You might also like
- Vietnam War Women Veterans Signs and Symptoms of Long-Lasting Physical and Psychological Injuries in Female Vietnam VeteransFrom EverandVietnam War Women Veterans Signs and Symptoms of Long-Lasting Physical and Psychological Injuries in Female Vietnam VeteransNo ratings yet
- WomeninMilitary PDFDocument10 pagesWomeninMilitary PDFAnksheNo ratings yet
- Relationships among Combat Experience, Moral Injury, and Mental Health OutcomesFrom EverandRelationships among Combat Experience, Moral Injury, and Mental Health OutcomesNo ratings yet
- After Every Darkness Is Light Resilient Afghan Women Coping With Violence and ImmigrationDocument12 pagesAfter Every Darkness Is Light Resilient Afghan Women Coping With Violence and ImmigrationJose GuardadoNo ratings yet
- Psychological Trauma and Ptsd/Soldiers (Child)From EverandPsychological Trauma and Ptsd/Soldiers (Child)No ratings yet
- Women in MilitaryDocument12 pagesWomen in Militaryapi-311829801No ratings yet
- Differential Vulnerability?Document24 pagesDifferential Vulnerability?Daniela RochaNo ratings yet
- The Influence of Veteran Status, Psychiatric Diagnosis, and Traumatic Brain Injury On Inadequate SleepDocument20 pagesThe Influence of Veteran Status, Psychiatric Diagnosis, and Traumatic Brain Injury On Inadequate SleepdewaNo ratings yet
- Integrating Females into the U.S. ArmyDocument14 pagesIntegrating Females into the U.S. ArmyMorgan Van Epp CutlipNo ratings yet
- Rita Paper Part IIDocument11 pagesRita Paper Part IIgkempf10No ratings yet
- Rhetorical Analysis Zombie FinalDocument12 pagesRhetorical Analysis Zombie Finalapi-610120761No ratings yet
- Amara Roles and Challenges of WomenDocument16 pagesAmara Roles and Challenges of WomenEng MohammedNo ratings yet
- Clinical Psychology Review: Amy E. Street, Dawne Vogt, Lissa DutraDocument10 pagesClinical Psychology Review: Amy E. Street, Dawne Vogt, Lissa Dutraapi-234667778No ratings yet
- Reintegration of Ex-Military Personnel With Civil Life-A Social Issue and Big Challenge: An Empirical StudyDocument15 pagesReintegration of Ex-Military Personnel With Civil Life-A Social Issue and Big Challenge: An Empirical Studymohammad shahidullahNo ratings yet
- Sean Borden - Research Paper LsaDocument13 pagesSean Borden - Research Paper Lsaapi-535842202No ratings yet
- Korean Comfort Women Trauma and Recovery: Into An Unforgivable PastDocument12 pagesKorean Comfort Women Trauma and Recovery: Into An Unforgivable PastMinahilTariqNo ratings yet
- Child Soldiering: Impact On Childhood Development and Learning CapacityDocument23 pagesChild Soldiering: Impact On Childhood Development and Learning CapacityPEIC Data0% (1)
- ResearchhomelessfvetsDocument7 pagesResearchhomelessfvetsapi-283974130No ratings yet
- Annotated BibsDocument5 pagesAnnotated Bibsapi-296636859No ratings yet
- Trauma and ResilienceDocument9 pagesTrauma and ResilienceMinahilTariqNo ratings yet
- ProposalDocument18 pagesProposalThulasivanthana UdhayashankarNo ratings yet
- Stress and Emotional Well-Being in Military Organizations: Digitalcommons@University of Nebraska - LincolnDocument31 pagesStress and Emotional Well-Being in Military Organizations: Digitalcommons@University of Nebraska - LincolnAufar AdikusumoNo ratings yet
- Spiro - HRS DMC Paper On Military ServiceDocument25 pagesSpiro - HRS DMC Paper On Military ServiceShopnil SarkarNo ratings yet
- Iwa Final Draft 2Document11 pagesIwa Final Draft 2api-669709143No ratings yet
- FulltextDocument31 pagesFulltextAna- Diana BalcanNo ratings yet
- HeenancDocument12 pagesHeenancapi-457789068No ratings yet
- Military Culture and The Transition To CivilianDocument5 pagesMilitary Culture and The Transition To CivilianJian Carla ManuyagNo ratings yet
- Women in Military DebateDocument15 pagesWomen in Military DebateRebecca Isabel Ponce Cepeda100% (1)
- A New AgeDocument8 pagesA New Ageapi-253343239No ratings yet
- Annotated Bibliography - Effect of War On ChildrenDocument10 pagesAnnotated Bibliography - Effect of War On ChildrenaiizNo ratings yet
- Women at WarDocument9 pagesWomen at WarArina PredaNo ratings yet
- Psychological Debriefing (PD) of Trauma: A Proposed Model For AfricaDocument16 pagesPsychological Debriefing (PD) of Trauma: A Proposed Model For AfricaRAIZA CANILLASNo ratings yet
- Female Participations in UN Peacekeeping MissionsDocument7 pagesFemale Participations in UN Peacekeeping MissionsarcherselevatorsNo ratings yet
- PTSD Women Combat VeteransDocument6 pagesPTSD Women Combat VeteransMisty JaneNo ratings yet
- For Many Injured Veterans, A Lifetime of Consequences: Social & Demographic TrendsDocument20 pagesFor Many Injured Veterans, A Lifetime of Consequences: Social & Demographic TrendsJimNo ratings yet
- Sexual VictimataionDocument6 pagesSexual VictimataionAnonymous pUMYaiXBlWNo ratings yet
- Research Assignment 7b Holz 2Document19 pagesResearch Assignment 7b Holz 2api-251823562No ratings yet
- Survival in Times of Adversity Among Active Military Personnel With Local-Armed Conflict ExposureDocument12 pagesSurvival in Times of Adversity Among Active Military Personnel With Local-Armed Conflict ExposurePsychology and Education: A Multidisciplinary JournalNo ratings yet
- Unequal Burden of War (Publisher Version)Document33 pagesUnequal Burden of War (Publisher Version)Maaz AlamNo ratings yet
- By Maysa Hassaan Sayed: Women's Perception Regarding Domestic Violence Protocol of ThesisDocument13 pagesBy Maysa Hassaan Sayed: Women's Perception Regarding Domestic Violence Protocol of ThesisDrBasiony Abo FaresNo ratings yet
- Military Misogyny Final 2Document8 pagesMilitary Misogyny Final 2api-432201093No ratings yet
- The Cost-Effectiveness of Psychotherapy For The MaDocument22 pagesThe Cost-Effectiveness of Psychotherapy For The MaSerraNo ratings yet
- Vealey Beth-Ann PHDDocument163 pagesVealey Beth-Ann PHDCDR SalamanderNo ratings yet
- Cultural Immersion: Military Culture: Running Head: 1Document13 pagesCultural Immersion: Military Culture: Running Head: 1JLPNo ratings yet
- Skylar Mills Rogers Government 18 October 2017 Veterans Suicide Act of 2017Document6 pagesSkylar Mills Rogers Government 18 October 2017 Veterans Suicide Act of 2017api-336683893No ratings yet
- RH in Conflict SettingsDocument23 pagesRH in Conflict Settingsamani_elkhatimNo ratings yet
- 244-Orginal Articles-1504-1-10-20211227Document15 pages244-Orginal Articles-1504-1-10-20211227FikirNo ratings yet
- Espy 5323-Research PaperDocument12 pagesEspy 5323-Research Paperapi-284037288No ratings yet
- Chapter 2Document15 pagesChapter 2Prince James Marcial AgoncilloNo ratings yet
- Depressive Symptomatology Among HIV-Positive Women in The Era of HAART: A Stress and Coping ModelDocument12 pagesDepressive Symptomatology Among HIV-Positive Women in The Era of HAART: A Stress and Coping ModelAudia SurachminNo ratings yet
- Women in Non Stated Millitary GroupsDocument2 pagesWomen in Non Stated Millitary Groupsfarzana youafNo ratings yet
- Wool Handler Veterans TestimonyDocument26 pagesWool Handler Veterans TestimonyPatricia DillonNo ratings yet
- Psychological Impact of Victims of War and Conflict Amrita RathiDocument4 pagesPsychological Impact of Victims of War and Conflict Amrita RathidaliNo ratings yet
- Soldiers Returning From WarDocument4 pagesSoldiers Returning From WarTroy Le PageNo ratings yet
- Prostitution in Five Countries: Violence and Post-Traumatic Stress DisorderDocument22 pagesProstitution in Five Countries: Violence and Post-Traumatic Stress DisorderMMMMMMMMMMNo ratings yet
- 2-Post-Traumatic Stress Reaction and Internally Displaced Persons A Psychosocial ApproachDocument18 pages2-Post-Traumatic Stress Reaction and Internally Displaced Persons A Psychosocial ApproachClinical and Counselling Psychology ReviewNo ratings yet
- Research Paper On PTSD and The Iraq WarDocument9 pagesResearch Paper On PTSD and The Iraq Warixevojrif100% (1)
- Essay 3 Final DraftDocument7 pagesEssay 3 Final Draftapi-581720582No ratings yet
- Stanley B hw410 Final ProdjectDocument12 pagesStanley B hw410 Final Prodjectapi-548868021No ratings yet
- Norris 2011Document15 pagesNorris 2011Sitti Rosdiana YahyaNo ratings yet
- Etica Cercetării Științifice În Domeniul Științelor Sociale: Revista Transilvania March 2019Document6 pagesEtica Cercetării Științifice În Domeniul Științelor Sociale: Revista Transilvania March 2019Ion BanariNo ratings yet
- EmotionalStability APJM2016Document29 pagesEmotionalStability APJM2016Alina CiobanuNo ratings yet
- Gender Stereotypes and The Evaluation of Men and Women in Military Training PDFDocument17 pagesGender Stereotypes and The Evaluation of Men and Women in Military Training PDFKatalin GyüsziNo ratings yet
- Article 20 Prof 2020 Baron 20Document29 pagesArticle 20 Prof 2020 Baron 20Relaxing music, Meditation & Sleep - Moon ChildNo ratings yet
- The Association of Anxiety and Depressive SymptomsDocument13 pagesThe Association of Anxiety and Depressive SymptomsAlina CiobanuNo ratings yet
- Frustrare in DelincventaDocument6 pagesFrustrare in DelincventaAlina CiobanuNo ratings yet
- Advantages and Barriers of Formative Assessment inDocument4 pagesAdvantages and Barriers of Formative Assessment inAlina CiobanuNo ratings yet
- SanguinarianDocument1 pageSanguinarianAna NickNo ratings yet
- Be It Enacted by The Senate and House of Representatives of The Philippines in CongressDocument414 pagesBe It Enacted by The Senate and House of Representatives of The Philippines in CongressyoungkimNo ratings yet
- The Mediating Role of Cognitive Reappraisal Between Childhood Physical Abuse and Substance Abuse Among Young Adult Residents in A Selected Treatment and Rehabilitation Center in BicutanDocument14 pagesThe Mediating Role of Cognitive Reappraisal Between Childhood Physical Abuse and Substance Abuse Among Young Adult Residents in A Selected Treatment and Rehabilitation Center in BicutanPsychology and Education: A Multidisciplinary JournalNo ratings yet
- How Music Affects Teenagers' Behavior and DevelopmentDocument3 pagesHow Music Affects Teenagers' Behavior and DevelopmentRina DzhuraNo ratings yet
- 02 Physical Activity and Psychological Well-BeingDocument218 pages02 Physical Activity and Psychological Well-BeingDimas PutraNo ratings yet
- Herbs To Break Habits Happy HerbDocument17 pagesHerbs To Break Habits Happy HerbCiprian Infj100% (1)
- Understanding Teen DepressionDocument38 pagesUnderstanding Teen DepressionMadiha KhadimNo ratings yet
- Theories of Drug Craving, Ancient and Modern: D. Colin DrummondDocument4 pagesTheories of Drug Craving, Ancient and Modern: D. Colin DrummondPonciano AlngogNo ratings yet
- 3.Hum-Controlling Drug Menace in India - MR - Sree KRISHNA BHARADWAJ HDocument6 pages3.Hum-Controlling Drug Menace in India - MR - Sree KRISHNA BHARADWAJ HImpact JournalsNo ratings yet
- Drug AddictionDocument7 pagesDrug AddictionJohn LoganNo ratings yet
- 2022 CIT Roadmap SlidesDocument27 pages2022 CIT Roadmap SlidesSam JacksonNo ratings yet
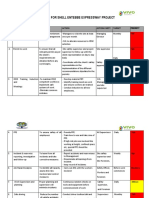
- Hsse Plan For Shell Entebbe Expressway Project: No Description Objective Action Action Party Target PriorityDocument5 pagesHsse Plan For Shell Entebbe Expressway Project: No Description Objective Action Action Party Target PriorityDENISNo ratings yet
- Australian Indigenous Mental Health Screening & Assessment ToolsDocument68 pagesAustralian Indigenous Mental Health Screening & Assessment ToolsAmitNo ratings yet
- Drugs AbuseDocument20 pagesDrugs AbuseKrishnaNo ratings yet
- Declare Health for Study in MalaysiaDocument1 pageDeclare Health for Study in MalaysiaMettaNo ratings yet
- Drug Abuse Essay - AlcoholismDocument5 pagesDrug Abuse Essay - Alcoholismapi-509288017No ratings yet
- Drug Use by Soldiers in The Vietnam WarDocument3 pagesDrug Use by Soldiers in The Vietnam WarVanish StarNo ratings yet
- EO Brgy Rehabilitation and Referral DeskDocument2 pagesEO Brgy Rehabilitation and Referral Deskbarangay413zone42100% (1)
- Fundamentals of Human DevelopmentDocument7 pagesFundamentals of Human DevelopmentJatin MakhijaniNo ratings yet
- Badac EoDocument3 pagesBadac EoRonabel CalicdanNo ratings yet
- Mental Status Exam Assessment GuideDocument3 pagesMental Status Exam Assessment GuideAmber Nicole HubbardNo ratings yet
- Fall Schedule 2010Document128 pagesFall Schedule 2010portlandccNo ratings yet
- Mental Health Nursing Module 1 - Introduction Student 2023Document44 pagesMental Health Nursing Module 1 - Introduction Student 2023Biology TutorNo ratings yet
- CMI Notes - June 2021 (Latest)Document146 pagesCMI Notes - June 2021 (Latest)HONG LIANG PERNNo ratings yet
- William T. O'Donohue, Michelle R. Byrd, Nicholas A. Cummings, Deborah A. Henderson - Behavioral Integrative Care - Treatments That Work in The Primary Care Setting (2004) PDFDocument412 pagesWilliam T. O'Donohue, Michelle R. Byrd, Nicholas A. Cummings, Deborah A. Henderson - Behavioral Integrative Care - Treatments That Work in The Primary Care Setting (2004) PDFSidarta RodriguesNo ratings yet
- Psych Nursing LectureDocument448 pagesPsych Nursing LectureCherry Ann Garcia DuranteNo ratings yet
- Counseling and Mental Health Care For Transgender PDFDocument72 pagesCounseling and Mental Health Care For Transgender PDFTherese EspinosaNo ratings yet
- Course Reflection Letter PDFDocument4 pagesCourse Reflection Letter PDFManisha SharmaNo ratings yet
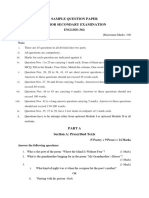
- Sample Question Paper Senior Secondary Examination: ENGLISHDocument24 pagesSample Question Paper Senior Secondary Examination: ENGLISHpriyanshu jainNo ratings yet
- Unit 4 Heath TopicDocument32 pagesUnit 4 Heath Topicralph allan bibatNo ratings yet
- High-Risers: Cabrini-Green and the Fate of American Public HousingFrom EverandHigh-Risers: Cabrini-Green and the Fate of American Public HousingNo ratings yet
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfFrom EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfRating: 5 out of 5 stars5/5 (36)
- Not a Crime to Be Poor: The Criminalization of Poverty in AmericaFrom EverandNot a Crime to Be Poor: The Criminalization of Poverty in AmericaRating: 4.5 out of 5 stars4.5/5 (37)
- The Meth Lunches: Food and Longing in an American CityFrom EverandThe Meth Lunches: Food and Longing in an American CityRating: 5 out of 5 stars5/5 (5)
- Nickel and Dimed: On (Not) Getting By in AmericaFrom EverandNickel and Dimed: On (Not) Getting By in AmericaRating: 4 out of 5 stars4/5 (186)
- Hillbilly Elegy: A Memoir of a Family and Culture in CrisisFrom EverandHillbilly Elegy: A Memoir of a Family and Culture in CrisisRating: 4 out of 5 stars4/5 (4284)
- Same Kind of Different As Me Movie Edition: A Modern-Day Slave, an International Art Dealer, and the Unlikely Woman Who Bound Them TogetherFrom EverandSame Kind of Different As Me Movie Edition: A Modern-Day Slave, an International Art Dealer, and the Unlikely Woman Who Bound Them TogetherRating: 4 out of 5 stars4/5 (685)
- Workin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherFrom EverandWorkin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherNo ratings yet
- The Great Displacement: Climate Change and the Next American MigrationFrom EverandThe Great Displacement: Climate Change and the Next American MigrationRating: 4 out of 5 stars4/5 (19)
- Poor Economics: A Radical Rethinking of the Way to Fight Global PovertyFrom EverandPoor Economics: A Radical Rethinking of the Way to Fight Global PovertyRating: 4.5 out of 5 stars4.5/5 (263)
- Who Really Owns Ireland: How we became tenants in our own land - and what we can do about itFrom EverandWho Really Owns Ireland: How we became tenants in our own land - and what we can do about itNo ratings yet
- Fucked at Birth: Recalibrating the American Dream for the 2020sFrom EverandFucked at Birth: Recalibrating the American Dream for the 2020sRating: 4 out of 5 stars4/5 (173)
- Heartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthFrom EverandHeartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthRating: 4 out of 5 stars4/5 (188)
- Skimmed: Breastfeeding, Race, and InjusticeFrom EverandSkimmed: Breastfeeding, Race, and InjusticeRating: 5 out of 5 stars5/5 (1)
- How the Poor Can Save Capitalism: Rebuilding the Path to the Middle ClassFrom EverandHow the Poor Can Save Capitalism: Rebuilding the Path to the Middle ClassRating: 5 out of 5 stars5/5 (6)
- Nickel and Dimed: On (Not) Getting By in AmericaFrom EverandNickel and Dimed: On (Not) Getting By in AmericaRating: 3.5 out of 5 stars3.5/5 (197)
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfFrom EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfRating: 4 out of 5 stars4/5 (126)
- The Great Displacement: Climate Change and the Next American MigrationFrom EverandThe Great Displacement: Climate Change and the Next American MigrationRating: 4.5 out of 5 stars4.5/5 (32)
- The Mole People: Life in the Tunnels Beneath New York CityFrom EverandThe Mole People: Life in the Tunnels Beneath New York CityRating: 3.5 out of 5 stars3.5/5 (190)
- This Is Ohio: The Overdose Crisis and the Front Lines of a New AmericaFrom EverandThis Is Ohio: The Overdose Crisis and the Front Lines of a New AmericaRating: 4 out of 5 stars4/5 (37)
- Alienated America: Why Some Places Thrive While Others CollapseFrom EverandAlienated America: Why Some Places Thrive While Others CollapseRating: 4 out of 5 stars4/5 (35)
- Superclass: The Global Power Elite and the World They Are MakingFrom EverandSuperclass: The Global Power Elite and the World They Are MakingRating: 3.5 out of 5 stars3.5/5 (32)