You might also like
- English10 Q2 Mod3 FormulatingAStatementofOpinionorAssertionDocument20 pagesEnglish10 Q2 Mod3 FormulatingAStatementofOpinionorAssertionmary anne wenceslaoNo ratings yet
- Tuberculosis and COVID-19 Interaction - A Review of BiolDocument15 pagesTuberculosis and COVID-19 Interaction - A Review of BiolMatvey SprindzukNo ratings yet
- DR Dina - TB & CovidDocument10 pagesDR Dina - TB & CovidDina FaizahNo ratings yet
- Immune InteractionDocument10 pagesImmune InteractionGaspar PonceNo ratings yet
- Sars-Cov-2, Bacterial Co-Infections, and Amr: The Deadly Trio in Covid-19?Document4 pagesSars-Cov-2, Bacterial Co-Infections, and Amr: The Deadly Trio in Covid-19?M ANo ratings yet
- Vaccine 2021Document17 pagesVaccine 2021cdsaludNo ratings yet
- COVID-19 and Tuberculosis: HighlightDocument7 pagesCOVID-19 and Tuberculosis: HighlightMariaNo ratings yet
- Type 1 Diabetes Triggered by Covid-19 Pandemic A Potential OutbreakDocument3 pagesType 1 Diabetes Triggered by Covid-19 Pandemic A Potential OutbreaksamuelNo ratings yet
- Viruses 13 00931 v2Document13 pagesViruses 13 00931 v2Kandy Caroline Woordt de PrincesNo ratings yet
- The Prevalence and Significance of The Pulmonary Bacterial Super-Infections Among Hospitalized COVID-19 Patients: A Scoping ReviewDocument7 pagesThe Prevalence and Significance of The Pulmonary Bacterial Super-Infections Among Hospitalized COVID-19 Patients: A Scoping Reviewد. مسلم الدخيليNo ratings yet
- HIV and COVID 19 Comorbidity Current EviDocument7 pagesHIV and COVID 19 Comorbidity Current EviM.ALDI RIZALDINo ratings yet
- Cellular and Molecular ImmunologyDocument21 pagesCellular and Molecular ImmunologyMUGDHA MITTALNo ratings yet
- Ageing Research ReviewsDocument11 pagesAgeing Research ReviewsLorena Morena Rosa MelchiorNo ratings yet
- 2019 Coronavirus Disease (COVID-19) Outbreak: A Review ArticleDocument6 pages2019 Coronavirus Disease (COVID-19) Outbreak: A Review ArticleMelakuNo ratings yet
- The Impact of COVID-19 On HIV Treatment and Research: A Call To ActionDocument14 pagesThe Impact of COVID-19 On HIV Treatment and Research: A Call To ActionAnastasia Yovita SariNo ratings yet
- TB in The Time of CovidDocument21 pagesTB in The Time of Coviddani catriaNo ratings yet
- Tuberculosis and COVID 19 in India: Challenges and OpportunitiesDocument3 pagesTuberculosis and COVID 19 in India: Challenges and OpportunitiesBram DaudNo ratings yet
- Pathogens 11 00445 v2Document14 pagesPathogens 11 00445 v2Jajang PortalNo ratings yet
- Pathogenesis of COVID-19-induced ARDS: Implications For An Ageing PopulationDocument12 pagesPathogenesis of COVID-19-induced ARDS: Implications For An Ageing PopulationJuliana SanjayaNo ratings yet
- En - 2308 0531 RFMH 22 03 650Document3 pagesEn - 2308 0531 RFMH 22 03 650jhonyNo ratings yet
- Human and Novel Coronavirus Infections in Children: A ReviewDocument21 pagesHuman and Novel Coronavirus Infections in Children: A ReviewWilmer UcedaNo ratings yet
- Jurnal 3Document8 pagesJurnal 3kalstarNo ratings yet
- Etiologi-Patofisioloy COVID-19Document12 pagesEtiologi-Patofisioloy COVID-19hening ciptiany pertiwyNo ratings yet
- The Novel Human Coronavirus Disease COVID DarulDocument9 pagesThe Novel Human Coronavirus Disease COVID Daruldarul qutniNo ratings yet
- The Microbial Coinfection in COVID-19Document9 pagesThe Microbial Coinfection in COVID-19liporagiNo ratings yet
- Review: Coronavirus Disease 2019 (COVID-19) : Latest Developments in Potential TreatmentsDocument14 pagesReview: Coronavirus Disease 2019 (COVID-19) : Latest Developments in Potential Treatmentsjenny12No ratings yet
- Clinical Outcomes in Patients Co-Infected With COVID-19 and Staphylococcus Aureus: A Scoping ReviewDocument17 pagesClinical Outcomes in Patients Co-Infected With COVID-19 and Staphylococcus Aureus: A Scoping ReviewLUIS MIGUEL CASTILLA MORANNo ratings yet
- Rheumatology: Implications of COVID 19 in Pediatric RheumatologyDocument21 pagesRheumatology: Implications of COVID 19 in Pediatric RheumatologyLaira VillalobosNo ratings yet
- Concepts in Disaster MedicineDocument8 pagesConcepts in Disaster MedicinedaniaNo ratings yet
- The Epidemiology and Pathogenesis of Coronavirus Disease Covid 19 Outbreak Hussin A Rothan Download 2024 Full ChapterDocument26 pagesThe Epidemiology and Pathogenesis of Coronavirus Disease Covid 19 Outbreak Hussin A Rothan Download 2024 Full Chapterbertha.harriman873100% (12)
- Embrazo en La ERA COVID 2020Document25 pagesEmbrazo en La ERA COVID 2020Juan Guillermo BuitragoNo ratings yet
- TB COVID Global Cohort ERJ 2022Document16 pagesTB COVID Global Cohort ERJ 2022The SangeNo ratings yet
- Velavan Et Al-2020-Tropical Medicine International HealthDocument4 pagesVelavan Et Al-2020-Tropical Medicine International Healthjunior rodriguesNo ratings yet
- COVID-19 and Diabetes Mellitus How One Pandemic Worsens The OtherDocument13 pagesCOVID-19 and Diabetes Mellitus How One Pandemic Worsens The OtherPatty MArivel ReinosoNo ratings yet
- The Pathophysiology of Virulence of The COVID-19 VirusDocument28 pagesThe Pathophysiology of Virulence of The COVID-19 VirusMohamed MounirNo ratings yet
- The Pathophysiology of Virulence of The COVID-19Document31 pagesThe Pathophysiology of Virulence of The COVID-19Glaneisia MitchellNo ratings yet
- "Health Is Not ValuedDocument134 pages"Health Is Not ValuedgeorgeNo ratings yet
- The Pathophysiology of Virulence of The COVID-19Document31 pagesThe Pathophysiology of Virulence of The COVID-19Vania ShaulaNo ratings yet
- COVID-19 and Dengue Fever: A Dangerous Combination For The Health System in BrazilDocument2 pagesCOVID-19 and Dengue Fever: A Dangerous Combination For The Health System in BrazilRaíssa Barbosa LuccheseNo ratings yet
- COVID-19 and Psoriasis Should We Fear For Patients Treated With BiologicsDocument4 pagesCOVID-19 and Psoriasis Should We Fear For Patients Treated With BiologicsEstu Paramadina PratamaNo ratings yet
- Mycobacteriumtuberculosis and Antibiotic ResistanceDocument19 pagesMycobacteriumtuberculosis and Antibiotic ResistanceinnocentNo ratings yet
- Covid 19 Diagnostio e TerapiaDocument15 pagesCovid 19 Diagnostio e TerapiaJess ElizeuNo ratings yet
- Covid NigeriaDocument5 pagesCovid NigeriaPriscy CandoNo ratings yet
- The Severity of The Co-Infection of Mycoplasma Pneumoniae in COVID-19 PatientsDocument7 pagesThe Severity of The Co-Infection of Mycoplasma Pneumoniae in COVID-19 Patientsemmanuel AndemNo ratings yet
- Koodak PDFDocument9 pagesKoodak PDFHugoMarcelo77No ratings yet
- Coronavirus Disease 2019 (COVID-19) Outcomes in HIV/AIDS Patients: A Systematic ReviewDocument11 pagesCoronavirus Disease 2019 (COVID-19) Outcomes in HIV/AIDS Patients: A Systematic ReviewherrerachaimNo ratings yet
- Jurnal 6Document2 pagesJurnal 6kalstarNo ratings yet
- Coronavirus Disease (Covid-19-Sars-Cov-2) and Nutrition: Is Infection in Italy Suggesting A Connection?Document6 pagesCoronavirus Disease (Covid-19-Sars-Cov-2) and Nutrition: Is Infection in Italy Suggesting A Connection?Ivan PitrulliNo ratings yet
- Maternal Physiological Changes in Pregnancyand Pathophysiology of COVID-19Document5 pagesMaternal Physiological Changes in Pregnancyand Pathophysiology of COVID-19Ario DaniantoNo ratings yet
- Tuberculosis Reactivation After Severe Sars-Cov-2 PneumoniaDocument2 pagesTuberculosis Reactivation After Severe Sars-Cov-2 PneumoniajohannaNo ratings yet
- Covid y AntropizaciónDocument5 pagesCovid y AntropizaciónjuanvillicanaNo ratings yet
- Jurnal InternasionalDocument8 pagesJurnal InternasionalPutriyani Ode aliNo ratings yet
- Pneumonia Caused by M. TBDocument8 pagesPneumonia Caused by M. TBerniherawatia658No ratings yet
- Significance TB and Covid 19Document4 pagesSignificance TB and Covid 19Yulia DevinaNo ratings yet
- Biomarkers of Ageing and Frailty May Predict COVID-19 SeverityDocument13 pagesBiomarkers of Ageing and Frailty May Predict COVID-19 SeverityPPDS Rehab Medik UnhasNo ratings yet
- Resolution of Coronavirus Disease 2019 COVID 19Document12 pagesResolution of Coronavirus Disease 2019 COVID 19Job GonzagaNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - UpToDateDocument43 pagesCoronavirus Disease 2019 (COVID-19) - UpToDateGloria MiramontesNo ratings yet
- COVID - Risk of Hospitaization IF-1.6Document20 pagesCOVID - Risk of Hospitaization IF-1.6Manal Haj HamadNo ratings yet
- 1 s2.0 S128645792030099X MainDocument7 pages1 s2.0 S128645792030099X MainNia KurniawanNo ratings yet
- Assessment of Drugs Administered in The Middle East As Part of The COVID 19 Management ProtocolsDocument20 pagesAssessment of Drugs Administered in The Middle East As Part of The COVID 19 Management ProtocolsHany ManikNo ratings yet
- Facing COVID-19 with the benefits of medical cannabisFrom EverandFacing COVID-19 with the benefits of medical cannabisNo ratings yet
- Covid Mental HealthDocument37 pagesCovid Mental HealthKalki DeephNo ratings yet
- Academic FreezeDocument2 pagesAcademic FreezeVincent Dominic BatoctoyNo ratings yet
- Crisis and Critique On Preparedness, Authoritarianism and The Regulatory StateDocument11 pagesCrisis and Critique On Preparedness, Authoritarianism and The Regulatory StateNikos KarfakisNo ratings yet
- Indrani GuptaDocument23 pagesIndrani GuptaPrerna singhNo ratings yet
- MessageDocument3 pagesMessagearaceliaguilar364No ratings yet
- Toberevised ThesisDocument34 pagesToberevised ThesisCharrie Faye Magbitang HernandezNo ratings yet
- Case Study - ZaloDocument18 pagesCase Study - ZaloTu TaNo ratings yet
- VNHSW Report-Health ProgramsDocument12 pagesVNHSW Report-Health Programsmaverick arquilloNo ratings yet
- Email:: Third Quarter Learner's Module 2 January 10-14, 2022Document8 pagesEmail:: Third Quarter Learner's Module 2 January 10-14, 2022Elia Saph MoonNo ratings yet
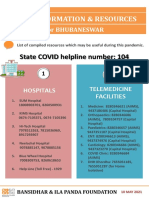
- State COVID Helpline Number: 104Document4 pagesState COVID Helpline Number: 104Yugant NayakNo ratings yet
- Does Playing Apart Really Bring Us Together - Preprint - v1Document18 pagesDoes Playing Apart Really Bring Us Together - Preprint - v1Mirian Josaro LlasaNo ratings yet
- My Memorable Vacation To India - Final DraftDocument1 pageMy Memorable Vacation To India - Final DraftSafwara SindhaNo ratings yet
- Rohilda MallariDocument2 pagesRohilda MallariAmy BCNo ratings yet
- Music Education and Distance Learning During COVID 19 A SurveyDocument11 pagesMusic Education and Distance Learning During COVID 19 A Surveycreyss0nNo ratings yet
- Sienna's Statement To The Toronto StarDocument2 pagesSienna's Statement To The Toronto StarToronto StarNo ratings yet
- RQS#Andrea Geni Entebang#19WVR12318Document103 pagesRQS#Andrea Geni Entebang#19WVR12318CAI YI LIMNo ratings yet
- Coronavirus & Force Majeure Bodhisattwa Majumder-1Document13 pagesCoronavirus & Force Majeure Bodhisattwa Majumder-1Abhi TripathiNo ratings yet
- Report Socio Economic Impacts of COVID 19 in COMESA FINAL EDIT 09.12.20Document106 pagesReport Socio Economic Impacts of COVID 19 in COMESA FINAL EDIT 09.12.20Sean GutsaNo ratings yet
- Acupuncture Effects On Covid 19 Long Hauler SyndromeDocument8 pagesAcupuncture Effects On Covid 19 Long Hauler SyndromeHerald Scholarly Open AccessNo ratings yet
- Kpj's Covid-19 BookletDocument62 pagesKpj's Covid-19 BookletKan Mi YiewNo ratings yet
- Mouhamadou Lamine Sarr CPC 1B MR Brunson Peace 2 Semester English TestDocument3 pagesMouhamadou Lamine Sarr CPC 1B MR Brunson Peace 2 Semester English TestLamine SarrNo ratings yet
- PLDT Inc - 17a 2019Document381 pagesPLDT Inc - 17a 2019Kylie Luigi Leynes BagonNo ratings yet
- Excess Deaths Inuk Research GateDocument31 pagesExcess Deaths Inuk Research Gatepetelechat222No ratings yet
- Sports NotesDocument1 pageSports NotessaniyaNo ratings yet
- Report On Consumer Preference On RTE Foods Post COVIDDocument16 pagesReport On Consumer Preference On RTE Foods Post COVIDMeenakshi SundaresanNo ratings yet
- 2022 First Edition MagazineDocument32 pages2022 First Edition Magazinequavioushuncho78No ratings yet
- Razmerita Et Al.Document819 pagesRazmerita Et Al.Nouman AamirNo ratings yet
- Self-Declaration / Undertaking by Students/Research Scholar/Project JRF Returning To IIT (ISM), DhanbadDocument2 pagesSelf-Declaration / Undertaking by Students/Research Scholar/Project JRF Returning To IIT (ISM), DhanbadSujoyDeNo ratings yet
- Thesis BurnoutDocument5 pagesThesis BurnoutLeslie Schulte100% (1)