You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Surgical Instruments, Types of Surgery and Surgical TechniquesDocument12 pagesSurgical Instruments, Types of Surgery and Surgical Techniquessheryl_morales100% (1)
- Unlock Your Hip Flexors Emails: Table of ContentDocument43 pagesUnlock Your Hip Flexors Emails: Table of ContentAmani Trang100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Consciousness in The Universe Is Scale Invariant and Implies An Event Horizon of The Human Brain PDFDocument39 pagesConsciousness in The Universe Is Scale Invariant and Implies An Event Horizon of The Human Brain PDFAdrián GonzálezNo ratings yet
- Pilates in The Second Trimester of PregnancyDocument18 pagesPilates in The Second Trimester of PregnancyAmani Trang100% (1)
- st60 Wind Manual PDFDocument52 pagesst60 Wind Manual PDFDave WinwoodNo ratings yet
- Track MaintenanceDocument18 pagesTrack MaintenanceMargaux MaipidNo ratings yet
- Nogva Marine Gearbox Ver.3.1Document30 pagesNogva Marine Gearbox Ver.3.1cezar frasao67% (3)
- CANbedded CANopen Availability enDocument4 pagesCANbedded CANopen Availability enAndres RiveraNo ratings yet
- CREII-Module-I - Lecture 4 PDFDocument34 pagesCREII-Module-I - Lecture 4 PDFshubhamNo ratings yet
- Strengthening The Central Nervous SystemDocument3 pagesStrengthening The Central Nervous SystemAmani Trang100% (1)
- All Chakra Set 1Document1 pageAll Chakra Set 1Amani TrangNo ratings yet
- Ijerph 18 02741 v2Document12 pagesIjerph 18 02741 v2Amani TrangNo ratings yet
- Advice and Exercise After ChildbirthDocument24 pagesAdvice and Exercise After ChildbirthAmani TrangNo ratings yet
- The JCD Fitness: Training ProgramDocument6 pagesThe JCD Fitness: Training ProgramAmani TrangNo ratings yet
- From Flat To All That Weeks 5 6Document7 pagesFrom Flat To All That Weeks 5 6Amani TrangNo ratings yet
- Teaching Concepts and Techniques of Yoga To Children: Yogacharya Dr. Ananda Balayogi BhavananiDocument8 pagesTeaching Concepts and Techniques of Yoga To Children: Yogacharya Dr. Ananda Balayogi BhavananiAmani TrangNo ratings yet
- QTY Protein Carbs Fats Calories Meal 1 (Blender)Document1 pageQTY Protein Carbs Fats Calories Meal 1 (Blender)Amani TrangNo ratings yet
- From Flat To All That - : Jamie Eason Middleton's Program 2015Document7 pagesFrom Flat To All That - : Jamie Eason Middleton's Program 2015Amani TrangNo ratings yet
- The Modern Natural Bodybuilder: Dietary Intake, Supplement Usage, Training Demands, and Their Health ImplicationsDocument333 pagesThe Modern Natural Bodybuilder: Dietary Intake, Supplement Usage, Training Demands, and Their Health ImplicationsAmani TrangNo ratings yet
- From Flat To All PDFDocument7 pagesFrom Flat To All PDFAmani TrangNo ratings yet
- From Flat To All That FitDocument6 pagesFrom Flat To All That FitAmani TrangNo ratings yet
- BA Bharathanatyam Latest Syllabus 2015 RegulationDocument18 pagesBA Bharathanatyam Latest Syllabus 2015 RegulationAmani TrangNo ratings yet
- REVISEDDance 2020-21Document26 pagesREVISEDDance 2020-21Amani TrangNo ratings yet
- IDIN-3 DTV3 Extra Grammar Exercises I PARTIALDocument4 pagesIDIN-3 DTV3 Extra Grammar Exercises I PARTIALrobert martinezNo ratings yet
- 8454 - Formulir Tanpa Judul (Respons)Document32 pages8454 - Formulir Tanpa Judul (Respons)Yelina KusumaNo ratings yet
- 50 Phrasal Verbs (Printing Version)Document3 pages50 Phrasal Verbs (Printing Version)Nagore MonteroNo ratings yet
- Sl. No. State/Union Territory: List of SecretariesDocument21 pagesSl. No. State/Union Territory: List of Secretariesrajaaero14350% (2)
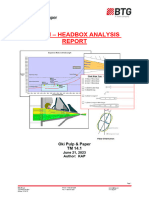
- OKI Tissue TM 14.1 Headbox Sheet Recommendations 6-21-23Document5 pagesOKI Tissue TM 14.1 Headbox Sheet Recommendations 6-21-23ismiasyofNo ratings yet
- Transportation and Highway Engineering PDFDocument3 pagesTransportation and Highway Engineering PDFReymark AbatayoNo ratings yet
- Annex 11 ITMSprinklersysteminspection 1649142576210Document6 pagesAnnex 11 ITMSprinklersysteminspection 1649142576210AmanNo ratings yet
- P&ID Development-StorageDocument7 pagesP&ID Development-StoragePrawira EffendiNo ratings yet
- Expected Credit Loss Analysis For Non Banking Financial Companies PDFDocument29 pagesExpected Credit Loss Analysis For Non Banking Financial Companies PDFAnandNo ratings yet
- Fernando Sorrentino StoriesDocument125 pagesFernando Sorrentino Storieswriterhari100% (3)
- Text1-Introduction To Cost Accounting-Student ResourceDocument22 pagesText1-Introduction To Cost Accounting-Student Resourcekinai williamNo ratings yet
- Footprint Expert Solder Joint Goal Tables: Updated: June 2020 © 2014 - 2021 - PCB Libraries, IncDocument35 pagesFootprint Expert Solder Joint Goal Tables: Updated: June 2020 © 2014 - 2021 - PCB Libraries, IncANANDNo ratings yet
- KBS Series Piezo BuzzersDocument1 pageKBS Series Piezo BuzzersBenjamín Varela UmbralNo ratings yet
- Ca-P IFU 897N203599A enDocument2 pagesCa-P IFU 897N203599A enenrique santillanNo ratings yet
- Autocollimator PDFDocument3 pagesAutocollimator PDFappannusaNo ratings yet
- Product Catalogue 01Document11 pagesProduct Catalogue 01Sanja TinaNo ratings yet
- PrednisoloneDocument4 pagesPrednisoloneUmemura-san SOkmo100% (1)
- Egaa/Bfs: 1.1. Atis 1.2. Noise Abatement Procedures 1. GeneralDocument24 pagesEgaa/Bfs: 1.1. Atis 1.2. Noise Abatement Procedures 1. GeneralTweed3ANo ratings yet
- E CA19-9ms en 20Document3 pagesE CA19-9ms en 20Hassan GillNo ratings yet
- Air Compressor Summary ListDocument4 pagesAir Compressor Summary ListAlvin Smith100% (1)
- For Your Local Distributor VisitDocument4 pagesFor Your Local Distributor VisitninaNo ratings yet
- Rock Drilling Methods 5Document16 pagesRock Drilling Methods 5Mbambiko NathanNo ratings yet
- بارجةDocument9 pagesبارجةMohamad Al khamisNo ratings yet