You might also like
- Anesthaesia and Intensive CareDocument139 pagesAnesthaesia and Intensive CareIvan Kurniadi100% (2)
- December2019 PCPMedicalDirectives4.6.1 PocketbookDocument166 pagesDecember2019 PCPMedicalDirectives4.6.1 PocketbookFirst LastNo ratings yet
- Cardiac Surgery Post-Op Care PDFDocument12 pagesCardiac Surgery Post-Op Care PDFHazel100% (1)
- DGL SBLC 110 World BanksDocument3 pagesDGL SBLC 110 World BanksJavier E. Hernández F.No ratings yet
- E-MDs Solution Series 7.2 Installation Guide R00 - 20110713Document68 pagesE-MDs Solution Series 7.2 Installation Guide R00 - 20110713itsokrelax100% (1)
- Date Account & Explanation F Debit CreditDocument7 pagesDate Account & Explanation F Debit CreditCindy Claire Pilapil88% (8)
- IEEE Hybrid GroundingDocument27 pagesIEEE Hybrid GroundingAlfredo Castillo BarettNo ratings yet
- COLLECTION OF BLOOD SPECIMENS MANUAL 2018-2020 - For Lab Guide PDFDocument27 pagesCOLLECTION OF BLOOD SPECIMENS MANUAL 2018-2020 - For Lab Guide PDFGonzalez ArturoNo ratings yet
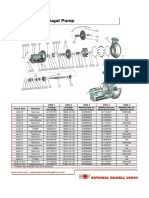
- Mission Magnum I Pump Spare PartsDocument2 pagesMission Magnum I Pump Spare PartsEleazar GallegosNo ratings yet
- 1) Cir v. Marubeni Corp-Duya (d2017)Document1 page1) Cir v. Marubeni Corp-Duya (d2017)joyceNo ratings yet
- The Crashing Ventilated Patient Ch.3 (Jairo I. Santanilla, ACEP, 2011) PDFDocument10 pagesThe Crashing Ventilated Patient Ch.3 (Jairo I. Santanilla, ACEP, 2011) PDFPkernNo ratings yet
- Anaesthesia & Intensive Care: For Fcai, Frca EdaicDocument139 pagesAnaesthesia & Intensive Care: For Fcai, Frca EdaicMuhammad Farid100% (2)
- Sedation Policy LPCH 6 11Document24 pagesSedation Policy LPCH 6 11Tribowo WicaksonoNo ratings yet
- Conscious Sedation StandardsDocument43 pagesConscious Sedation StandardsGhaleb Nasrallah95% (21)
- ACLS II Sept 25 StudentsDocument60 pagesACLS II Sept 25 StudentsLex CatNo ratings yet
- H940C PartsDocument388 pagesH940C PartsRildo ChavesNo ratings yet
- Infection Control in ICUDocument7 pagesInfection Control in ICUzenagit123456No ratings yet
- Shangai Houton ParkDocument15 pagesShangai Houton ParkHari HaranNo ratings yet
- Special Circumstances GuidelinesDocument19 pagesSpecial Circumstances GuidelinesRayNo ratings yet
- Blood Transfusion Guidelines PDFDocument21 pagesBlood Transfusion Guidelines PDFEmhemed Amer Tabib100% (2)
- Mechanical Ventilition COVID GuidelinesDocument7 pagesMechanical Ventilition COVID Guidelinesheba abuhelwaNo ratings yet
- CruiseShip Healthcare Guidelines 2011Document7 pagesCruiseShip Healthcare Guidelines 2011Kevin Lee Dupuy Jr.No ratings yet
- Basic Anesthetic Monitoring 2011Document3 pagesBasic Anesthetic Monitoring 2011egomezgrasNo ratings yet
- Monere in Anesthesia: Dr. Vinsensius ThomasDocument12 pagesMonere in Anesthesia: Dr. Vinsensius ThomasThomas KweeNo ratings yet
- Prone Position Guidelines-2Document14 pagesProne Position Guidelines-2SAMINo ratings yet
- $RFIIM3JDocument4 pages$RFIIM3JMichaelNo ratings yet
- Spirometry GuidelineDocument33 pagesSpirometry GuidelineSaraNo ratings yet
- Final Protocol Full and Final (72030)Document13 pagesFinal Protocol Full and Final (72030)Nido MalghaniNo ratings yet
- m52386 v1 Consedps21 2003Document7 pagesm52386 v1 Consedps21 2003Pepo BelovedNo ratings yet
- American Academy of Pediatrics: ABBREVIATION. PICU, Pediatric Intensive Care UnitDocument3 pagesAmerican Academy of Pediatrics: ABBREVIATION. PICU, Pediatric Intensive Care UnitdoctorsamitNo ratings yet
- StrokeDocument49 pagesStrokeChellamani UmakanthanNo ratings yet
- Guideline Admission To PICUDocument5 pagesGuideline Admission To PICUSony PrabowoNo ratings yet
- Guidelines On Management of Covid-19 Icu PatientDocument32 pagesGuidelines On Management of Covid-19 Icu PatientBrainy LumineusNo ratings yet
- SKILL STATION Management of Critically Ill Patient With Septic Shock Provider GuideDocument27 pagesSKILL STATION Management of Critically Ill Patient With Septic Shock Provider GuidesrinidhiNo ratings yet
- Anesthesia Secrets: Aspiration: Intern 張雅婷Document19 pagesAnesthesia Secrets: Aspiration: Intern 張雅婷張雅婷No ratings yet
- Local Anesthetic Systemic Toxicity (LAST)Document4 pagesLocal Anesthetic Systemic Toxicity (LAST)Abdelaziz ShokryNo ratings yet
- Guias ElsoDocument10 pagesGuias ElsoSebastián Caimanque CortésNo ratings yet
- 3.icu Admission CriteriaDocument7 pages3.icu Admission CriteriaPearlson JebamarshelNo ratings yet
- Guidelines Postresuscitation CareDocument39 pagesGuidelines Postresuscitation CareParvathy R NairNo ratings yet
- Special Circumstances Guidelines ALSDocument19 pagesSpecial Circumstances Guidelines ALSHamzaMasoodNo ratings yet
- 02-Incentive SpirometryDocument5 pages02-Incentive SpirometryPaloma CaneoNo ratings yet
- Code Blue Free For EveryoneDocument93 pagesCode Blue Free For EveryonedindaNo ratings yet
- Adult Client With Cardiovascular DisorderDocument14 pagesAdult Client With Cardiovascular Disordergraphicsbydi4mondNo ratings yet
- Emergency Neurological Life Support: Airway, Ventilation, and SedationDocument50 pagesEmergency Neurological Life Support: Airway, Ventilation, and SedationastrianamaulidianiNo ratings yet
- Chapter 4 - Postoperative CareDocument14 pagesChapter 4 - Postoperative Careandy liNo ratings yet
- 64 - MERS CoV P&PDocument24 pages64 - MERS CoV P&PerwindaNo ratings yet
- Critical Care Therapy and Respiratory Care Section: 1.0 DescriptionDocument7 pagesCritical Care Therapy and Respiratory Care Section: 1.0 DescriptionStefano Ignacio Valenzano FigueroaNo ratings yet
- TNSOP 6 Clinical GuidelinesDocument14 pagesTNSOP 6 Clinical Guidelinesazar103No ratings yet
- Acute Life-Threatening Hypoxemia During Mechanical VentilationDocument8 pagesAcute Life-Threatening Hypoxemia During Mechanical VentilationCesar Rivas CamposNo ratings yet
- 9a Nephrology PolicyDocument6 pages9a Nephrology PolicyRoslee SleeNo ratings yet
- Cobatrice - Syllabus 2021Document97 pagesCobatrice - Syllabus 2021Mohd Saif KhanNo ratings yet
- 2 Critical Care UnitDocument59 pages2 Critical Care UnitPALMA , JULIA A.No ratings yet
- ICU Criteria DuringDocument5 pagesICU Criteria DuringBaebee LouNo ratings yet
- Emergence and Postoperative Anesthetic Management: Prepared By: Serkalem Teshome Advised by Instructor WosneyelehDocument85 pagesEmergence and Postoperative Anesthetic Management: Prepared By: Serkalem Teshome Advised by Instructor WosneyelehagatakassaNo ratings yet
- Printed 9Document63 pagesPrinted 9Melodia Turqueza GandezaNo ratings yet
- Clinical Case Reports - 2021 - Sapkota - Fatal Anaphylaxis To Intravenous Ondansetron A Case ReportDocument3 pagesClinical Case Reports - 2021 - Sapkota - Fatal Anaphylaxis To Intravenous Ondansetron A Case Reportwilliam lozaNo ratings yet
- LiverpoolIntra-Hospital Transfer of ICU PatientsDocument8 pagesLiverpoolIntra-Hospital Transfer of ICU PatientsInnas DoankNo ratings yet
- Aldrette Score (Nitasha Best) (Discharge Criteria From Pacu)Document72 pagesAldrette Score (Nitasha Best) (Discharge Criteria From Pacu)Parvathy R NairNo ratings yet
- A3132020184314919 PDFDocument20 pagesA3132020184314919 PDFAnushka SoniNo ratings yet
- MOHFW Critical Care GuidelinesDocument123 pagesMOHFW Critical Care GuidelinesMOHAMMED IQBALNo ratings yet
- Adult Vital Sign ProtocolDocument10 pagesAdult Vital Sign ProtocolMegersa AleneNo ratings yet
- ESI ER CompleteDocument45 pagesESI ER Completetammy2121No ratings yet
- 7 Steps of Medical Direction 31Document22 pages7 Steps of Medical Direction 31jonathan layaNo ratings yet
- Transport: Administering Oxygen by Manual Resuscitation BAG Nursing Action RationaleDocument3 pagesTransport: Administering Oxygen by Manual Resuscitation BAG Nursing Action RationaleIan TuNo ratings yet
- Rims Covid TRTMNT Protocol 1Document30 pagesRims Covid TRTMNT Protocol 1Sooraj ThomasNo ratings yet
- Cruise Ship Health Care Guidelines PrepDocument8 pagesCruise Ship Health Care Guidelines PrepMaxMusterNo ratings yet
- Standards For Basic Anesthetic MonitoringDocument3 pagesStandards For Basic Anesthetic MonitoringMuhammad AsyrafNo ratings yet
- Edcba: Economic Decision and Cost Benefit AnalysisDocument4 pagesEdcba: Economic Decision and Cost Benefit AnalysisJOSE LUISNo ratings yet
- Case Method 1Document8 pagesCase Method 1Abcid BlancaNo ratings yet
- OHAS Midterm Quiz 1 - Attempt ReviewDocument7 pagesOHAS Midterm Quiz 1 - Attempt ReviewNot Racist By The WayNo ratings yet
- Motion in A Straight Line PDFDocument26 pagesMotion in A Straight Line PDFsujit21in4376100% (1)
- Insurance Regulatory and Development ActDocument13 pagesInsurance Regulatory and Development ActSai VasudevanNo ratings yet
- Accounting Practice Set (Journal Ledger Trial Balance)Document13 pagesAccounting Practice Set (Journal Ledger Trial Balance)Yasmien Mae ValdesconaNo ratings yet
- Specifying Generator TestingDocument4 pagesSpecifying Generator TestingAmit BiswasNo ratings yet
- Entrepreneurship SchemesDocument6 pagesEntrepreneurship SchemesSADENT2100% (1)
- Assignment - 1: Chapter - 2 Probability Concepts and Applications WTVX Case StudyDocument9 pagesAssignment - 1: Chapter - 2 Probability Concepts and Applications WTVX Case StudySiddhant SinghNo ratings yet
- Effect of Social MediaDocument14 pagesEffect of Social MediaChaitanya PurohitNo ratings yet
- Hotel. How May I Help You?Document2 pagesHotel. How May I Help You?putu kasparinataNo ratings yet
- Demand PlaningDocument48 pagesDemand PlaningdaliyaNo ratings yet
- Byron v. Boone and Audray S. Boone v. United States, 470 F.2d 232, 10th Cir. (1972)Document8 pagesByron v. Boone and Audray S. Boone v. United States, 470 F.2d 232, 10th Cir. (1972)Scribd Government DocsNo ratings yet
- Custom Car Care: Case Analysis OnDocument4 pagesCustom Car Care: Case Analysis OnSatyabrataNayakNo ratings yet
- Magnetorheological Finishing - A ReviewDocument7 pagesMagnetorheological Finishing - A ReviewAnonymous yorzHjDBdNo ratings yet
- (Term Paper) The Rationale of Shari'ah Supporting Contracts - A Case of MPODocument22 pages(Term Paper) The Rationale of Shari'ah Supporting Contracts - A Case of MPOHaziyah HalimNo ratings yet
- Mico Paulo S. Caballero - Let Us Practice MoreDocument3 pagesMico Paulo S. Caballero - Let Us Practice MoreMico Paulo CaballeroNo ratings yet
- Filipino Value SystemDocument2 pagesFilipino Value SystemJayvee Amoy AmolatoNo ratings yet
- mt4 GuideDocument24 pagesmt4 GuideGeorge PruteanuNo ratings yet
- PDFDocument6 pagesPDFRuel GonzalesNo ratings yet
- Motion For Issuance of Certificate of FinalityDocument3 pagesMotion For Issuance of Certificate of Finalitymarvilie sernaNo ratings yet
- Cyber Defense MatrixDocument141 pagesCyber Defense MatrixDiego MagoNo ratings yet