You might also like
- CookingDocument11 pagesCookingapi-603300265No ratings yet
- CookingDocument10 pagesCookingapi-603300265No ratings yet
- Doh Customer Satisfaction Survey Final VersionDocument2 pagesDoh Customer Satisfaction Survey Final Versionapi-603300265No ratings yet
- Outcomes StudyDocument1 pageOutcomes Studyapi-603300265No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CONTOH Surat Lamaran Kerja Bhs EngDocument10 pagesCONTOH Surat Lamaran Kerja Bhs Engboy5mil3No ratings yet
- The Angel Next Door Spoils Me Rotten - 01 (Yen Press)Document228 pagesThe Angel Next Door Spoils Me Rotten - 01 (Yen Press)Gilbert ValenzuelaNo ratings yet
- Electro-Diesels v6Document14 pagesElectro-Diesels v6Nuh AinuhaNo ratings yet
- Ingestable Robots: Presented By: Rakesh C N IV Sem McaDocument12 pagesIngestable Robots: Presented By: Rakesh C N IV Sem McaRamesh kNo ratings yet
- EMILE DURKHEIM On The Division of Labor in SocietyDocument23 pagesEMILE DURKHEIM On The Division of Labor in Societymalamati007100% (1)
- Class 7 Science July Monthly TestDocument3 pagesClass 7 Science July Monthly TestPugalmeena PugalmeenaNo ratings yet
- Ansible (DevOps)Document531 pagesAnsible (DevOps)air_jajaNo ratings yet
- Gratitude Journal 1Document50 pagesGratitude Journal 1Alesander Camacho100% (1)
- Newman's Apologia and The Drama of Faith and Reason - Draft5Document131 pagesNewman's Apologia and The Drama of Faith and Reason - Draft5Sancrucensis100% (6)
- Unleash The Warrior WithinDocument217 pagesUnleash The Warrior WithinIbis12100% (1)
- AP Eazy Tiled A4Document33 pagesAP Eazy Tiled A4Tanvir DaphedarNo ratings yet
- Bausa, Ampil, Suarez, Parades & Bausa For Petitioner. CV Law Office & Associates For Private RespondentsDocument32 pagesBausa, Ampil, Suarez, Parades & Bausa For Petitioner. CV Law Office & Associates For Private RespondentsChesza MarieNo ratings yet
- Naruto Coloured Volume 06Document175 pagesNaruto Coloured Volume 06kian.kdlmNo ratings yet
- Logistics Processes and Practices: Ms. Sebonkile ThabaDocument27 pagesLogistics Processes and Practices: Ms. Sebonkile ThabapercyNo ratings yet
- Dialight CE Catalogue 2016 2Document60 pagesDialight CE Catalogue 2016 2KABRENo ratings yet
- Communication Networks in Organisations PDFDocument2 pagesCommunication Networks in Organisations PDFDevin100% (1)
- TF23 - DCYF Meet Program Morning (4x800m, Consolation, Field Events)Document15 pagesTF23 - DCYF Meet Program Morning (4x800m, Consolation, Field Events)Ryan Raposo0% (1)
- SK Itinerary Travel Travel Order Travel CompletedDocument3 pagesSK Itinerary Travel Travel Order Travel CompletedAntonette Frilles GibagaNo ratings yet
- Woman and TaxDocument7 pagesWoman and TaxMeita LarasatiNo ratings yet
- Error Analysis Interlanguage PDFDocument2 pagesError Analysis Interlanguage PDFNancyNo ratings yet
- Posting+0051-2023 +Resolution+No +01,+series+of+2023+ (E) + (HVB+SGD)Document6 pagesPosting+0051-2023 +Resolution+No +01,+series+of+2023+ (E) + (HVB+SGD)Carolyn VillagraciaNo ratings yet
- Language Analysis Part 1: The BasicsDocument20 pagesLanguage Analysis Part 1: The BasicsLevi LiuNo ratings yet
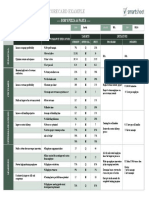
- IC Restaurant Balanced Scorecard ExampleDocument1 pageIC Restaurant Balanced Scorecard Examplemuscdalife100% (1)
- Diff n2 HL - SL Vid PDFDocument21 pagesDiff n2 HL - SL Vid PDFfayekoNo ratings yet
- Itr2 - 2019 - PR2 JPDocument89 pagesItr2 - 2019 - PR2 JPvenkateshbitraNo ratings yet
- The Meaning of The HousesDocument15 pagesThe Meaning of The HousesAnnie ToriNo ratings yet
- SAP Human Resources: Priya AroraDocument24 pagesSAP Human Resources: Priya AroraSARITANo ratings yet
- Communal LandDocument17 pagesCommunal Landermias dersehNo ratings yet
- Strategist 14Document159 pagesStrategist 14Namrit ZatakiyaNo ratings yet
- Insurance Analysis ReportDocument12 pagesInsurance Analysis ReportMazharul KarimNo ratings yet