You might also like
- Notice 15 2 2021 NewDocument1 pageNotice 15 2 2021 NewMahmood RahmanNo ratings yet
- Fellows Wealfare Rules 2010Document6 pagesFellows Wealfare Rules 2010Mahmood RahmanNo ratings yet
- 4021f699-27ae-4ef0-b5da-0a3acee772f5Document191 pages4021f699-27ae-4ef0-b5da-0a3acee772f5Mahmood RahmanNo ratings yet
- Frffi: ? Q.: FMRC Mmdicine XWDocument1 pageFrffi: ? Q.: FMRC Mmdicine XWMahmood RahmanNo ratings yet
- 3366332Document5 pages3366332Mahmood RahmanNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Antidepressant MCQs Group 2Document4 pagesAntidepressant MCQs Group 2Ayesha Ayesha100% (1)
- Safety Comparison of NSAIDsDocument16 pagesSafety Comparison of NSAIDsSuraj SubediNo ratings yet
- Classification of Drugs of AbuseDocument3 pagesClassification of Drugs of AbuseArlanLaderasManhicNo ratings yet
- LASA 16.4.2021 SYRUP and OthersDocument10 pagesLASA 16.4.2021 SYRUP and OthersANISNo ratings yet
- Hyoscine-N-butylbromide Perindopril Aspirin Simvastatin / Lovastatin Betahistine Ranitidine LoratadineDocument1 pageHyoscine-N-butylbromide Perindopril Aspirin Simvastatin / Lovastatin Betahistine Ranitidine LoratadineAinaDamiaNo ratings yet
- 10 4292@wjgpt v8 I1 26Document14 pages10 4292@wjgpt v8 I1 26Syawal PratamaNo ratings yet
- HeroinDocument19 pagesHeroinZainurain Zainal AbidinNo ratings yet
- Drug and Alcohol Testing in The WorkplaceDocument16 pagesDrug and Alcohol Testing in The WorkplaceYasmin KayeNo ratings yet
- Pharmacology A - Sympathetic Drugs Reviewer Ver 2.0 PDFDocument2 pagesPharmacology A - Sympathetic Drugs Reviewer Ver 2.0 PDFJohn Benedict BondocNo ratings yet
- Toxi-Lab Product Catalog Email-New2009Document40 pagesToxi-Lab Product Catalog Email-New2009Rizki M H IndrawanNo ratings yet
- Drugs Q and ADocument5 pagesDrugs Q and ALicudine Hiasmin100% (2)
- Republic Act No 9165Document13 pagesRepublic Act No 9165Jess QuintanaNo ratings yet
- Don Pablo Lorenzo Memorial High SchoolDocument9 pagesDon Pablo Lorenzo Memorial High SchoolCeerwin YamsonNo ratings yet
- Psy240 Appendix D Drug Health Effects ScaleDocument1 pagePsy240 Appendix D Drug Health Effects ScaleTammy PoeNo ratings yet
- Drugs Causing PhotosensitivityDocument4 pagesDrugs Causing PhotosensitivityaloescreamNo ratings yet
- Pharmacology-I II Pharm.D. Question BankDocument6 pagesPharmacology-I II Pharm.D. Question BankAnanda Vijayasarathy100% (1)
- A CB Scoring 062712Document1 pageA CB Scoring 062712Condor7tNo ratings yet
- Medication Preparation Dosage Remarks: Antipyretic/AnalgesicDocument4 pagesMedication Preparation Dosage Remarks: Antipyretic/AnalgesicTIFFANIE CHRISTEL UYNo ratings yet
- Pharmacology Midterm BlueDocument5 pagesPharmacology Midterm BlueRhealyn LegaspiNo ratings yet
- Understanding Substance Abuse in AdolescentsDocument24 pagesUnderstanding Substance Abuse in AdolescentsJacqueline MansillaNo ratings yet
- Medication20quizzes 12028429Document2 pagesMedication20quizzes 12028429DurgaNadellaNo ratings yet
- Missouri Counties Sue Drug Companies Over Opioid CrisisDocument274 pagesMissouri Counties Sue Drug Companies Over Opioid CrisisSam ClancyNo ratings yet
- HOOD COUNTY - Tolar ISD - 1996 Texas School Survey of Drug and Alcohol UseDocument6 pagesHOOD COUNTY - Tolar ISD - 1996 Texas School Survey of Drug and Alcohol UseTexas School Survey of Drug and Alcohol UseNo ratings yet
- Kratom Proposed Schedule I RuleDocument21 pagesKratom Proposed Schedule I RuleJamesNo ratings yet
- Drug & Alcohol Awareness: Employee TrainingDocument58 pagesDrug & Alcohol Awareness: Employee TrainingconsiNo ratings yet
- Cdi Lecture 1Document10 pagesCdi Lecture 1TJ del MarNo ratings yet
- Jurnal ReadingDocument13 pagesJurnal Readingeliamegasari01No ratings yet
- Devi Ratnasari - Obat Golongan NSAIDDocument2 pagesDevi Ratnasari - Obat Golongan NSAIDDevi RatnasariNo ratings yet
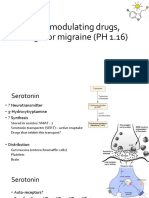
- 5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)Document13 pages5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)shruti sangwanNo ratings yet
- Unitatea de Măsură Cantitate A Preț Unitar, LeiDocument14 pagesUnitatea de Măsură Cantitate A Preț Unitar, LeivictorNo ratings yet