitation After Fractures of - 2018 - Clinical Orthopaedic Rehabilitat PDFTolo CantallopsNo ratings yet
- Fratura Tipo II Odontoide Com PseudoatroseDocument7 pagesFratura Tipo II Odontoide Com PseudoatroseJesus DecepcionadoNo ratings yet
- Distal Radius Fractures in The Elderly: Review ArticleDocument17 pagesDistal Radius Fractures in The Elderly: Review ArticleBli PutuNo ratings yet
- Principle of FracturesDocument33 pagesPrinciple of FracturesMARISOL GALLEGO DUQUENo ratings yet
- Acute Midshaft Clavicular Fracture PDFDocument10 pagesAcute Midshaft Clavicular Fracture PDFDiana Marcela Benítez HernándezNo ratings yet
- Diagnosis and Treatment of Multiligament Knee Injury: State of The ArtDocument19 pagesDiagnosis and Treatment of Multiligament Knee Injury: State of The ArtsabariaNo ratings yet
- FxClavícula PDFDocument7 pagesFxClavícula PDFPenélope CrespoNo ratings yet
- Defroda 2016Document6 pagesDefroda 2016Guido Alfonso Fierro PortoNo ratings yet
- Art 1Document10 pagesArt 1Danilo LlumitasigNo ratings yet
- Closed Manipulation and Casting of Distal Radius FracturesDocument10 pagesClosed Manipulation and Casting of Distal Radius FracturesDody KurniawanNo ratings yet
- Approaching Unusual Pediatric Distal Humeral FracturesDocument11 pagesApproaching Unusual Pediatric Distal Humeral FracturesDiego Rivas-VazquezNo ratings yet
- Tan2012 PDFDocument10 pagesTan2012 PDFdebyanditaNo ratings yet
- Treatment of Humeral Shaft Fractures: A Critical Analysis ReviewDocument9 pagesTreatment of Humeral Shaft Fractures: A Critical Analysis ReviewRafaelAntonioNarvaezAguirreNo ratings yet
- One Night With The BillionerDocument10 pagesOne Night With The BillionerEmma KuderaNo ratings yet
- Manejo de Fracturas Mediales de Cadera 2015 Femoral Neck Fractures - Current ManagementDocument9 pagesManejo de Fracturas Mediales de Cadera 2015 Femoral Neck Fractures - Current ManagementSergio Tomas Cortés MoralesNo ratings yet
- Rehabilitation After Plate Fixation of Upper and Lower Extremity FracturesDocument6 pagesRehabilitation After Plate Fixation of Upper and Lower Extremity FractureswirasenaNo ratings yet
- Mutifocal FracturesDocument4 pagesMutifocal FracturesElmer NarvaezNo ratings yet
- The Management of Distal Ulnar Fractures in Adults PDFDocument9 pagesThe Management of Distal Ulnar Fractures in Adults PDFBETHANo ratings yet
- Classifications of Intertrochanteric Fractures and Their Clinical ImportanceDocument6 pagesClassifications of Intertrochanteric Fractures and Their Clinical ImportanceJuan Pablo Sandoval BrionesNo ratings yet
- Acta Orthopaedica Et Traumatologica Turcica: Kenan Koca, Yusuf Erdem, Ça Gri Neyis Ci, Omer Ers enDocument4 pagesActa Orthopaedica Et Traumatologica Turcica: Kenan Koca, Yusuf Erdem, Ça Gri Neyis Ci, Omer Ers enIacob RoxanaNo ratings yet
- Perry2008 2Document12 pagesPerry2008 2luis castroNo ratings yet
- Bsms 1Document3 pagesBsms 1Filip starcevicNo ratings yet
- Mar2012 CC SkendzelDocument9 pagesMar2012 CC SkendzelJavierLarenasNo ratings yet
- Femoral Neck Fractures in Young Patients State Of.3Document5 pagesFemoral Neck Fractures in Young Patients State Of.3Rizwan Ahamed T ANo ratings yet
- Rib FractureDocument6 pagesRib FracturenasyilaputriNo ratings yet
- Complex Elbow Instability: Matthew Dipaola, MD, William B. Geissler, MD, A. Lee Osterman, MDDocument14 pagesComplex Elbow Instability: Matthew Dipaola, MD, William B. Geissler, MD, A. Lee Osterman, MDAndrea Z MilanoNo ratings yet
- SUBTDocument7 pagesSUBTJandira SalvadorNo ratings yet
- Fractures of The Middle Third of The Facial SkeletonDocument7 pagesFractures of The Middle Third of The Facial SkeletonMahendra Perumal50% (2)
- 1.management of Mandibular Condyle Fractures A ReviewDocument6 pages1.management of Mandibular Condyle Fractures A ReviewNisa RohmaNo ratings yet
- Acutrak Fixation of Comminuted Distal Radial FracturesDocument4 pagesAcutrak Fixation of Comminuted Distal Radial Fracturessanjay chhawraNo ratings yet
- 224 Closed Manipulation Casting of Distal Radius Fractures Fernandez DL 2005 Hand Clin p307-316 PDFDocument10 pages224 Closed Manipulation Casting of Distal Radius Fractures Fernandez DL 2005 Hand Clin p307-316 PDFanindyadputriNo ratings yet
- D5DADocument3 pagesD5DAdemoaccount demoNo ratings yet
- Pelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDFDocument11 pagesPelvic Fractures. Part 2. Contemporary Indications and Techniques For Definitive Surgical Management PDFJulio Cesar Guillen MoralesNo ratings yet
- Exposure Coronoid FXDocument9 pagesExposure Coronoid FXGiulio PriftiNo ratings yet
- 1 Principles of Internal Fixation: 1.1.1 Mechanical Properties of BoneDocument29 pages1 Principles of Internal Fixation: 1.1.1 Mechanical Properties of BoneCarlos CalderonNo ratings yet
- Hombro Inlges PDFDocument6 pagesHombro Inlges PDFOscar Segun DoNo ratings yet
- Dynamic External Fixation For Proximal Interphalangeal Fracture-DislocationsDocument9 pagesDynamic External Fixation For Proximal Interphalangeal Fracture-DislocationsrifkizidnyNo ratings yet
- Corelation of The Changes Between The Iridocorneal - Angle and Other Paramet E Rs at The Neovascular GlaucomaDocument25 pagesCorelation of The Changes Between The Iridocorneal - Angle and Other Paramet E Rs at The Neovascular GlaucomaAJVAZI100% (1)
- CPS ReportDocument4 pagesCPS ReportWXYZ-TV Channel 7 DetroitNo ratings yet
- Weight Bearing As Tolerated: Knee Replacement Exercise BookletDocument33 pagesWeight Bearing As Tolerated: Knee Replacement Exercise BookletRAGHAVNo ratings yet
- Wheat Flour Bussines Plan 2Document22 pagesWheat Flour Bussines Plan 2Yoseph Melesse100% (9)
- Classification of Drugs of AbuseDocument3 pagesClassification of Drugs of AbuseArlanLaderasManhicNo ratings yet
- Learner DiversityDocument1 pageLearner DiversityHenry Buemio100% (1)
- Catch Up Fridays Lesson PlanDocument2 pagesCatch Up Fridays Lesson PlanJedison IlocsoNo ratings yet
- Thesis StatementDocument15 pagesThesis StatementJos50% (2)
- Vent Weaning Ped22Document9 pagesVent Weaning Ped22Obed AhumadaNo ratings yet
- Paridhi English LanguageDocument7 pagesParidhi English LanguageKasturi GhoshNo ratings yet
- Working While Disabled: How We Can Help: SSA - GovDocument23 pagesWorking While Disabled: How We Can Help: SSA - GovKimberly Love AlgerNo ratings yet
- Ananda DheaDocument11 pagesAnanda DheadindacrusitaNo ratings yet
- Tor Proyek Stunting-BangdaDocument26 pagesTor Proyek Stunting-BangdaKiky Nurfayanti Denra'No ratings yet
- Organizational Transactional Analysis As PDFDocument10 pagesOrganizational Transactional Analysis As PDFAlexandr KachenovskyNo ratings yet
- Position Paper About Legalization of Marijuana in The PhilippinesDocument2 pagesPosition Paper About Legalization of Marijuana in The PhilippinesHabibi Waishu93% (14)
- Smoking With JJ ResearchDocument17 pagesSmoking With JJ ResearchKittiwin VongsakulNo ratings yet
- Rad 97Document188 pagesRad 97Ahmed BadranNo ratings yet
- Lifting and Basic Life SupportDocument37 pagesLifting and Basic Life SupportmijaNo ratings yet
- Eldorado Tool & Manufacturing Company LTD Job DescriptionDocument1 pageEldorado Tool & Manufacturing Company LTD Job DescriptionEthan StoneNo ratings yet
- Philippine Navy Naval Installation Command Naval Installation and Facilities-National Capital RegionDocument9 pagesPhilippine Navy Naval Installation Command Naval Installation and Facilities-National Capital RegionDuchesne San JoseNo ratings yet
- S1 - Opening Statement Access & Egress: Health & Safety Risk Management SystemDocument4 pagesS1 - Opening Statement Access & Egress: Health & Safety Risk Management SystemBruno NwarieNo ratings yet
- Using Secondary Data in Doctoral Research: by Jim Goes and Marilyn SimonDocument3 pagesUsing Secondary Data in Doctoral Research: by Jim Goes and Marilyn SimonSon AdamNo ratings yet
- Child Safety PDFDocument240 pagesChild Safety PDFVaibhav AgarwalNo ratings yet
- COMSECXDocument5 pagesCOMSECXJoseph CruzNo ratings yet
- Metanoia: Reflect - Reform - RenewDocument39 pagesMetanoia: Reflect - Reform - RenewLJ ZamoraNo ratings yet
- hdf492 Portfolio PresentationDocument14 pageshdf492 Portfolio Presentationapi-403412647No ratings yet
- DR M Javed Aftab - 2020Document9 pagesDR M Javed Aftab - 2020Dr. Muhammad Javed AftabNo ratings yet
- IV Fluids ChartDocument1 pageIV Fluids Chartzahidtaniv71% (7)
- WNL Junk Food Marketing at The Olympics UppDocument5 pagesWNL Junk Food Marketing at The Olympics UppAndrzejNo ratings yet
- ResearchDocument210 pagesResearchBurn CalapardoNo ratings yet
- To Engineer Is Human: The Role of Failure in Successful DesignFrom EverandTo Engineer Is Human: The Role of Failure in Successful DesignRating: 4 out of 5 stars4/5 (138)
- The Things We Make: The Unknown History of Invention from Cathedrals to Soda Cans (Father's Day Gift for Science and Engineering Curious Dads)From EverandThe Things We Make: The Unknown History of Invention from Cathedrals to Soda Cans (Father's Day Gift for Science and Engineering Curious Dads)No ratings yet
- Composite Structures of Steel and Concrete: Beams, Slabs, Columns and Frames for BuildingsFrom EverandComposite Structures of Steel and Concrete: Beams, Slabs, Columns and Frames for BuildingsNo ratings yet
- The Things We Make: The Unknown History of Invention from Cathedrals to Soda CansFrom EverandThe Things We Make: The Unknown History of Invention from Cathedrals to Soda CansRating: 4.5 out of 5 stars4.5/5 (21)
- Rocks and Minerals of The World: Geology for Kids - Minerology and SedimentologyFrom EverandRocks and Minerals of The World: Geology for Kids - Minerology and SedimentologyRating: 4.5 out of 5 stars4.5/5 (5)
- Skyway: The True Story of Tampa Bay's Signature Bridge and the Man Who Brought It DownFrom EverandSkyway: The True Story of Tampa Bay's Signature Bridge and the Man Who Brought It DownNo ratings yet
- Troubleshooting and Repair of Diesel EnginesFrom EverandTroubleshooting and Repair of Diesel EnginesRating: 1.5 out of 5 stars1.5/5 (2)
- Crossings: How Road Ecology Is Shaping the Future of Our PlanetFrom EverandCrossings: How Road Ecology Is Shaping the Future of Our PlanetRating: 4.5 out of 5 stars4.5/5 (10)
- The Great Bridge: The Epic Story of the Building of the Brooklyn BridgeFrom EverandThe Great Bridge: The Epic Story of the Building of the Brooklyn BridgeRating: 4.5 out of 5 stars4.5/5 (59)
- Structural Cross Sections: Analysis and DesignFrom EverandStructural Cross Sections: Analysis and DesignRating: 4.5 out of 5 stars4.5/5 (19)
- Finite Element Analysis and Design of Steel and Steel–Concrete Composite BridgesFrom EverandFinite Element Analysis and Design of Steel and Steel–Concrete Composite BridgesNo ratings yet
- Compendium of Best Practices in Road Asset ManagementFrom EverandCompendium of Best Practices in Road Asset ManagementNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Summary of Taiichi Ohno's Taiichi Ohno's Workplace ManagementFrom EverandSummary of Taiichi Ohno's Taiichi Ohno's Workplace ManagementNo ratings yet
- Rock Fracture and Blasting: Theory and ApplicationsFrom EverandRock Fracture and Blasting: Theory and ApplicationsRating: 5 out of 5 stars5/5 (2)
- Transport Phenomena in Heat and Mass TransferFrom EverandTransport Phenomena in Heat and Mass TransferJ.A. ReizesRating: 5 out of 5 stars5/5 (1)
- Roads: An Anthropology of Infrastructure and ExpertiseFrom EverandRoads: An Anthropology of Infrastructure and ExpertiseRating: 5 out of 5 stars5/5 (2)