You might also like
- Search Engine Marketing Course Material 2t4d9Document165 pagesSearch Engine Marketing Course Material 2t4d9Yoga Guru100% (2)
- Construction Materials and Testing: "WOOD"Document31 pagesConstruction Materials and Testing: "WOOD"Aira Joy AnyayahanNo ratings yet
- The Evolution of Airway Management - New Concepts and Conflicts With Traditional PracticeDocument13 pagesThe Evolution of Airway Management - New Concepts and Conflicts With Traditional Practicecaca100% (1)
- Areas of Research Interest in Airway Management: Direction and GapsDocument3 pagesAreas of Research Interest in Airway Management: Direction and GapsLaras Bani WasesoNo ratings yet
- Videolaryngoscopy Increases Mouth-To-Mouth' Distance Compared With Direct LaryngosDocument2 pagesVideolaryngoscopy Increases Mouth-To-Mouth' Distance Compared With Direct LaryngosHugo Robles GómezNo ratings yet
- Nej MR A 1916801Document12 pagesNej MR A 1916801bagholderNo ratings yet
- Manejo de La Via Aerea Dificil 2021nejmDocument12 pagesManejo de La Via Aerea Dificil 2021nejmMartha Isabel BurgosNo ratings yet
- Training in Uniportal VATS LobectomyDocument7 pagesTraining in Uniportal VATS LobectomyAlin Ionut BurlacuNo ratings yet
- Controversiesin Microvascular Maxillofacial Reconstruction: Adam P. Fagin,, Daniel PetrisorDocument10 pagesControversiesin Microvascular Maxillofacial Reconstruction: Adam P. Fagin,, Daniel PetrisorSheetal HNo ratings yet
- Cannot Intubate, Cannot Oxygenate" (CICO) Rescue by Emergency Front of Neck Airway (eFONA)Document9 pagesCannot Intubate, Cannot Oxygenate" (CICO) Rescue by Emergency Front of Neck Airway (eFONA)Jorge QuilumbaNo ratings yet
- The Evolution of Airway Management - New Concepts and Conflicts With Traditional PracticeDocument13 pagesThe Evolution of Airway Management - New Concepts and Conflicts With Traditional PracticeKartika RahmawatiNo ratings yet
- Airway Technique Strengths and LimitationsDocument15 pagesAirway Technique Strengths and LimitationsJEFFERSON MUÑOZNo ratings yet
- TMP 99 BADocument6 pagesTMP 99 BAFrontiersNo ratings yet
- The Lost Airway Potnuru2020Document14 pagesThe Lost Airway Potnuru2020Felipe CarmonaNo ratings yet
- Dispositivos - Supragloticos LECTURADocument13 pagesDispositivos - Supragloticos LECTURAAinhoa Jimenez TraperoNo ratings yet
- Hagberg 2015Document3 pagesHagberg 2015fadhila_nurrahmaNo ratings yet
- Preventing Laparoscopic InjuryDocument10 pagesPreventing Laparoscopic InjuryMaestro JadNo ratings yet
- Airway Management Guideline and Device UpdatesDocument17 pagesAirway Management Guideline and Device UpdatesaprinaNo ratings yet
- Supraglottic Airway DevicesDocument20 pagesSupraglottic Airway DevicesZac CamannNo ratings yet
- 405 2020 Article 6196Document8 pages405 2020 Article 6196Nabil Last FriendNo ratings yet
- Articulo en InglesDocument20 pagesArticulo en InglesJavier VivarNo ratings yet
- A Review of Natural Orifice Translumenal Endoscopic Surgery (NOTES) For Intra-Abdominal SurgeryDocument20 pagesA Review of Natural Orifice Translumenal Endoscopic Surgery (NOTES) For Intra-Abdominal SurgerylifeofnameNo ratings yet
- PIIS000709122030458XDocument4 pagesPIIS000709122030458Xmarco enriquezNo ratings yet
- Anaesthesia - September 1992 - Mason - Learning Fibreoptic Intubation Fundamental ProblemsDocument3 pagesAnaesthesia - September 1992 - Mason - Learning Fibreoptic Intubation Fundamental ProblemsfoolscribdNo ratings yet
- 538-Article Text-7432-1-10-20200805Document8 pages538-Article Text-7432-1-10-20200805Ankita GuravNo ratings yet
- Tracheostomy Management During The COVID-19 PandemicDocument3 pagesTracheostomy Management During The COVID-19 Pandemicika lestariNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument16 pagesBest Practice & Research Clinical Obstetrics and GynaecologyMaría PradoNo ratings yet
- Prediction of Difficult Mask Ventilation: Clinical InvestigationsDocument8 pagesPrediction of Difficult Mask Ventilation: Clinical InvestigationsdiandianNo ratings yet
- Safe Surgery 2Document5 pagesSafe Surgery 2Masrun FatanahNo ratings yet
- VideolaringosDocument9 pagesVideolaringosmaomed2014No ratings yet
- Five Years Experience of Tracheostomy at A Tertiary Level Hospital (Dhaka Medical College Hospital) in Bangladesh Review of 257 CasesDocument8 pagesFive Years Experience of Tracheostomy at A Tertiary Level Hospital (Dhaka Medical College Hospital) in Bangladesh Review of 257 CasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- AO CMFS During COVID-19Document6 pagesAO CMFS During COVID-19โสภาพรรณวดี รวีวารNo ratings yet
- Techniques of Surgical TracheostomyDocument10 pagesTechniques of Surgical TracheostomyMhd Al Fazri BroehNo ratings yet
- Jurnal Suction English PDFDocument4 pagesJurnal Suction English PDFJoko SuprionoNo ratings yet
- Outcome and Complication of Paediatric Dacryocystorhinostomy at Mardan Medical Complex Ophthalmology UnitDocument3 pagesOutcome and Complication of Paediatric Dacryocystorhinostomy at Mardan Medical Complex Ophthalmology UnitInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Aesculap Ds Appendectomy ClipDocument12 pagesAesculap Ds Appendectomy ClipdoniNo ratings yet
- Surgical Management of Turbinoplasty LO MEJOR DE LO MEJORDocument10 pagesSurgical Management of Turbinoplasty LO MEJOR DE LO MEJORDavid CáceresNo ratings yet
- Theatre VentilationDocument4 pagesTheatre VentilationKanokwan BorwornphiphattanachaiNo ratings yet
- Summary of Anesthesia Consultant - André FerreiraDocument1 pageSummary of Anesthesia Consultant - André FerreiracedivadeniaNo ratings yet
- Jurnal Close Suction EvalDocument8 pagesJurnal Close Suction EvalFatimah ZahraNo ratings yet
- 01 Office-Based LaryngealDocument10 pages01 Office-Based LaryngealG WNo ratings yet
- Supraglottic Airway Devices_ Present State and __Outlook for 2050Document13 pagesSupraglottic Airway Devices_ Present State and __Outlook for 2050drisaacvelazquezNo ratings yet
- Oral Oncology: CORONA-steps For Tracheotomy in COVID-19 Patients: A Staff-Safe Method For Airway ManagementDocument3 pagesOral Oncology: CORONA-steps For Tracheotomy in COVID-19 Patients: A Staff-Safe Method For Airway ManagementCorin Boice TelloNo ratings yet
- Management of Maxillofacial Trauma in EmergencyDocument11 pagesManagement of Maxillofacial Trauma in EmergencyDicky Nanda KhaNo ratings yet
- Core Clinical Content For Postgraduate Anaesthetic Training and Continuing Professional DevelopmentDocument50 pagesCore Clinical Content For Postgraduate Anaesthetic Training and Continuing Professional DevelopmentAbeNo ratings yet
- Airway management in practiotioner in Trauma patientsDocument3 pagesAirway management in practiotioner in Trauma patientsjrnavarrovNo ratings yet
- Maggiore 2013Document10 pagesMaggiore 2013oman hendiNo ratings yet
- Advances in Anesthesia: The Role of Videolaryngoscopy in Airway ManagementDocument12 pagesAdvances in Anesthesia: The Role of Videolaryngoscopy in Airway ManagementAgung HidayaniNo ratings yet
- Pediatric Anesthesia - 2007 - CATCHPOLE - Patient Handover From Surgery To Intensive Care Using Formula 1 Pit Stop andDocument9 pagesPediatric Anesthesia - 2007 - CATCHPOLE - Patient Handover From Surgery To Intensive Care Using Formula 1 Pit Stop andkowaopfdlfzfwnispxNo ratings yet
- Comparison of A Supraglottic Gel Device and An Endotracheal Tube in Keratoplasty Performed Under General Anesthesia: A Randomized Clinical TrialDocument4 pagesComparison of A Supraglottic Gel Device and An Endotracheal Tube in Keratoplasty Performed Under General Anesthesia: A Randomized Clinical TrialJoseph Chipana GutierrezNo ratings yet
- Complications and Failure of Airway ManagementDocument18 pagesComplications and Failure of Airway ManagementNirma RahayuNo ratings yet
- Keratoconus 2Document39 pagesKeratoconus 2YOSEF DERDESAWENo ratings yet
- tang-et-al-2022-pilot-single-arm-study-to-inveDocument12 pagestang-et-al-2022-pilot-single-arm-study-to-inveLinhNo ratings yet
- AnestesiologiaDocument9 pagesAnestesiologiaMarjorie SimbañaNo ratings yet
- Safety Bulletin - Issue 8 - July 2023Document2 pagesSafety Bulletin - Issue 8 - July 2023MubeenRahmanNo ratings yet
- 1 s2.0 S1479666X20301888 MainDocument5 pages1 s2.0 S1479666X20301888 MainTécnicos CredineNo ratings yet
- 2021 J of Clinical MonitoringDocument5 pages2021 J of Clinical MonitoringAirwayNo ratings yet
- Supraglotic DivicesDocument5 pagesSupraglotic DivicesDavid OrtizNo ratings yet
- 6 - Surgical Management of The Difficult Adult AirwayDocument10 pages6 - Surgical Management of The Difficult Adult AirwayFer QuirozNo ratings yet
- Evaluation and Management of The Physiologically.16Document11 pagesEvaluation and Management of The Physiologically.16alveteNo ratings yet
- Principles and Practice of Lacrimal SurgeryFrom EverandPrinciples and Practice of Lacrimal SurgeryMohammad Javed AliNo ratings yet
- Advanced Techniques in Minimally Invasive and Robotic Colorectal SurgeryFrom EverandAdvanced Techniques in Minimally Invasive and Robotic Colorectal SurgeryOvunc BardakciogluNo ratings yet
- Computer ViruesDocument19 pagesComputer ViruesMuhammad Adeel AnsariNo ratings yet
- A Report On Kantajew MandirDocument21 pagesA Report On Kantajew MandirMariam Nazia 1831388030No ratings yet
- Unit 2 Water Treatment Ce3303Document18 pagesUnit 2 Water Treatment Ce3303shivaNo ratings yet
- Deutsche BankDocument4 pagesDeutsche BankMukesh KumarNo ratings yet
- Hotel Engineering Facilities: A Case Study of Maintenance PerformanceDocument7 pagesHotel Engineering Facilities: A Case Study of Maintenance PerformanceHoh Pui KeiNo ratings yet
- BED 101 Voc & Tech. Course ContentDocument3 pagesBED 101 Voc & Tech. Course ContentSunday PaulNo ratings yet
- Fujitsu Lifebook p1120 ManualDocument91 pagesFujitsu Lifebook p1120 Manualمحمد يحىNo ratings yet
- Quantification Skills in The Construction IndustryDocument34 pagesQuantification Skills in The Construction IndustryBRGRNo ratings yet
- My Watch Runs WildDocument3 pagesMy Watch Runs WildLarissa SnozovaNo ratings yet
- Password ManagementDocument7 pagesPassword ManagementNeerav KrishnaNo ratings yet
- 6 Construction of ShoeDocument33 pages6 Construction of ShoevedNo ratings yet
- Constructivism improves a lesson on nounsDocument6 pagesConstructivism improves a lesson on nounsOlaniyi IsaacNo ratings yet
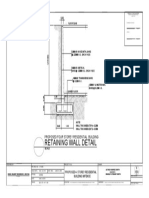
- Retaining Wall DetailsDocument1 pageRetaining Wall DetailsWilbert ReuyanNo ratings yet
- Optical Fiber Communication Case Study on Material DispersionDocument5 pagesOptical Fiber Communication Case Study on Material DispersionAyush SharmaNo ratings yet
- 6 An Indian American Woman in Space 2Document11 pages6 An Indian American Woman in Space 2Manju YadavNo ratings yet
- INSYS - EBW Serie EbookDocument4 pagesINSYS - EBW Serie EbookJorge_Andril_5370No ratings yet
- A Primer On Financial Time Series AnalysisDocument93 pagesA Primer On Financial Time Series AnalysisKM AgritechNo ratings yet
- Compare The Political System of Kazakhstan, USA, UK PresentationDocument19 pagesCompare The Political System of Kazakhstan, USA, UK PresentationAiganym OmiraliNo ratings yet
- Analects of A.T. Still-Nature Quotes-UnboundedDocument8 pagesAnalects of A.T. Still-Nature Quotes-UnboundedBruno OliveiraNo ratings yet
- bk978 1 6817 4068 3ch1Document28 pagesbk978 1 6817 4068 3ch1fysmaNo ratings yet
- LESSON 9 Steam Generators 2Document12 pagesLESSON 9 Steam Generators 2Salt PapiNo ratings yet
- 2014 01 RappTrans - Weight Sensors ReportDocument51 pages2014 01 RappTrans - Weight Sensors Reportsuraj dhulannavarNo ratings yet
- Henoch Schönlein PurpuraDocument12 pagesHenoch Schönlein PurpuraRavania Rahadian Putri100% (1)
- Phy Worksheet IG 3 Phase 2Document6 pagesPhy Worksheet IG 3 Phase 2Umair RazaNo ratings yet
- Lost Jar Action: WCP Slickline Europe Learning Centre SchlumbergerDocument19 pagesLost Jar Action: WCP Slickline Europe Learning Centre SchlumbergerMohsin PvNo ratings yet
- Winter's Bracing Approach RevisitedDocument5 pagesWinter's Bracing Approach RevisitedJitendraNo ratings yet
- 03 Authority To TravelDocument5 pages03 Authority To TravelDiana Marie Vidallon AmanNo ratings yet
- Financial ManagementDocument2 pagesFinancial ManagementSanna KazmiNo ratings yet