You might also like
- Practical Handbook of Pharmaceutical Chemistry for M.PharmFrom EverandPractical Handbook of Pharmaceutical Chemistry for M.PharmNo ratings yet
- 1 s2.0 S0165022X05001119 MainDocument14 pages1 s2.0 S0165022X05001119 MainBivin EbenezerNo ratings yet
- Determine of Morphine and Codeine in Human Urine by Gas Chromatography-Mass SpectrometryDocument7 pagesDetermine of Morphine and Codeine in Human Urine by Gas Chromatography-Mass Spectrometryamaliahriskaika100% (1)
- Analytical Method Development and Validation of Teneligliptin by Using RP HPLC With ICH GuidelinesDocument5 pagesAnalytical Method Development and Validation of Teneligliptin by Using RP HPLC With ICH GuidelinesEditor IJTSRDNo ratings yet
- A Validated RP-HPLC Method For The Determination of Celecoxib in Bulk and Pharmaceutical Dosage FormDocument5 pagesA Validated RP-HPLC Method For The Determination of Celecoxib in Bulk and Pharmaceutical Dosage FormOskar LazaroNo ratings yet
- CitrizineDocument5 pagesCitrizineAbdu K. ÊlmankoryNo ratings yet
- Mitijps PaperDocument7 pagesMitijps PaperBrijeshkunvar MishraNo ratings yet
- 20211226124933a5 64 JCM 2108 2174Document11 pages20211226124933a5 64 JCM 2108 2174Venkat PalaganiNo ratings yet
- Development and Validation of Bioanalytical Methods For Quantitative Analysis of Gefitinib by Using Uv-Visible SpectrophotometryDocument13 pagesDevelopment and Validation of Bioanalytical Methods For Quantitative Analysis of Gefitinib by Using Uv-Visible SpectrophotometryPamarthi TejaswiNo ratings yet
- Creatinina em urinaDocument6 pagesCreatinina em urinaThiago VillaNo ratings yet
- Methadone Extraction Using Solid Phase Extraction From Urine and Quantification by Gas Chromatography-Mass SpectrometryDocument13 pagesMethadone Extraction Using Solid Phase Extraction From Urine and Quantification by Gas Chromatography-Mass SpectrometryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Preparation of A Naltrexone HCL Potentiometric Sensor and 1 PDFDocument7 pagesPreparation of A Naltrexone HCL Potentiometric Sensor and 1 PDFNilaNo ratings yet
- Estimation of Meropenem in Human Plasma by HPLC-UV and Its Application in Comparative Bioavailability StudyDocument8 pagesEstimation of Meropenem in Human Plasma by HPLC-UV and Its Application in Comparative Bioavailability Studyayand2005No ratings yet
- HPLC METHOD VALIDATIONDocument5 pagesHPLC METHOD VALIDATIONbavirisettikiranNo ratings yet
- A Comparative Study For The Quantitative Determination of Paracetamol in Tablets Using UVDocument7 pagesA Comparative Study For The Quantitative Determination of Paracetamol in Tablets Using UVRizqita Atikah SNo ratings yet
- Thermo - Drug Abuse in UrineDocument7 pagesThermo - Drug Abuse in UrineYoosu NguyenNo ratings yet
- Lorno HPLCDocument5 pagesLorno HPLCmostafaNo ratings yet
- ToxigcmsDocument37 pagesToxigcmsTadesse TakeleNo ratings yet
- Met AnaDocument17 pagesMet AnaMadhuri YakkalaNo ratings yet
- Toxilab TubeDocument8 pagesToxilab TubeDrMd IdrisNo ratings yet
- RCM 2100Document6 pagesRCM 2100Annia KurniawatiNo ratings yet
- J Clin Pathol 1988 Crocker 576 81Document7 pagesJ Clin Pathol 1988 Crocker 576 81Ryan SadonoNo ratings yet
- IJRPBSDocument8 pagesIJRPBSrakesh2284No ratings yet
- Simultaneous Determination of Cefotaxime Sodium and Paracetamol by LC-MSDocument7 pagesSimultaneous Determination of Cefotaxime Sodium and Paracetamol by LC-MSIOSR Journal of PharmacyNo ratings yet
- Validation Sop GCMSDocument12 pagesValidation Sop GCMSMai PhuNo ratings yet
- A New RP-HPLC Method For Analysis of Mebeverine Hydrochloride in Raw Materials and TabletsDocument4 pagesA New RP-HPLC Method For Analysis of Mebeverine Hydrochloride in Raw Materials and TabletsEkaSelvinaNo ratings yet
- Determination of Morphine in Human Urine by A Simple Reverse Phase High-Performance Liquid Chromatography Method With UV DetectionDocument5 pagesDetermination of Morphine in Human Urine by A Simple Reverse Phase High-Performance Liquid Chromatography Method With UV DetectionAdi SubagioNo ratings yet
- 17 Ac19Document9 pages17 Ac19Dana StoinNo ratings yet
- Paper Cyproheptadine PDFDocument8 pagesPaper Cyproheptadine PDFMauro SucupiraNo ratings yet
- Cyanide Spectroquant 114561 WW Method 1999 PDFDocument20 pagesCyanide Spectroquant 114561 WW Method 1999 PDFSantos Edwin Cari ApazaNo ratings yet
- CelicoxibDocument8 pagesCelicoxibDavid Raju GollapudiNo ratings yet
- Development and Validation of A LC/MS/MS Method For The Determination of Duloxetine in Human Plasma and Its Application To Pharmacokinetic StudyDocument14 pagesDevelopment and Validation of A LC/MS/MS Method For The Determination of Duloxetine in Human Plasma and Its Application To Pharmacokinetic StudyMohamed Medhat AliNo ratings yet
- UV method for metformin quantification in tabletsDocument4 pagesUV method for metformin quantification in tabletsWilliam SmithNo ratings yet
- Arnhard 2012Document14 pagesArnhard 2012malwanafhc.adNo ratings yet
- Art 04Document6 pagesArt 04sportcar2000No ratings yet
- Jurnal HPLCDocument3 pagesJurnal HPLCRiche Dewata S.No ratings yet
- 153 FullDocument7 pages153 FullMaulinaNo ratings yet
- Jurnal HPLC KromatografiDocument8 pagesJurnal HPLC KromatografiDevi AtikahNo ratings yet
- Development and Validation of HPLC Method For The Estimation of Lapatinib in Bulk Drugs and Pharmaceutical FormulationsDocument8 pagesDevelopment and Validation of HPLC Method For The Estimation of Lapatinib in Bulk Drugs and Pharmaceutical FormulationspalkybdNo ratings yet
- 10.1515 - Revac 2022 0039Document12 pages10.1515 - Revac 2022 0039yordanosezerihun07No ratings yet
- A Very Sensitive Bioanalytical Method For The Estimation of Escitalopram in Rat Plasma Using Liquid Chromatography WithDocument10 pagesA Very Sensitive Bioanalytical Method For The Estimation of Escitalopram in Rat Plasma Using Liquid Chromatography WithvinayNo ratings yet
- C995 03 PDFDocument12 pagesC995 03 PDFdanzan1No ratings yet
- A Novel Sample Preparation For Shotgun Proteomics Characterization of HCPs in AntibodiesDocument9 pagesA Novel Sample Preparation For Shotgun Proteomics Characterization of HCPs in AntibodiesTaylor SimmonnsNo ratings yet
- Glucose KitDocument2 pagesGlucose KitJuan Enrique Ramón OrellanaNo ratings yet
- Quantitative Analysis and Purity Evaluation of Medroxyprogesterone Acetate by HPLCDocument12 pagesQuantitative Analysis and Purity Evaluation of Medroxyprogesterone Acetate by HPLCLeonardo GiraldoNo ratings yet
- Pre-Column Derivatization Method For DeterminingDocument7 pagesPre-Column Derivatization Method For DeterminingKuanNo ratings yet
- DiacereinDocument6 pagesDiacereinRikin ShahNo ratings yet
- Assignment GCMSDocument6 pagesAssignment GCMSdean016026No ratings yet
- Validated HPLC Method for Quetiapine ImpuritiesDocument9 pagesValidated HPLC Method for Quetiapine ImpuritiesVinaya SnehalathaNo ratings yet
- Ashraf M. Mahmoud, Saad A. Alqahtani: American Journal of Analytical Chemistry, 2016, 7, 179-191Document13 pagesAshraf M. Mahmoud, Saad A. Alqahtani: American Journal of Analytical Chemistry, 2016, 7, 179-191DrGajanan VaishnavNo ratings yet
- Journal of Chemical and Pharmaceutical Research, 2013, 5 (5) :1-11Document11 pagesJournal of Chemical and Pharmaceutical Research, 2013, 5 (5) :1-11NurulnameiiNo ratings yet
- Suspected Pediatric IngestionsDocument5 pagesSuspected Pediatric IngestionsJenness VillanuevaNo ratings yet
- Dextromethorphan + QuinidineDocument11 pagesDextromethorphan + QuinidineDavid Raju GollapudiNo ratings yet
- HPLC Method for Zinc Carnosine AnalysisDocument5 pagesHPLC Method for Zinc Carnosine AnalysisSouheila MniNo ratings yet
- New Spectrophotometric Assay of Pyrantel Pamoate in Pharmaceuticals and Spiked Human Urine Using Three Complexing AgentsDocument2 pagesNew Spectrophotometric Assay of Pyrantel Pamoate in Pharmaceuticals and Spiked Human Urine Using Three Complexing AgentsNurul FatimahNo ratings yet
- Cao2008 Article AMethodForQuantifyingTheUnstabDocument9 pagesCao2008 Article AMethodForQuantifyingTheUnstabUsman ArshadNo ratings yet
- Online Extraction LC-MSMS Method For The Simultaneous Quantitative...Document11 pagesOnline Extraction LC-MSMS Method For The Simultaneous Quantitative...qketzalNo ratings yet
- Sian Ournal of HemistryDocument5 pagesSian Ournal of Hemistryjkc collegeNo ratings yet
- A Laboratory Manual of Physical PharmaceuticsFrom EverandA Laboratory Manual of Physical PharmaceuticsRating: 2.5 out of 5 stars2.5/5 (2)
- Drugs & Pharma Tech HandbookDocument13 pagesDrugs & Pharma Tech Handbookإلياس صادقNo ratings yet
- An Analysis of The Wood Sugar Assay Using HPLC PDFDocument7 pagesAn Analysis of The Wood Sugar Assay Using HPLC PDFBelete BayeNo ratings yet
- Ally TestDocument17 pagesAlly TestAhmed MasoudNo ratings yet
- Acebutolol HydrochlorideDocument2 pagesAcebutolol HydrochlorideMaximiliano OjedaNo ratings yet
- Definition and terms of chromatography techniqueDocument4 pagesDefinition and terms of chromatography techniqueHarshit KumarNo ratings yet
- Extraction and Separation of Plant PigmentsDocument4 pagesExtraction and Separation of Plant PigmentsJade EncarnacionNo ratings yet
- Microfluidic Paper Device Detects Salivary AldehydesDocument4 pagesMicrofluidic Paper Device Detects Salivary AldehydesVeena mitraNo ratings yet
- BMW 162Document7 pagesBMW 162Ridho2 AfriyanNo ratings yet
- HILIC Practical GuideDocument30 pagesHILIC Practical GuidepatrickjanssenNo ratings yet
- Ast D-6953Document6 pagesAst D-6953jesrcontreras1976100% (1)
- Myoglobin Extraction in BiochemistryDocument1 pageMyoglobin Extraction in BiochemistrySteven Obrien100% (1)
- Uv Analysis Method Development For Diclofenac and Paracetamol in CombinationDocument28 pagesUv Analysis Method Development For Diclofenac and Paracetamol in Combination0921py100% (5)
- Ionpac Cs5A Column & Metpac Reagents: Rapid, Routine Analysis of Transition Metals in Diverse SamplesDocument6 pagesIonpac Cs5A Column & Metpac Reagents: Rapid, Routine Analysis of Transition Metals in Diverse Samplescecilia elizabeth quiroga talledoNo ratings yet
- Analysis Results Report E MDocument3 pagesAnalysis Results Report E MViorel PopNo ratings yet
- NernstDocument3 pagesNernstAdeliza Mortalla100% (2)
- Trace Chloride, Fluoride, and Bromide in Liquid Organics by Combustion Ion Chromatography (CIC)Document14 pagesTrace Chloride, Fluoride, and Bromide in Liquid Organics by Combustion Ion Chromatography (CIC)ZhaoYun1314No ratings yet
- Chemical Weapons Convention Chemicals Analysis - 2005 - Mesilaakso - The OPCW Gas Chromatograph Mass Spectrometer ForDocument14 pagesChemical Weapons Convention Chemicals Analysis - 2005 - Mesilaakso - The OPCW Gas Chromatograph Mass Spectrometer ForWacel HamaniNo ratings yet
- Key Differences Between GC/MS and LC/MSDocument3 pagesKey Differences Between GC/MS and LC/MSForid AhammadNo ratings yet
- HPLC Analysis of Nicotinamide Pyridoxine Riboflavi PDFDocument9 pagesHPLC Analysis of Nicotinamide Pyridoxine Riboflavi PDFcitrahdynNo ratings yet
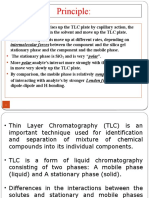
- Principle:: Intermolecular Forces Between The Component and The Silica GelDocument32 pagesPrinciple:: Intermolecular Forces Between The Component and The Silica GelKrishnan GiribabuNo ratings yet
- Spoilage On Canned Foods BAMDocument28 pagesSpoilage On Canned Foods BAMGuillermo BarriosNo ratings yet
- Quality Control ChemDocument21 pagesQuality Control ChemAli Rizvi100% (1)
- Ginger PresentationDocument22 pagesGinger PresentationFirzawati HamadahNo ratings yet
- IEXDocument11 pagesIEXRizky RamadhaniNo ratings yet
- Analytica Chimica Acta: Ahmed Abdulrahman, Ashraf GhanemDocument17 pagesAnalytica Chimica Acta: Ahmed Abdulrahman, Ashraf GhanemRosyida AdiniaNo ratings yet
- EBTaboada Hybridigm Presentation v070617Document37 pagesEBTaboada Hybridigm Presentation v070617Ari HalosNo ratings yet
- Oleo Essencial e Chenopodium Ambroioides L, Atividade Anticoxidantes e AntibacterianaDocument9 pagesOleo Essencial e Chenopodium Ambroioides L, Atividade Anticoxidantes e AntibacterianaLéya MateusNo ratings yet
- CitralDocument11 pagesCitralLithin LekkalaNo ratings yet
- Analyze Ink Using Paper ChromatographyDocument4 pagesAnalyze Ink Using Paper ChromatographyJohn Jill T. VillamorNo ratings yet
- Spectrophotochemical and Chroma Analysis .PPDocument55 pagesSpectrophotochemical and Chroma Analysis .PPKhyra JuliaNo ratings yet