You might also like
- Soft Tissue Injuries and Injury Tolerance LevelsDocument12 pagesSoft Tissue Injuries and Injury Tolerance LevelsDeepsNo ratings yet
- Correlative Pathology and Biomechanics of Craniospinal Injuries A Post-Mortem Study of Fifty Fatal Cases and A Clinical Review of 300 Treated CasesDocument7 pagesCorrelative Pathology and Biomechanics of Craniospinal Injuries A Post-Mortem Study of Fifty Fatal Cases and A Clinical Review of 300 Treated CasesDeepsNo ratings yet
- Effect of A Protective Device in The Reduction of Head InjuryDocument11 pagesEffect of A Protective Device in The Reduction of Head InjuryDeepsNo ratings yet
- Field Investigations of The Injury Protection Offered by Some Energy Absorbing Steering SystemsDocument12 pagesField Investigations of The Injury Protection Offered by Some Energy Absorbing Steering SystemsDeepsNo ratings yet
- Engineering-Medical Analysis of Fatal and Non-Fatal Head Injuries of Helmeted Motorcycle VictimsDocument9 pagesEngineering-Medical Analysis of Fatal and Non-Fatal Head Injuries of Helmeted Motorcycle VictimsDeepsNo ratings yet
- Head and Spinal Injury Tolerance With No Direct Head ImpactDocument9 pagesHead and Spinal Injury Tolerance With No Direct Head ImpactDeepsNo ratings yet
- Experimental Trauma of Occipital ImpactsDocument13 pagesExperimental Trauma of Occipital ImpactsDeepsNo ratings yet
- Injury Patterns According To Crash ConfigurationDocument6 pagesInjury Patterns According To Crash ConfigurationDeepsNo ratings yet
- Studies of The Motion of The Brain at A Suddenly Applied Rotation of The SkullDocument8 pagesStudies of The Motion of The Brain at A Suddenly Applied Rotation of The SkullDeepsNo ratings yet
- Prototypes of Head Injuries Application To Animal ExperimentsDocument12 pagesPrototypes of Head Injuries Application To Animal ExperimentsDeepsNo ratings yet
- A Generation Model of Vehicle Crash Pulse For Injury Severity Prediction Based On A Typical SedanDocument5 pagesA Generation Model of Vehicle Crash Pulse For Injury Severity Prediction Based On A Typical SedanDeepsNo ratings yet
- The Effect of Seatback Stiffness and Collision Severity On The Dynamic Behaviour of The Head During WhiplashDocument10 pagesThe Effect of Seatback Stiffness and Collision Severity On The Dynamic Behaviour of The Head During WhiplashDeepsNo ratings yet
- Review of Head Injury Tolerance To Direct ImpactDocument18 pagesReview of Head Injury Tolerance To Direct ImpactDeepsNo ratings yet
- Development of A Generic Low Speed Rear Impact Pulse For Assessing Soft Tissue Neck Injury RiskDocument12 pagesDevelopment of A Generic Low Speed Rear Impact Pulse For Assessing Soft Tissue Neck Injury RiskDeepsNo ratings yet
- The Epidemiology of Injury - A ReviewDocument15 pagesThe Epidemiology of Injury - A ReviewDeepsNo ratings yet
- A Safety-Focused Vehicle Driving Strategy Towards Minimal Injury Severity in Imminent Collision ScenariosDocument4 pagesA Safety-Focused Vehicle Driving Strategy Towards Minimal Injury Severity in Imminent Collision ScenariosDeepsNo ratings yet
- A New Oblique Impact Test For Motorcycle HelmetsDocument3 pagesA New Oblique Impact Test For Motorcycle HelmetsDeepsNo ratings yet
- An Analysis of Fatal Car Crashes in Which The Victim Was Wearing A Seat BeltDocument10 pagesAn Analysis of Fatal Car Crashes in Which The Victim Was Wearing A Seat BeltDeepsNo ratings yet
- Key Words: Accelerations, Biomechanics, Kinematics, Neck, Occupants, Rear ImpactsDocument2 pagesKey Words: Accelerations, Biomechanics, Kinematics, Neck, Occupants, Rear ImpactsDeepsNo ratings yet
- Modelling Driver Cognitive Behaviours Under Critical Scenes Based On Deep LearningDocument4 pagesModelling Driver Cognitive Behaviours Under Critical Scenes Based On Deep LearningDeepsNo ratings yet
- Capturing Driver Evasive Manoeuvres in Pre-Crash Phases From Large-Scale Real-World Critical Scene VideosDocument4 pagesCapturing Driver Evasive Manoeuvres in Pre-Crash Phases From Large-Scale Real-World Critical Scene VideosDeepsNo ratings yet
- Loading Rate and Torsional Moments Predict Pilon FracturesDocument17 pagesLoading Rate and Torsional Moments Predict Pilon FracturesDeepsNo ratings yet
- Handbook of Lithium-Ion Battery Pack Design-Chemistry Components Types and TerminologyDocument8 pagesHandbook of Lithium-Ion Battery Pack Design-Chemistry Components Types and TerminologyDeeps100% (1)
- Chinese Finite Element Human Body Model Development Based On THUMS Occupant v402Document4 pagesChinese Finite Element Human Body Model Development Based On THUMS Occupant v402DeepsNo ratings yet
- Statistical Interpretation of Predictive Factors of Head Impact Kinematics in Traumatic Brain InjuryDocument4 pagesStatistical Interpretation of Predictive Factors of Head Impact Kinematics in Traumatic Brain InjuryDeepsNo ratings yet
- Trauma BiomechanicsDocument13 pagesTrauma BiomechanicsDeepsNo ratings yet
- Electronics For Beginners: A Practical Introduction To Schematics, Circuits, and MicrocontrollersDocument21 pagesElectronics For Beginners: A Practical Introduction To Schematics, Circuits, and MicrocontrollersDeepsNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Maintenance OF Micro Hydro: A Proposal ONDocument13 pagesMaintenance OF Micro Hydro: A Proposal ONNah Sr AdNo ratings yet
- VS - VPSP - DVL - DVSP - SSV - MSP - MVL Vertical Lift - Pre-Delivery and Frequent Inspection Report PDFDocument1 pageVS - VPSP - DVL - DVSP - SSV - MSP - MVL Vertical Lift - Pre-Delivery and Frequent Inspection Report PDFMaria Alejandra Peña LeonNo ratings yet
- Living in Belgrade Guide 2017Document83 pagesLiving in Belgrade Guide 2017Jamal KassisNo ratings yet
- En 14363 Trcece ProbeDocument114 pagesEn 14363 Trcece ProbeDragana TranavacNo ratings yet
- Ôn ThiDocument4 pagesÔn ThiKim Ánh ĐàoNo ratings yet
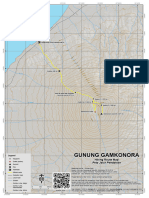
- Peta Jalur Pendakian Gunung GamkonoraDocument1 pagePeta Jalur Pendakian Gunung GamkonoraMuhammad Radima RahmadNo ratings yet
- Itinerary - 2023-09-03T153815.530Document1 pageItinerary - 2023-09-03T153815.530Sabah FouathiaNo ratings yet
- Philippine Jeepney Route NumbersDocument2 pagesPhilippine Jeepney Route NumbersHime “oujohime” Shiraishi100% (1)
- Stability Data BookletDocument18 pagesStability Data BookletPaul Ashton25% (4)
- P 10 eDocument1 pageP 10 eMuhdAisar96No ratings yet
- Anna Louise Strong - I Saw The New PolandDocument300 pagesAnna Louise Strong - I Saw The New PolandMocha SinghNo ratings yet
- R StudioDocument4 pagesR Studiosrishti bhatejaNo ratings yet
- Classification of Heat EnginesDocument20 pagesClassification of Heat EnginesParva ShrivastavaNo ratings yet
- Pallet Racking Pros ConsDocument28 pagesPallet Racking Pros ConsVuong LuuNo ratings yet
- Results Qualification iXS EDC #1 Losinj 2023Document6 pagesResults Qualification iXS EDC #1 Losinj 2023racementNo ratings yet
- HRV BrochureDocument20 pagesHRV BrochureAnonymous rSOjy9zPqrNo ratings yet
- AIAA EbooksDocument9 pagesAIAA Ebookssarah86304325No ratings yet
- Airport Operations and MarkingsDocument44 pagesAirport Operations and MarkingsDev Mohanty100% (2)
- Parking Management: Strategies, Evaluation and PlanningDocument31 pagesParking Management: Strategies, Evaluation and PlanningzaminrehNo ratings yet
- Fixed Speed / Constant Fill Fluid CouplingsDocument8 pagesFixed Speed / Constant Fill Fluid CouplingsAvinash GamitNo ratings yet
- BMW E32 - Dash Capacitor ReplacementDocument8 pagesBMW E32 - Dash Capacitor Replacementsamsularief03100% (1)
- (Darsenglizy.com موقع درس انجليزي) ليلة إمتحان العمالقة تالتة إعدادي 2023 مجابة ترم أولDocument25 pages(Darsenglizy.com موقع درس انجليزي) ليلة إمتحان العمالقة تالتة إعدادي 2023 مجابة ترم أولShaimaa HabibNo ratings yet
- Topic: Suspension System: Group 1 MembersDocument21 pagesTopic: Suspension System: Group 1 MembersMilcentNo ratings yet
- Miami Movie-The Specialist (1994)Document21 pagesMiami Movie-The Specialist (1994)Michael Cano LombardoNo ratings yet
- MV Wilhelm GustloffDocument2 pagesMV Wilhelm GustloffNadia AminNo ratings yet
- BS 2655-7 1970Document34 pagesBS 2655-7 1970AnoyNo ratings yet
- FS-6525MFP-6530MFP SM PDFDocument345 pagesFS-6525MFP-6530MFP SM PDFReneeNo ratings yet
- Pacific Islands Fuel Pricing - SPCDocument40 pagesPacific Islands Fuel Pricing - SPCHumphreyNo ratings yet
- TuytDocument117 pagesTuytJuan VarelaNo ratings yet
- Mikey Mails ItDocument7 pagesMikey Mails ItobielkoNo ratings yet