You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Vacancy Announcement (/2021 Advertisement) - Reannouncement!Document7 pagesVacancy Announcement (/2021 Advertisement) - Reannouncement!Htet Lynn HtunNo ratings yet
- Vacancy Announcement (61/2022 Advertisement)Document3 pagesVacancy Announcement (61/2022 Advertisement)Htet Lynn HtunNo ratings yet
- Medical Doctor: Première Urgence Internationale (PUI)Document3 pagesMedical Doctor: Première Urgence Internationale (PUI)Htet Lynn HtunNo ratings yet
- AVE HE Hildren International Vacancy Announcement: For Myanmar National OnlyDocument4 pagesAVE HE Hildren International Vacancy Announcement: For Myanmar National OnlyHtet Lynn HtunNo ratings yet
- MSI Reproductive Choices Medical Officer Social Media and Contact Center 9th May 2022Document2 pagesMSI Reproductive Choices Medical Officer Social Media and Contact Center 9th May 2022Htet Lynn HtunNo ratings yet
- Myanmar Red Cross Society: HR-Field VA No. 003.01 - Medical DoctorDocument6 pagesMyanmar Red Cross Society: HR-Field VA No. 003.01 - Medical DoctorHtet Lynn HtunNo ratings yet
- Program Coordinator HIVTB 0Document3 pagesProgram Coordinator HIVTB 0Htet Lynn HtunNo ratings yet
- Statistical Compilation of Annual Statement Information For Health Insurance Companies in 2018Document181 pagesStatistical Compilation of Annual Statement Information For Health Insurance Companies in 2018Htet Lynn HtunNo ratings yet
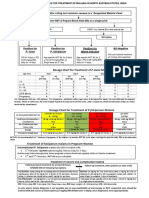
- Dosage Chart For Treatment of P.vivax MalariaDocument1 pageDosage Chart For Treatment of P.vivax MalariaHtet Lynn HtunNo ratings yet
- 2071 Solvency Margin Directive For Non Life Insurer 1Document9 pages2071 Solvency Margin Directive For Non Life Insurer 1Htet Lynn HtunNo ratings yet
- Myanmar Annual Country Report 2019Document52 pagesMyanmar Annual Country Report 2019Htet Lynn HtunNo ratings yet
- The Analytical Life Insurer: Profitable Analytic Strategies For Life and Annuity CarriersDocument12 pagesThe Analytical Life Insurer: Profitable Analytic Strategies For Life and Annuity CarriersHtet Lynn HtunNo ratings yet
- Med Stock 2.8.2021Document5 pagesMed Stock 2.8.2021Htet Lynn HtunNo ratings yet
- Use of Medical Big Data To Enhance Life Insurance Business: Takahide Shinge Yuji Kamata Takanobu Osaki Hirofumi KondoDocument6 pagesUse of Medical Big Data To Enhance Life Insurance Business: Takahide Shinge Yuji Kamata Takanobu Osaki Hirofumi KondoHtet Lynn HtunNo ratings yet
- 300 Years of Data AnalyticsDocument18 pages300 Years of Data AnalyticsHtet Lynn HtunNo ratings yet
- Research 2011 Medical MarkersDocument93 pagesResearch 2011 Medical MarkersHtet Lynn HtunNo ratings yet
- SwissRe Life Risk Selection 2011Document41 pagesSwissRe Life Risk Selection 2011Htet Lynn HtunNo ratings yet
- Research in Life InsuranceDocument6 pagesResearch in Life InsuranceHtet Lynn HtunNo ratings yet
- Asia-Pacific Disaster Report 2019 - Full Version PDFDocument130 pagesAsia-Pacific Disaster Report 2019 - Full Version PDFFrancesc CarbonellNo ratings yet
- Research and Development Activities of Life Insurance CompaniesDocument15 pagesResearch and Development Activities of Life Insurance CompaniesHtet Lynn HtunNo ratings yet
- Statistical Compilation of Annual Statement Information For Life & Health Insurance Companies in 2018Document216 pagesStatistical Compilation of Annual Statement Information For Life & Health Insurance Companies in 2018Htet Lynn HtunNo ratings yet
- Statistical Methods and Applications in Insurance and Finance - CIMPA School, Marrakech and El Kelaa M'gouna, Morocco, April 2013 (PDFDrive)Document228 pagesStatistical Methods and Applications in Insurance and Finance - CIMPA School, Marrakech and El Kelaa M'gouna, Morocco, April 2013 (PDFDrive)Htet Lynn HtunNo ratings yet
- Southeast Asia's Developing Life Insurance MarketsDocument3 pagesSoutheast Asia's Developing Life Insurance MarketsHtet Lynn HtunNo ratings yet
- Lic Edms RFPDocument124 pagesLic Edms RFPHtet Lynn HtunNo ratings yet
- Life Insurance Underwriting Guide (PDFDrive)Document84 pagesLife Insurance Underwriting Guide (PDFDrive)Htet Lynn HtunNo ratings yet
- Life Insurance Illustrations Practice Note Feb 2018Document113 pagesLife Insurance Illustrations Practice Note Feb 2018Htet Lynn HtunNo ratings yet
- Third Party Liability Law - PADocument4 pagesThird Party Liability Law - PAHtet Lynn HtunNo ratings yet
- Quick Survey - Data AnalysisDocument2 pagesQuick Survey - Data AnalysisHtet Lynn HtunNo ratings yet
- ISSA - Prevention of Occupational Risk in Health ServiceDocument21 pagesISSA - Prevention of Occupational Risk in Health ServiceHtet Lynn HtunNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- IO Cadet Survey and Best Practice Guide 2014Document42 pagesIO Cadet Survey and Best Practice Guide 2014alkazum100% (2)
- Boddy 2016Document8 pagesBoddy 2016EBO The InspirationistNo ratings yet
- 05 EJournal The Importance of Digital Marketing in PakistanDocument9 pages05 EJournal The Importance of Digital Marketing in PakistanM Fauzi SetiawanNo ratings yet
- 436 - 1 - 1 - Sampling of CoalDocument24 pages436 - 1 - 1 - Sampling of CoalSudhanshu DashNo ratings yet
- Om CH-4Document48 pagesOm CH-4Tesfaye KebedeNo ratings yet
- Worksheet: Qualitative vs. Quantitative Observations w8.SILN.1Document2 pagesWorksheet: Qualitative vs. Quantitative Observations w8.SILN.1Aisaka TaigaNo ratings yet
- (123doc) Common Difficulties in Translation From English To Vietnamese Encountered by The Fourthyear Students of English Faculty in Thuongmai UniversityDocument46 pages(123doc) Common Difficulties in Translation From English To Vietnamese Encountered by The Fourthyear Students of English Faculty in Thuongmai UniversityThu ThuỷNo ratings yet
- 4.designfor AASHTO 1997Document18 pages4.designfor AASHTO 1997Aku PalsuNo ratings yet
- Bsn/Nursing Research 2 (NCM 115) : Module # 2Document5 pagesBsn/Nursing Research 2 (NCM 115) : Module # 2Shane Frances SaborridoNo ratings yet
- Korean Film DomDocument6 pagesKorean Film DomRobert Frio86% (7)
- ISEB Paper QuestionsDocument9 pagesISEB Paper QuestionsPraveen KanwarNo ratings yet
- Different Methods, Approaches, Strategies of TeachingDocument35 pagesDifferent Methods, Approaches, Strategies of TeachingCary TolenadaNo ratings yet
- Gas Turbine ConsultancyDocument4 pagesGas Turbine ConsultancyAek JayNo ratings yet
- Unit 1: Introduction To Marketing Analytics: DR - Durga Wati Kushwaha Assistant ProfessorDocument33 pagesUnit 1: Introduction To Marketing Analytics: DR - Durga Wati Kushwaha Assistant ProfessorShivangi GuptaNo ratings yet
- Exploratory, Descriptive, and Causal Research DesignsDocument26 pagesExploratory, Descriptive, and Causal Research Designsvip9anasNo ratings yet
- Research MCQDocument24 pagesResearch MCQSaseela Balagobei100% (1)
- Cohesive Features in The Expository Writing of Undergraduates in Two Chinese UniversitiesDocument36 pagesCohesive Features in The Expository Writing of Undergraduates in Two Chinese UniversitiesMuftah HamedNo ratings yet
- Eda 223 Lesson 2 Introduction To Probability and StatisticsDocument27 pagesEda 223 Lesson 2 Introduction To Probability and StatisticsJustine IanNo ratings yet
- Development Methodology PDFDocument51 pagesDevelopment Methodology PDFKirushnarajNo ratings yet
- The Technology Acceptance Model: January 2008Document15 pagesThe Technology Acceptance Model: January 2008إمحمد السنوسي القزيريNo ratings yet
- A Systematic Guideline For Developing The Best Real-Time PCR PrimersDocument9 pagesA Systematic Guideline For Developing The Best Real-Time PCR PrimersSamNo ratings yet
- Independent Evaluation of FDA's First Cycle Review Performance - Retrospective Analysis Final ReportDocument37 pagesIndependent Evaluation of FDA's First Cycle Review Performance - Retrospective Analysis Final Reportrgodeshwer1No ratings yet
- Escalation - 05 ContentsDocument20 pagesEscalation - 05 ContentsSarinNo ratings yet
- BHPS Volume ADocument628 pagesBHPS Volume ADeboshree GhoshNo ratings yet
- Initializing The Need For Digital Leadership: A Meta-Analysis Review On Leadership Styles in Educational SectorDocument19 pagesInitializing The Need For Digital Leadership: A Meta-Analysis Review On Leadership Styles in Educational SectorsofyanNo ratings yet
- Moving Shots On A 3d Seismic SurveyDocument3 pagesMoving Shots On A 3d Seismic SurveyRodrigo Silva100% (1)
- Service Quality, Food Quality, Customer Satisfaction and RetentionDocument9 pagesService Quality, Food Quality, Customer Satisfaction and RetentionKashif IftikharNo ratings yet
- RM Notes (5modules)Document136 pagesRM Notes (5modules)rihan786mr7No ratings yet
- 4final REPORT - 1-62Document64 pages4final REPORT - 1-62Jyoti YadavNo ratings yet
- The Evolution of Complex NumberDocument13 pagesThe Evolution of Complex NumbersmeenaNo ratings yet