You might also like
- Cardiopulmonary PhysiotherapyDocument181 pagesCardiopulmonary PhysiotherapyOana Moza100% (3)
- Nursing Care Plan - ProdigalidadDocument5 pagesNursing Care Plan - ProdigalidadZxiayieee JeonNo ratings yet
- Case Mapping NCPDocument4 pagesCase Mapping NCPTey PauleNo ratings yet
- Appendix B Nursing Care Plan Clinical Portait Assessment: Received PatientDocument14 pagesAppendix B Nursing Care Plan Clinical Portait Assessment: Received Patientjopearl18No ratings yet
- Chapter 3Document3 pagesChapter 3Miggy EstoniloNo ratings yet
- Barecuatro Module3 FdarDocument2 pagesBarecuatro Module3 FdarANGELICA CLAIRE BARECUATRONo ratings yet
- NCP Altered ComfortDocument2 pagesNCP Altered ComfortMadz Tajal0% (1)
- NCMB 316 Assignment NCP Part 2Document3 pagesNCMB 316 Assignment NCP Part 2I'm a PepegaNo ratings yet
- Burn - Daily Physical AssessmentDocument8 pagesBurn - Daily Physical AssessmentkrishcelNo ratings yet
- NCP - BSN12F - Pumbaya (Module 4)Document3 pagesNCP - BSN12F - Pumbaya (Module 4)Ellah PumbayaNo ratings yet
- Ha - Finals Lab ManualDocument24 pagesHa - Finals Lab ManualSamantha AquinoNo ratings yet
- Noted Persistent Vaginal Bleeding, Soft Abdomen. Directions: Make A Nursing Care Plan Based On The Scenario GivenDocument2 pagesNoted Persistent Vaginal Bleeding, Soft Abdomen. Directions: Make A Nursing Care Plan Based On The Scenario GivenMarie PotayreNo ratings yet
- 1o - Romano Murcia LodoviceDocument4 pages1o - Romano Murcia LodoviceJilliary AlexandraNo ratings yet
- Rle 101Document15 pagesRle 101Fea Marielle MacapayadNo ratings yet
- Kim - Physical AssessmentDocument3 pagesKim - Physical AssessmentMaria Elvira Abrogena DuadNo ratings yet
- NCP Requirements RleDocument7 pagesNCP Requirements RleZymer Lee AbasoloNo ratings yet
- Subjective:: Davao Doctor'S College Nursing Program Nursing Care PlanDocument4 pagesSubjective:: Davao Doctor'S College Nursing Program Nursing Care PlanJEVEE JEAN BETTERNo ratings yet
- OBAssessment Tool Guidein HADocument9 pagesOBAssessment Tool Guidein HAShawn MichaelNo ratings yet
- NCP For UDHDocument3 pagesNCP For UDHTomohiro HorieNo ratings yet
- NCP For PostpartumDocument9 pagesNCP For PostpartumYzel Vasquez AdavanNo ratings yet
- 1BSN3 GRP 2 Worksheet 3Document5 pages1BSN3 GRP 2 Worksheet 3ysa.antonio12No ratings yet
- Fernandez 1b NCPDocument7 pagesFernandez 1b NCPToni Marie FernandezNo ratings yet
- Pakanna-BSN2D Chunk-2-Vs.-01Document8 pagesPakanna-BSN2D Chunk-2-Vs.-01FATIMA SHANNON INDASAN. PAKANNANo ratings yet
- Forro Intestinal ObstructionDocument3 pagesForro Intestinal ObstructionShiehan Mae ForroNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainChristian De GuzmanNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainSheene Lysethea Sioteco AguilosNo ratings yet
- Nursing Diagnosis Objectiv eDocument4 pagesNursing Diagnosis Objectiv eرهف الرفاعيNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationJonna Mae TurquezaNo ratings yet
- Health Perception - Health Management Pattern:: Babinski Reflex and Neck ControlDocument2 pagesHealth Perception - Health Management Pattern:: Babinski Reflex and Neck ControlBenjie DimayacyacNo ratings yet
- Areas Functional Pattern GordonsDocument2 pagesAreas Functional Pattern GordonsBenjie DimayacyacNo ratings yet
- Viñas - NCP (Finals)Document2 pagesViñas - NCP (Finals)Azy Joy ViñasNo ratings yet
- ASSESSMENT S: "Nanghihina Ako, Hindi Ko Magawa Yung Mga GustoDocument1 pageASSESSMENT S: "Nanghihina Ako, Hindi Ko Magawa Yung Mga GustoCherie MayNo ratings yet
- Case NCP MelbaDocument2 pagesCase NCP MelbabambheesyeoboNo ratings yet
- Related Learning Experience Fundamentals in Nursing 4 RotationDocument3 pagesRelated Learning Experience Fundamentals in Nursing 4 RotationMark Eliezer CulasingNo ratings yet
- Final Nursing Care PlanDocument7 pagesFinal Nursing Care PlanKatherine BellezaNo ratings yet
- Pedia NCPDocument8 pagesPedia NCPFrancheska Nicole Delos SantosNo ratings yet
- NCP Conception ActivityDocument3 pagesNCP Conception ActivityMarl TanNo ratings yet
- Actual NCPDocument2 pagesActual NCPJhomines NialaNo ratings yet
- 5 BubbleheDocument1 page5 BubbleheErick SumicadNo ratings yet
- Nursing Care Plan: Western Mindanao State University College of NursingDocument11 pagesNursing Care Plan: Western Mindanao State University College of NursingPatricia VasquezNo ratings yet
- Silliman University: Nursing Care Plan During DeliveryDocument12 pagesSilliman University: Nursing Care Plan During DeliveryShandle Dynne BaenaNo ratings yet
- Cmca Rle 13Document126 pagesCmca Rle 13Carl Josef C. GarciaNo ratings yet
- TTP Care Plan 1 JevansDocument8 pagesTTP Care Plan 1 Jevansapi-439893609No ratings yet
- Scenario:: Pain AssessmentDocument7 pagesScenario:: Pain AssessmentLouwella RamosNo ratings yet
- Nursing-Care-Plan-J P VDocument8 pagesNursing-Care-Plan-J P VMa. Ferimi Gleam BajadoNo ratings yet
- NCPDocument18 pagesNCPStephanie Villanueva AdvinculaNo ratings yet
- نسخة case med and ncpDocument8 pagesنسخة case med and ncpBudoor AlatawiNo ratings yet
- Ectopic PregnancyDocument2 pagesEctopic PregnancyKim GalamgamNo ratings yet
- CRT Week 1Document9 pagesCRT Week 1api-643868511No ratings yet
- Group 4 NCPDocument9 pagesGroup 4 NCPJames De VeraNo ratings yet
- NCP Kenezo, Female 17Document2 pagesNCP Kenezo, Female 17labanesstephanyNo ratings yet
- Group A NCP and Soapie ChartingDocument10 pagesGroup A NCP and Soapie ChartingBethrice MelegritoNo ratings yet
- Case 3Document11 pagesCase 3Pam RuizNo ratings yet
- Larita, Anna V. BSN-2A Nursing Care Plan NCM 107Document2 pagesLarita, Anna V. BSN-2A Nursing Care Plan NCM 107Anna LaritaNo ratings yet
- Salawie 8 NCP Cancer Diseases MedSurgDocument16 pagesSalawie 8 NCP Cancer Diseases MedSurgAMEER MUHMIEN JALMAANI. LERIOSNo ratings yet
- NCP Ruq PainDocument3 pagesNCP Ruq PainKristine YoungNo ratings yet
- NCP & DSDocument4 pagesNCP & DSKyla Marie TejadaNo ratings yet
- Shoulder DystociaDocument9 pagesShoulder DystociaSoriao, Lovely Rose V.100% (1)
- AppendicitisDocument7 pagesAppendicitisRobert de Guzman Jr.No ratings yet
- Background of The Country Foreign PoliciesDocument5 pagesBackground of The Country Foreign PoliciesIvan Laurentine AceretNo ratings yet
- Perspective: SociologicalDocument14 pagesPerspective: SociologicalIvan Laurentine AceretNo ratings yet
- A Champ Is A Dreamer Who Never Gives Up".: Best Wishes To AllDocument1 pageA Champ Is A Dreamer Who Never Gives Up".: Best Wishes To AllIvan Laurentine AceretNo ratings yet
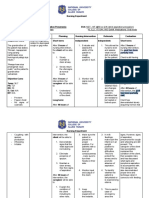
- VIII. Nursing Care Plan: Assessment Diagnosis Planning Intervention Rationlae EvaluationDocument9 pagesVIII. Nursing Care Plan: Assessment Diagnosis Planning Intervention Rationlae EvaluationIvan Laurentine AceretNo ratings yet
- Case Study of Chronic Hypertension With Superimposed Preeclampsia (Obstetrical Complex)Document13 pagesCase Study of Chronic Hypertension With Superimposed Preeclampsia (Obstetrical Complex)Ivan Laurentine AceretNo ratings yet
- This Study Resource Was: Client HistoryDocument1 pageThis Study Resource Was: Client HistoryIvan Laurentine AceretNo ratings yet
- GCS 3Ps Anaphy PathophysiologyDocument11 pagesGCS 3Ps Anaphy PathophysiologyIvan Laurentine AceretNo ratings yet
- Pre Eclampsia Case StudyDocument11 pagesPre Eclampsia Case StudyIvan Laurentine AceretNo ratings yet
- Group 2. Ectopic PregnancyDocument61 pagesGroup 2. Ectopic PregnancyIvan Laurentine Aceret100% (1)
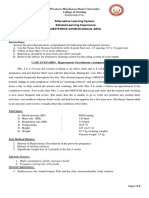
- For Female: Supine, With Knees Flexed, Feet About 2 Feet Apart, and Hips Slightly ExternallyDocument3 pagesFor Female: Supine, With Knees Flexed, Feet About 2 Feet Apart, and Hips Slightly ExternallyIvan Laurentine AceretNo ratings yet
- Grp5 Placenta Previa FINAL With RevisionsDocument64 pagesGrp5 Placenta Previa FINAL With RevisionsIvan Laurentine AceretNo ratings yet
- RootDocument119 pagesRootเทพนิมิตร สมภักดีNo ratings yet
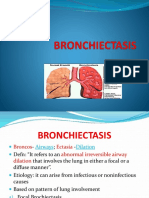
- Case Study: BronchiectasisDocument5 pagesCase Study: BronchiectasisHanna Mae HernandezNo ratings yet
- CH 13 Respiratory-SystemDocument88 pagesCH 13 Respiratory-SystemAntonio Calleja II100% (1)
- Anatomy and PhysiologyDocument7 pagesAnatomy and PhysiologyBlessyl Mae EstenzoNo ratings yet
- Pne67!2!08pozzi ReviewDocument10 pagesPne67!2!08pozzi ReviewmunirdayaniNo ratings yet
- RRT Clinical Application Gas LawDocument15 pagesRRT Clinical Application Gas LawsplouisscNo ratings yet
- Human Respiratory System Aniket DasDocument11 pagesHuman Respiratory System Aniket DasChep KepNo ratings yet
- Respiratory SystemDocument19 pagesRespiratory SystemayuNo ratings yet
- Imaging - Chest RadiologyDocument78 pagesImaging - Chest Radiologymoggs7No ratings yet
- Evaluation of Compliance With Standard Criteria For Postero-Anterior (Pa) Chest Radiographs in Parklane Hospital EnuguDocument37 pagesEvaluation of Compliance With Standard Criteria For Postero-Anterior (Pa) Chest Radiographs in Parklane Hospital EnuguLavinia VictorNo ratings yet
- Science9 q1 Mod1 SDOv2 1Document32 pagesScience9 q1 Mod1 SDOv2 1Amélie KatanaNo ratings yet
- Med Surg Respiratory SystemDocument173 pagesMed Surg Respiratory Systembamfalcon100% (4)
- Answers To Eocqs: Notes About Mark SchemesDocument3 pagesAnswers To Eocqs: Notes About Mark SchemesAayush GauchanNo ratings yet
- BronchiectasisDocument36 pagesBronchiectasisMujeeb AfzalNo ratings yet
- The Respiratory System: Asst. Prof. Dr. Ghaith Ali Jasim Al ZubaidyDocument106 pagesThe Respiratory System: Asst. Prof. Dr. Ghaith Ali Jasim Al Zubaidydeeqomaxamed1133No ratings yet
- BC (H) - IV-Human Physiology, Respiratory System-1 & 2Document45 pagesBC (H) - IV-Human Physiology, Respiratory System-1 & 2sidra nazirNo ratings yet
- Module 4 Respiratory SystemDocument8 pagesModule 4 Respiratory SystemJake Donely C. PaduaNo ratings yet
- Test AMG Sem II EnglezaDocument3 pagesTest AMG Sem II EnglezaCCCAXANo ratings yet
- Respiratory System: VocabularyDocument4 pagesRespiratory System: VocabularyFely NatadNo ratings yet
- New A Level Teacher Notes Part 2Document161 pagesNew A Level Teacher Notes Part 2farmerllama.gkNo ratings yet
- Jurnal Bronchitis Dengan AsmaDocument5 pagesJurnal Bronchitis Dengan AsmaMauLan SaputraNo ratings yet
- Systems Module 12Document40 pagesSystems Module 12Richiel Angulo SungaNo ratings yet
- The Design of The Avian Respiratory System: Development and Morphology - A Review A.D.FirdousDocument24 pagesThe Design of The Avian Respiratory System: Development and Morphology - A Review A.D.FirdousIndian Journal of Veterinary and Animal Sciences RNo ratings yet
- Anatomy & Physiology of Respiratory SystemDocument12 pagesAnatomy & Physiology of Respiratory SystemDgjj CompuiterNo ratings yet
- Draft April 29, 2014: Unit 1 Living Things and Their EnvironmentDocument293 pagesDraft April 29, 2014: Unit 1 Living Things and Their EnvironmentJeanylyn MelgarNo ratings yet
- CHAPTER-9, Respiration in Organisms.Document3 pagesCHAPTER-9, Respiration in Organisms.HarshitAhelani2379ScribdNo ratings yet
- 2 - Respiratory SystemDocument9 pages2 - Respiratory SystemHannah Grace CorveraNo ratings yet
- Anatomy Quizbook Volume 2 Head and NeckDocument92 pagesAnatomy Quizbook Volume 2 Head and NeckSakhile Ndlovu100% (1)
- Med TermDocument93 pagesMed TermCEFI Office for Research and PublicationsNo ratings yet